
Top 5 Reasons Medical Claims Get Denied in 2026 — And Exactly How to Fix Each One
If that sentence feels familiar, you are not alone — and you are not unlucky. In 2024, initial claim denial rates across the US healthcare system hit 11.8 percent, according to industry data tracked by Experian Health. For Medicare Advantage plans specifically, that number climbed to 15 to 17 percent. And a full 60 percent of medical group leaders reported that their denial rates were increasing compared to the prior year, according to MGMA.
Here is the part that should really bother you: between 60 and 90 percent of denied claims result from avoidable front-end errors — not clinical disputes with insurers. That means most denials are not a fight you need to win. They are a workflow problem you need to fix.
This guide covers the top 5 reasons medical claims get denied in 2026, the real statistics behind each one, and the specific, actionable steps your practice can take to prevent them — and recover the ones that have already hit your AR.
Why Claim Denial Rates Keep Rising in 2026
Before diving into the top 5 causes, it helps to understand what is driving the broader trend.
According to KFF’s analysis of ACA marketplace claims, two-thirds of insured adults in a January 2026 poll believe delays and denials of healthcare services are a “major problem.” One-third report having a claim denied in the past two years. Meanwhile, the American Journal of Managed Care reports that insurance claim denials have risen 16 percent from 2018 to 2024 — with no sign of reversal.
What is driving it? Three forces are colliding in 2026:
Payer AI automation. Many insurers now use automated tools to review and deny claims at high volume. These systems flag documentation gaps, coding inconsistencies, and authorization mismatches faster than any human reviewer — which means errors that previously slipped through are now being caught and denied at scale.
Expanding prior authorization requirements. Insurers increasingly require pre-approval for services that previously did not need it. Failing to secure authorization in time is now one of the fastest-growing denial reasons across all payer types.
Staffing pressure on billing teams. Healthcare organizations continue to face shortages of experienced coders and revenue cycle specialists — leading to more intake errors, coding mistakes, and missed authorization requirements.
The administrative cost per denied claim increased from $43.84 in 2022 to $57.23 in 2023. For a practice generating 50 denials per month, that is over $34,000 per year in administrative rework cost alone — before counting the revenue that never gets recovered.
Reason #1 — Missing or Inaccurate Patient Data at Intake
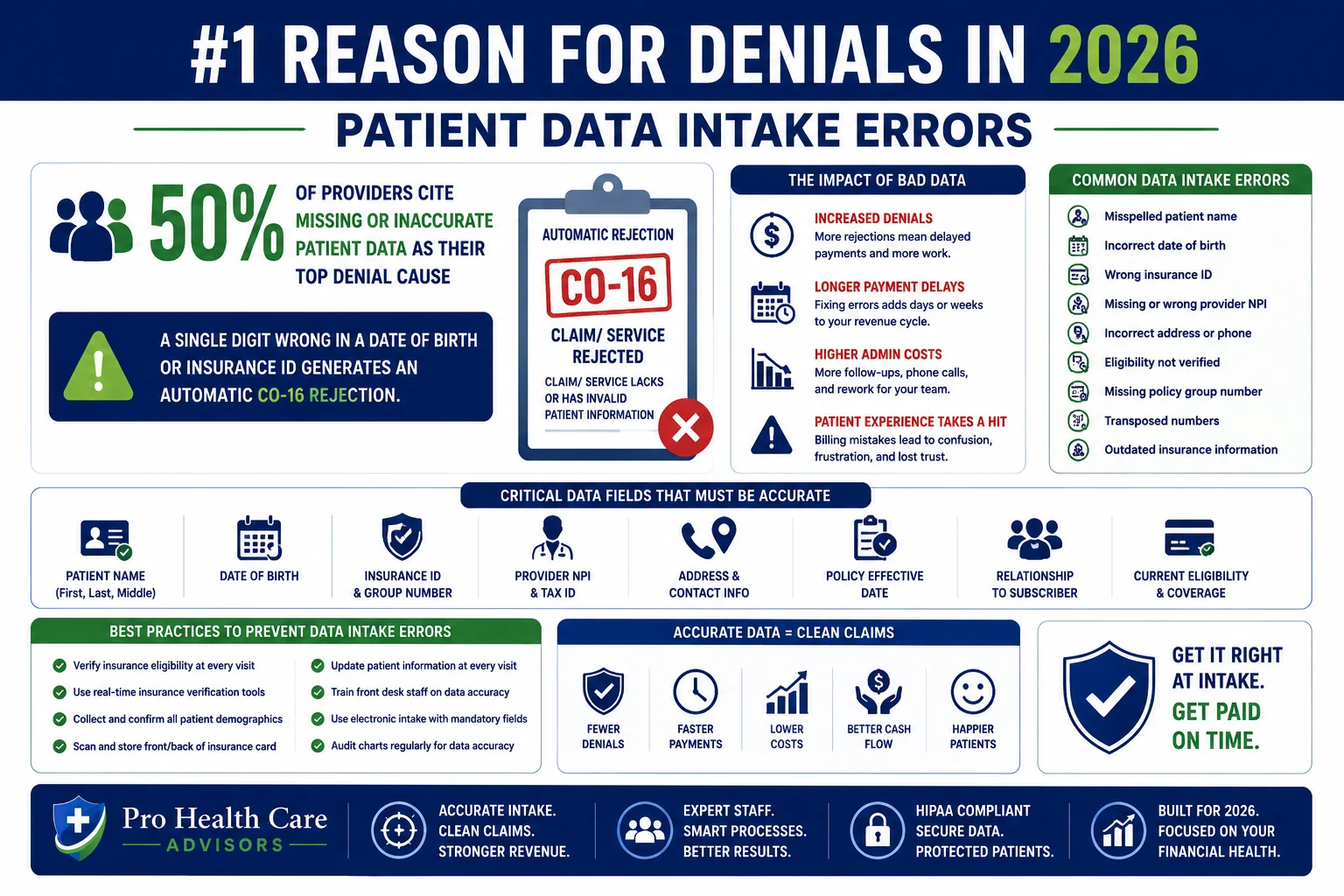
The stat: According to Experian Health’s State of Claims report, 68 percent of survey respondents say denials often stem from incorrect or incomplete patient information collected during intake. A separate analysis found that more than 25 percent of all claim denials trace back to simple data entry errors at registration.
What it looks like: A transposed digit in a date of birth. An insurance ID entered from an expired card. A misspelled patient name. A group number that changed when the patient’s employer renewed their plan in January. Any of these generates a CO-16 denial — “claim/service lacks information or has incorrect information” — and every one of them is entirely preventable.
Why it keeps happening: Front desk staff are juggling check-in, phone calls, patient questions, and a waiting room full of people. In that environment, data entry errors happen. What separates high-performing practices from struggling ones is not whether errors occur — it is whether there is a process to catch them before the claim goes out.
The fix:
First, verify insurance information at every visit — not just at the patient’s first appointment. Insurance changes constantly. A patient whose plan was correct in March may have a different group number, payer, or plan type in June. Real-time eligibility verification before every encounter catches these changes before they become denials.
Second, scan insurance cards and photo ID at every visit rather than relying on manually entered information. OCR-enabled scanning significantly reduces the transcription errors that generate CO-16 denials.
Third, implement pre-submission claim scrubbing that flags demographic mismatches before the claim leaves your system. Our medical billing and practice management services run eligibility verification and claim scrubbing as standard steps before every submission — maintaining a 98.5 percent clean claim rate specifically because errors like these are caught upstream.
For a detailed breakdown of what CO-16 and other denial codes mean and what to do when you see them, see our complete medical billing denial codes guide.
Reason #2 — Prior Authorization Errors and Gaps
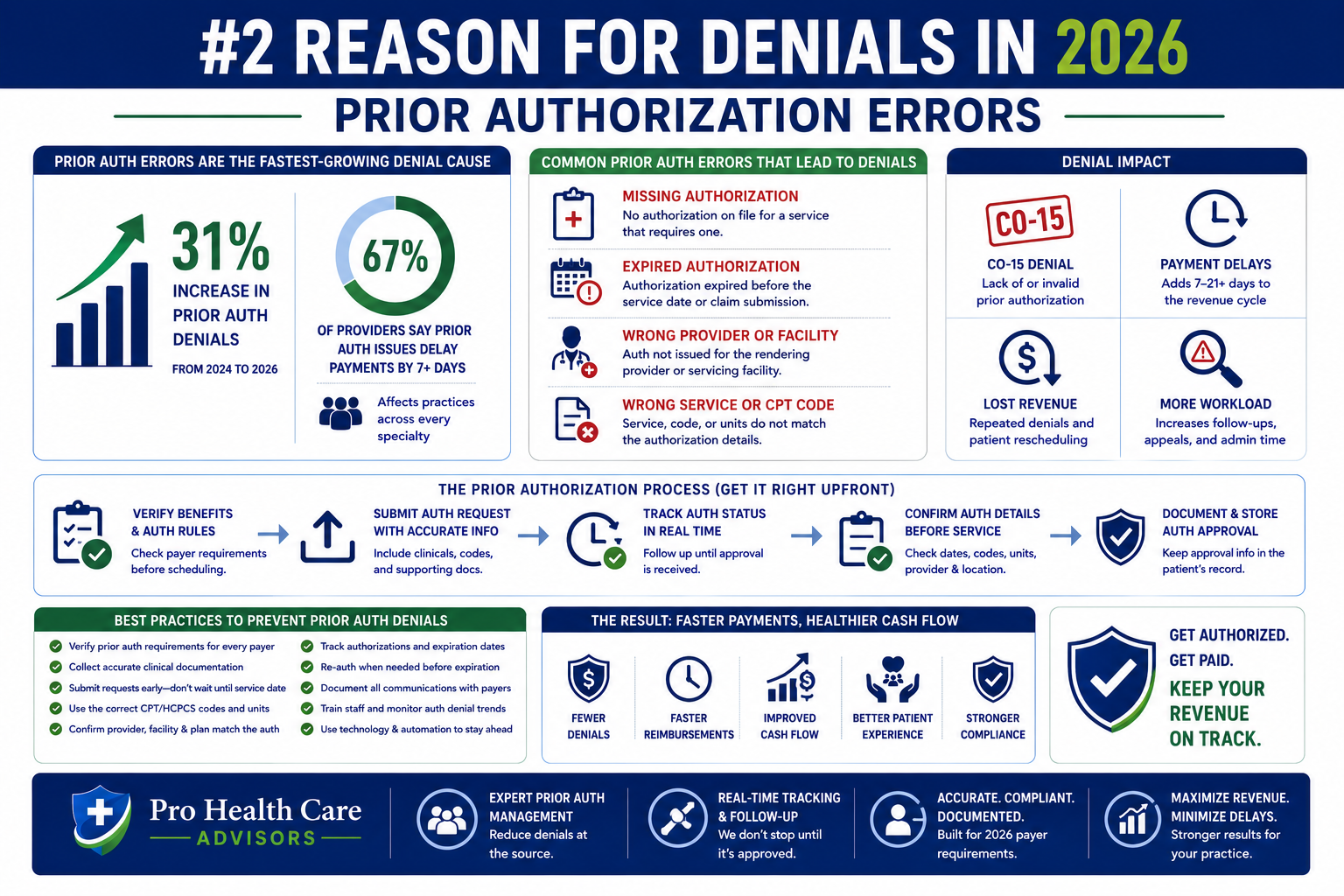
The stat: Prior authorization failures are now one of the fastest-growing denial reasons across all payer types. According to the American Medical Association, physicians spend an average of 14.5 hours per week on prior authorization — and even with that time investment, CO-15 denials (authorization missing or invalid) remain among the most common on EOBs nationwide.
What it looks like: A service is rendered. A claim is submitted. The payer denies it with CO-15 — “the authorization number is missing, invalid, or does not apply to the billed service.” Sometimes the authorization exists but was entered incorrectly on the claim. Sometimes it was obtained for a slightly different service code. Sometimes it simply was not obtained at all because a staff member assumed it was not required for that payer.
Why it keeps happening in 2026: Payers have dramatically expanded their prior authorization requirements. Services that did not require authorization two years ago now do. And with the CMS-0057-F prior authorization rule taking effect in January 2026, the rules around authorization timelines and denial explanations changed again — creating another round of workflow adjustments that underprepared practices have not yet made.
The fix:
Build a prior authorization tracking workflow — not a manual spreadsheet checked inconsistently, but a systematic process that identifies authorization requirements by payer and service type before scheduling, confirms authorization status before every procedure, and flags upcoming authorization expirations before they lapse.
The CMS-0057-F rule requires standard authorization decisions within 7 calendar days and urgent decisions within 72 hours — down from previous standards. Submit complete, documentation-ready requests on the first submission because payer decision windows are now tighter than before.
For the complete 2026 prior authorization rule picture and how it affects your practice, read our prior authorization rules changed 2026 guide.
Reason #3 — Insurance Eligibility Verification Failures
The stat: According to data from Healthsurehub’s claims denial analysis, a significant portion of claim denials — estimated at more than 25 percent — trace back to eligibility failures. These are the OA-23 denials (patient not enrolled on date of service) and CO-22 denials (another payer may be primary) that appear when a claim is submitted to the wrong payer or for a patient who was not covered on the date of service.
What it looks like: A patient presents their UnitedHealthcare card. Your front desk verifies the card is current and checks the patient in. Three weeks later, a denial arrives showing that the patient switched to a new employer health plan on the first of the month — and the UnitedHealthcare plan was terminated. Or the patient has secondary coverage that makes Medicare primary — and the claim went to Medicare when it should have gone to an employer plan first.
Why it keeps happening: In 2026, insurance changes happen constantly. According to the Kaiser Family Foundation, 38 percent of ACA marketplace plans available in 2026 were not available in 2024. The marketplace disruption — combined with employer plan renewals, Medicare Advantage enrollment changes, and Medicaid redeterminations — has created a period of unusually high insurance instability. Stored eligibility data from a patient’s last visit is frequently wrong.
The fix:
Run real-time eligibility verification before every appointment — not at the patient’s last visit, not at check-in from a stored record, but live, in real time, on the morning of every appointment. This catches plan changes, terminations, coordination of benefits issues, and carve-out routing requirements before they become denials.
Eligibility verification should go beyond confirming that coverage exists. It should confirm the specific plan type, the effective date, the group number, deductible status, and whether mental health or other specialty benefits are managed by a separate entity. A patient whose general medical insurance is Blue Shield but whose behavioral health benefits are managed by Optum will generate a denial if the mental health claim goes to Blue Shield.
Our revenue cycle management services include real-time eligibility verification as a standard step before every patient encounter — eliminating the OA-23 and CO-22 patterns that eligibility failures generate.
Reason #4 — ICD-10 Coding Errors and Medical Necessity Failures
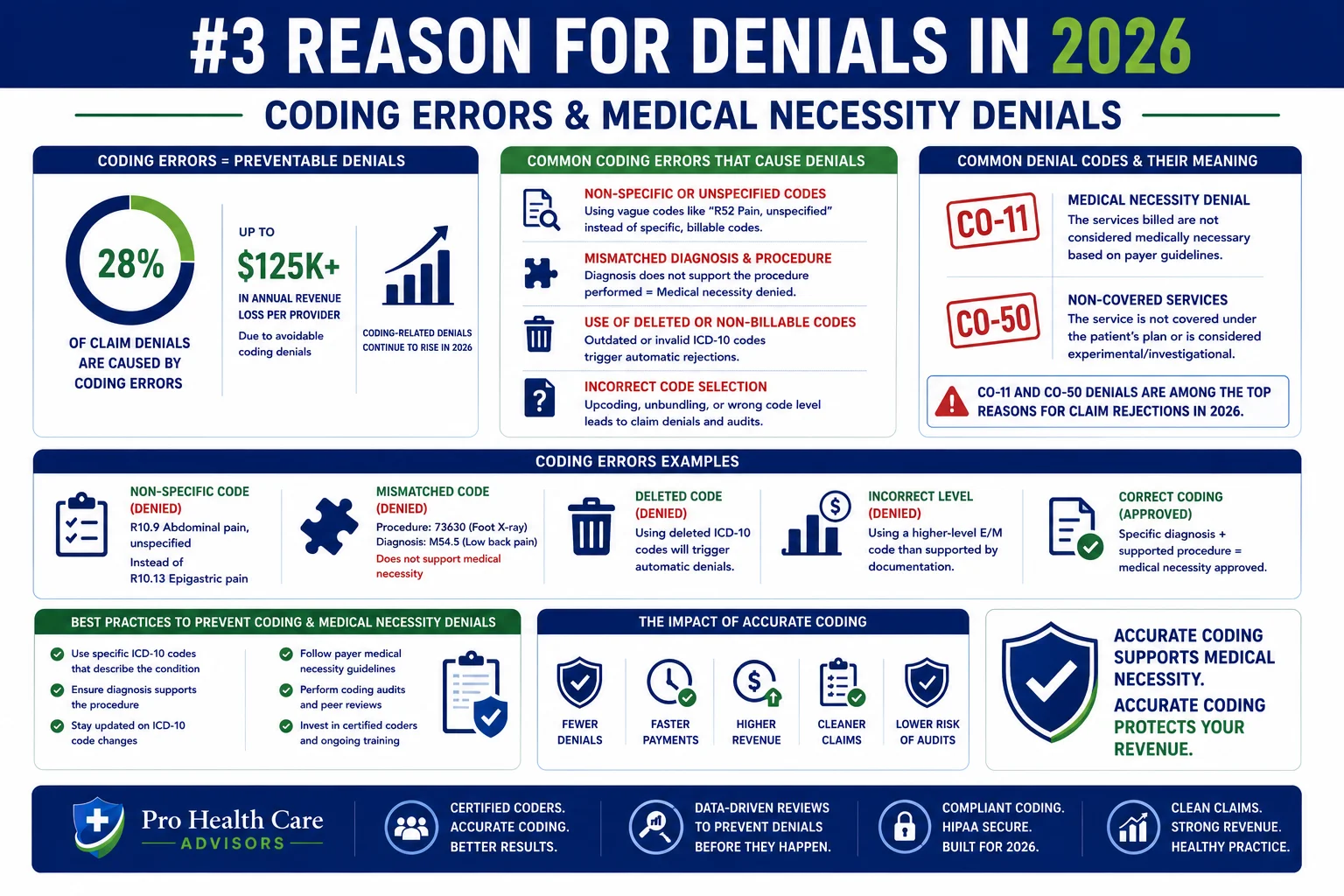
The stat: According to Medicotech’s 2026 denial analysis, ICD-10 coding errors — including use of newly deleted codes, non-specific diagnosis codes, and mismatched procedure-diagnosis combinations — are one of the top five denial causes in 2026. The OIG has identified approximately 61 percent of mental health Medicare claims as containing some type of coding or documentation error.
What it looks like: A CO-11 denial — “the diagnosis code does not support medical necessity for this service” — appears when the ICD-10 code submitted does not justify the procedure billed. A CO-50 denial — “medical necessity not established” — appears when the clinical documentation does not support the billed service even if the code is correct. And with 84 CPT codes deleted in the 2026 update, claims submitted with deleted codes generate automatic rejections before adjudication even begins.
Why it keeps happening: ICD-10 requires specificity — and non-specific codes are one of the most common coding errors. A provider who documents “chest pain” without specifying the type, location, and acuity will generate a code that is too vague to support specific cardiac procedures. A 2026 CPT code deletion that billing teams have not caught will generate rejections on every claim containing that code until someone identifies the pattern.
The fix:
Conduct a coding audit of your top 20 most-billed CPT and ICD-10 code combinations. Identify any codes deleted in the 2026 update that your practice is still using — our CPT code changes 2026 guide covers all 84 deletions and the replacement codes for each.
Train providers on ICD-10 specificity requirements for their specialty. The most common medical necessity denials trace back to documentation — providers who document at a general level when payers require specific functional limitations, acuity markers, and treatment rationale.
For CO-50 medical necessity denials specifically, appeals should include the full clinical record, the provider’s documented rationale for the service, and references to applicable clinical guidelines. A specific denial reason is something you can challenge — which is why the 2026 CMS rule requiring specific denial explanations is actually an advantage for practices with strong clinical documentation.
Our CodeMAXX services review coding accuracy before submission — catching the diagnosis-procedure mismatches that generate CO-11 and CO-50 denials, and identifying undercoding patterns that reduce net collections without generating visible denials.
Reason #5 — Lack of Medical Necessity Documentation in Clinical Notes
The stat: According to data from Experian Health, 68 percent of providers say submitting clean claims is harder than a year ago — and documentation gaps are a primary driver. Medical necessity documentation failures generate CO-50 denials that are among the hardest to overturn after the fact because the clinical record does not support the appeal.
What it looks like: A service is coded correctly. The authorization is in place. The patient’s insurance is current. But the clinical note does not clearly document why this patient needed this service on this date — and the payer’s AI-driven review system flags it as lacking medical necessity justification.
This is increasingly common as payers deploy automated utilization review systems that analyze documentation patterns at scale. A progress note that says “patient doing well, continue current treatment” is not medical necessity documentation. It is a billing vulnerability.
Why it keeps happening: Documentation requirements have increased significantly in 2026. Payers now require greater depth of clinical justification — documented symptom severity, functional impairment, treatment response, and rationale for continuing or changing treatment. Many providers are documenting at the level that was sufficient two or three years ago, without realizing that payer standards have shifted.
The fix:
Educate providers on what payers are looking for in medical necessity documentation for your specialty. In behavioral health, this means session-specific symptom severity, functional impairment data, and documented progress toward treatment goals. In cardiology and orthopedics, it means documented functional limitations, prior treatment attempts, and clinical rationale for the recommended service.
Build documentation templates that guide providers to include the elements that support medical necessity — not as a bureaucratic exercise, but as clinical documentation that accurately reflects the complexity of the care delivered.
When CO-50 denials arrive despite good documentation, build a structured appeal process that includes the complete clinical record, the provider’s explicit medical necessity statement, and references to applicable clinical guidelines. According to KFF research, 57 percent of denied Medicare Advantage claims are overturned on appeal — meaning most medical necessity denials are winnable with the right documentation and the right appeal language.
For a complete walkthrough of how to appeal medical necessity denials, see our medical billing denial codes guide.
Bonus: The Pattern Nobody Talks About — Denial Abandonment
Here is the number that is more alarming than the denial rate itself: approximately 60 percent of denied claims are never resubmitted or appealed. They are simply written off.
For a practice generating $200,000 per month in claims with a 12 percent denial rate, that is $24,000 in denied claims per month — and $14,400 of it is being written off without a fight.
The reason most practices abandon denials is not that the claims are unwinnable. It is that no one has time to work them. The billing team is managing incoming claims, posting payments, handling patient calls, and running eligibility checks. Denial appeals fall to whoever has a free hour — which is never.
The fix for denial abandonment is not working harder. It is building a structured denial management workflow with categorization, prioritization, and appeal tracking — so that every denied claim gets a response before the appeal window closes.
Our creative collection solutions are specifically built around this kind of structured denial recovery — including aged claims from previous billing periods that other billing teams have given up on.
How Pro Health Care Advisors Prevents All 5 Denial Types

Every one of the top 5 denial causes covered in this guide is addressable with the right billing process. Here is specifically how Pro Health Care Advisors prevents each one:
Intake data errors (Reason 1): Real-time insurance eligibility verification before every appointment, combined with pre-submission claim scrubbing that catches demographic errors before the claim leaves our system.
Prior authorization failures (Reason 2): Systematic PA tracking by payer and service type, with proactive follow-up on pending authorizations and electronic submission through payer-specific ePA systems.
Eligibility verification failures (Reason 3): Live eligibility checks on the morning of every appointment across our client base — not stored eligibility data from the patient’s last visit.
Coding errors and medical necessity failures (Reason 4): AAPC-certified coders review every claim for ICD-10 specificity, procedure-diagnosis alignment, deleted code usage, and modifier accuracy before submission. Our CodeMAXX services add a dedicated coding accuracy layer.
Documentation failures (Reason 5): We work with clinical teams to ensure that documentation templates capture the elements payers require for medical necessity — and when CO-50 denials arrive, our structured appeal process uses the clinical record and guideline references to achieve overturn rates well above the industry average.
The result: a 98.5 percent clean claim rate and a denial rate under 2 percent — compared to the national average of 11.8 percent.
We serve more than 30 specialties including cardiology, mental health, family practice, and wound care.
Frequently Asked Questions — Reasons Medical Claims Get Denied
Q: What is the number one reason medical claims get denied in 2026? Missing or inaccurate patient data at intake — cited by 50 percent of providers as their top denial cause — generates more denials than any other single factor. A single digit wrong in a date of birth or insurance ID generates an automatic CO-16 rejection that requires correction, resubmission, and processing time that delays payment.
Q: What percentage of medical claims are denied in 2026? Initial denial rates hit 11.8 percent nationally in 2024 and continued rising into 2026. For Medicare Advantage plans, the rate runs 15 to 17 percent. For ACA marketplace plans, some insurers deny 20 percent or more of in-network claims. According to Experian Health, 41 percent of providers now see at least one in ten claims denied.
Q: What percentage of denied claims are overturned on appeal? Studies show that 57 percent of denied Medicare Advantage claims are overturned on appeal — meaning more than half of the denials your practice is absorbing could be recovered with a proper appeal. The problem is that 60 percent of denied claims are never resubmitted at all.
Q: How do I find out why a specific claim was denied? The Explanation of Benefits (EOB) or Electronic Remittance Advice (ERA) contains a Claim Adjustment Reason Code (CARC) that identifies the denial reason. Our complete denial codes guide covers every major CARC — CO, PR, and OA codes — with plain-language explanations and exact fix steps for each.
Q: What is a CO-16 denial and how do I fix it? CO-16 means the claim is missing required information or contains incorrect information. The payer’s remittance usually includes a Remittance Advice Remark Code (RARC) that identifies the specific field. Correct the identified error and resubmit as a corrected claim. Common CO-16 causes include missing NPI, incorrect date of birth, invalid CLIA number, and mismatched place of service.
Q: How does prior authorization affect claim denial rates? Prior authorization failures generate CO-15 denials — one of the most common and most preventable denial types. With the 2026 CMS-0057-F rule requiring standard PA decisions within 7 days, practices that submit complete, accurate authorization requests upfront will see fewer CO-15 denials than those still using fax-based or incomplete PA workflows.
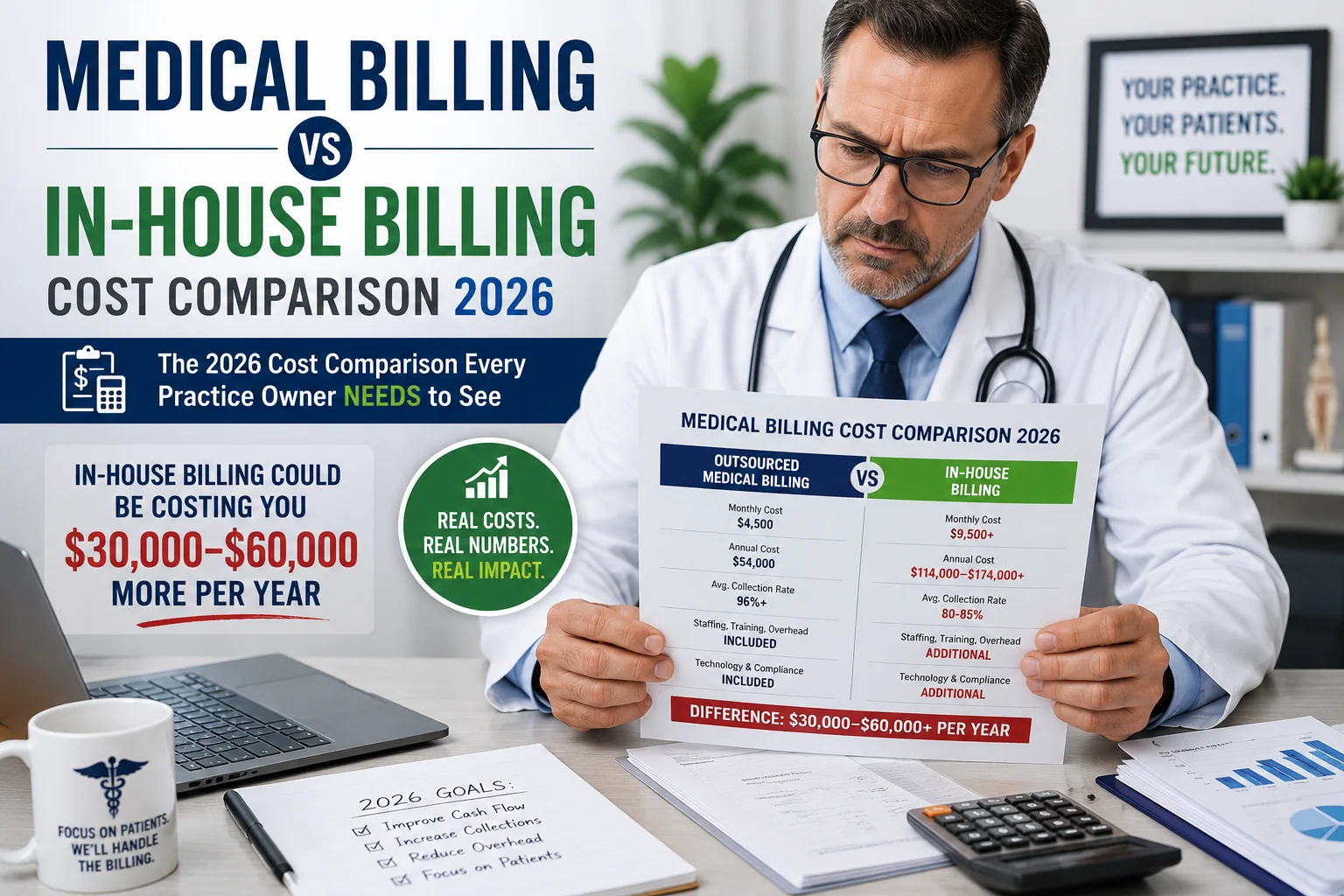
Q: Should I outsource billing to reduce claim denials? For most practices — particularly those with denial rates above 8 percent — yes. Outsourced billing partners with structured denial prevention workflows, real-time eligibility systems, and AAPC-certified coders consistently outperform in-house billing teams on clean claim rates and denial rates. Read our complete comparison: In-House vs Outsourced Medical Billing.

The Bottom Line — Most Denials Are Preventable, Not Inevitable
Claim denial rates are rising. But rising denial rates are not a law of nature — they are the predictable result of billing processes that have not kept pace with payer complexity.
Between 60 and 90 percent of denied claims result from avoidable front-end errors. The top 5 causes in this guide — intake data errors, prior authorization failures, eligibility verification misses, coding mistakes, and documentation gaps — are all workflow problems with specific, implementable solutions.
The practices collecting the most revenue in 2026 are not seeing fewer denials because they are lucky. They have built billing processes that prevent denials at the source — real-time eligibility verification, systematic prior authorization tracking, AAPC-certified coding review, and pre-submission scrubbing that catches errors before they reach the payer.
Pro Health Care Advisors builds exactly those processes for practices across more than 30 specialties — with a 98.5 percent clean claim rate and a denial rate under 2 percent as the measurable result.
If your practice’s denial rate is above 5 percent — or if you do not know what your denial rate is — that gap is costing you money every single month.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pressure. No pitch. Just a real look at where your claims are failing and exactly what it would take to fix them.