CPT CODE CHANGES 2026 — WHAT EVERY MEDICAL PRACTICE MUST KNOW RIGHT NOW
Every January 1st, the rules change.
New CPT codes take effect. Old ones get deleted. Some get revised in ways that look minor on paper but create major billing problems if your team does not know about them. And every year, practices that are not prepared walk into the new year submitting claims with outdated codes — generating denials they do not understand, undercollecting on services they delivered, and spending months cleaning up a mess that better preparation would have prevented entirely.
2026 is not a small update year. Not even close.
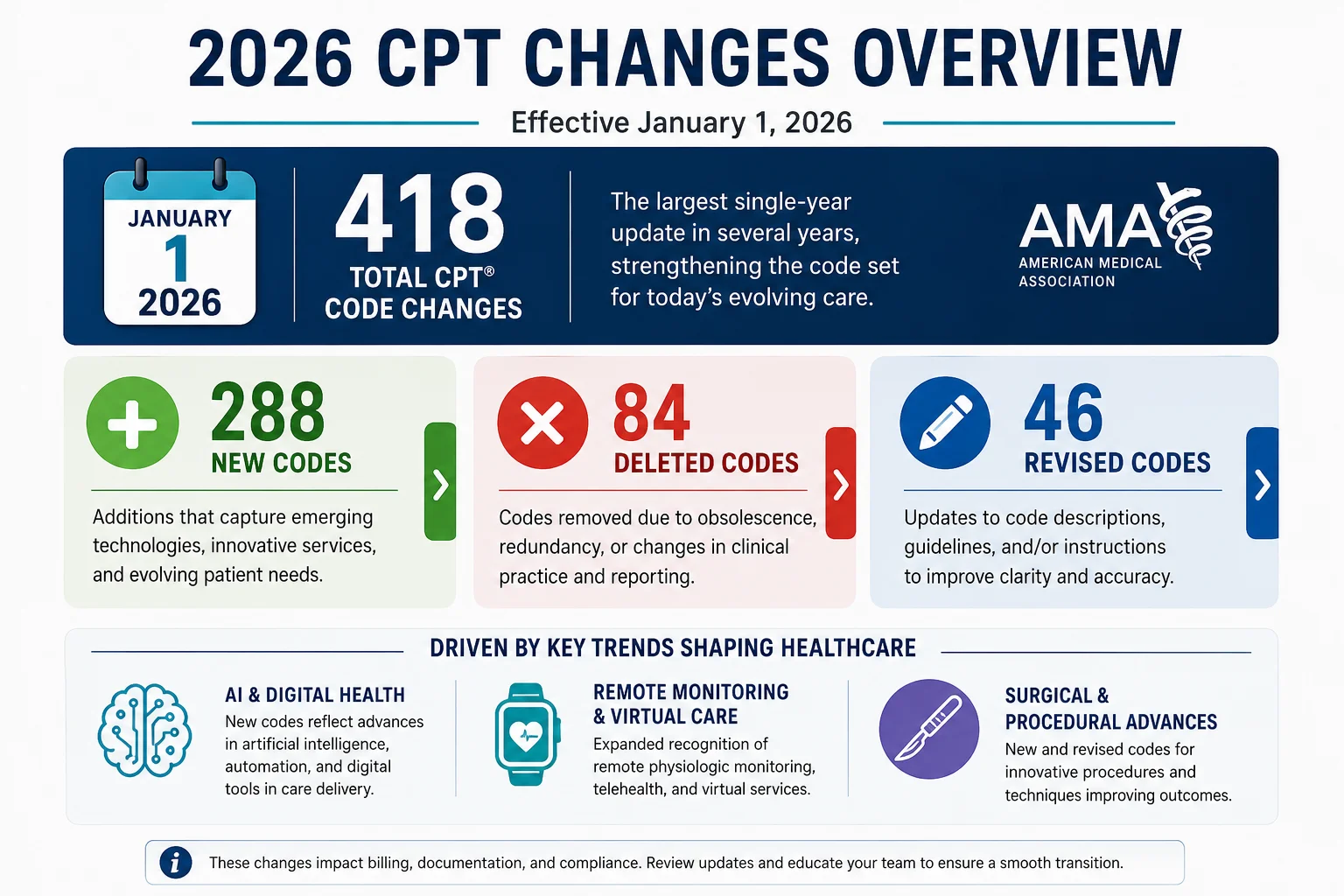
<cite index=”45-1″>The 2026 CPT code set includes 418 total changes — 288 new codes, 84 deletions, and 46 revisions</cite> — reflecting significant advances in digital health, artificial intelligence, remote patient monitoring, and minimally invasive surgery. <cite index=”47-1″>The updates reflect technological advancements and evolving care delivery models, particularly the shift toward outpatient settings.</cite>
This guide covers every major CPT code change in 2026 that affects medical practice billing — by category, with specific code numbers, plain-language explanations, and what your billing team needs to do right now if they have not already. Whether you run a primary care office, a cardiology group, an audiology practice, or a vascular surgery center — something in this year’s update affects you.
Why CPT Code Changes in 2026 Matter More Than Usual
Every year has CPT updates. But not every year has 418 of them.
<cite index=”49-1″>The 2026 update represents more than an annual refresh.</cite> It signals a structural shift in how the American Medical Association is categorizing clinical services — particularly in three areas that are reshaping how care is delivered and how practices get paid:
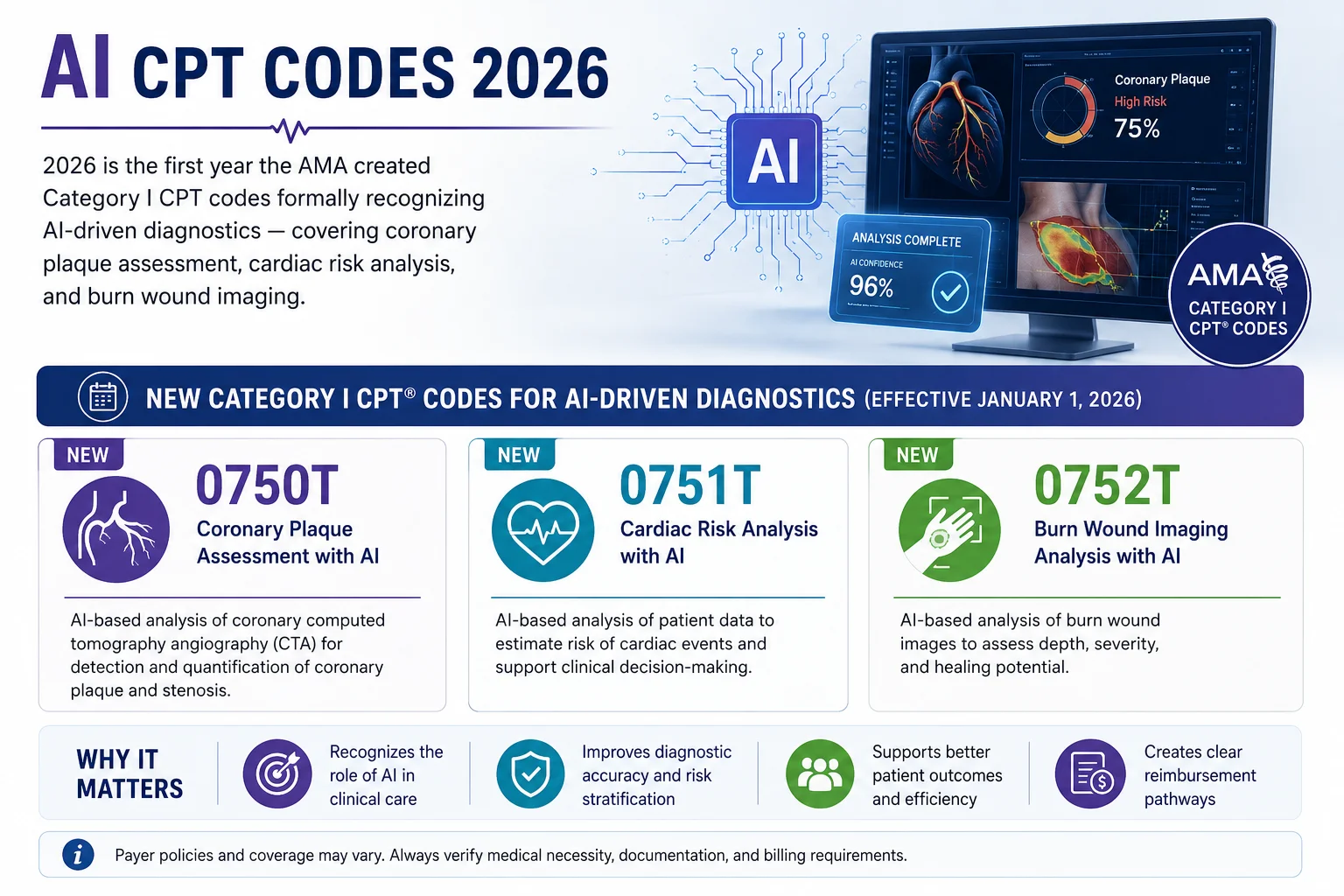
Artificial Intelligence in Clinical Decision-Making. For the first time, the CPT code set includes Category I codes that formally recognize AI as a standard tool in clinical care — not just an experimental add-on. Practices using AI-driven diagnostic tools now have proper billing codes for those services.
Remote Patient Monitoring Expansion. The 2026 update significantly expands RPM coding to cover shorter monitoring periods, new device categories, and initial treatment management — creating new revenue opportunities for practices that monitor patients outside the clinical setting.
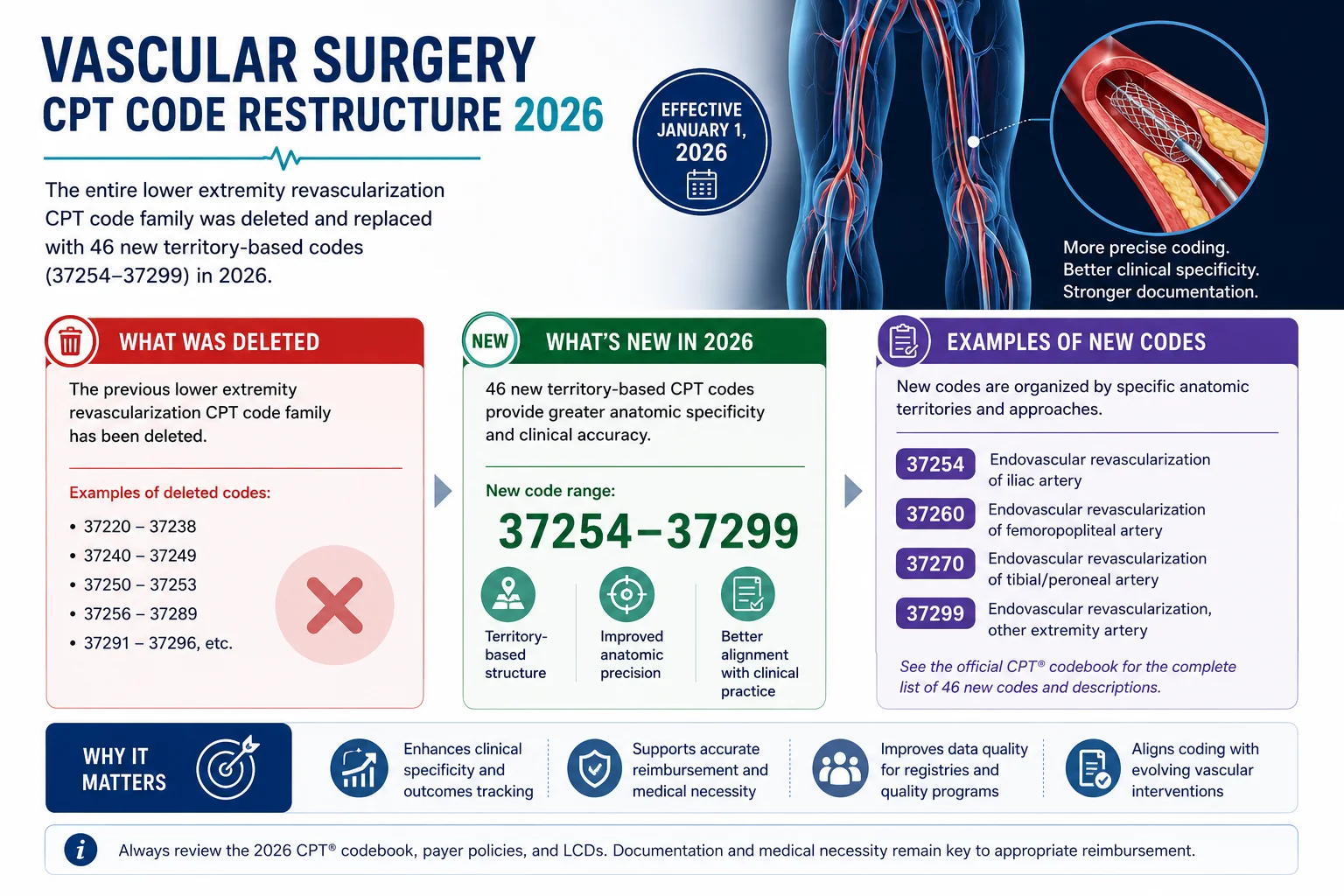
Surgical Code Restructuring. The lower extremity revascularization section was completely rebuilt. <cite index=”45-1″>The AMA has deleted previous codes and replaced them with 46 territory-based codes (37254–37299).</cite> Practices in vascular surgery and interventional cardiology that are still using the old codes are generating automatic denials on every claim in this category.
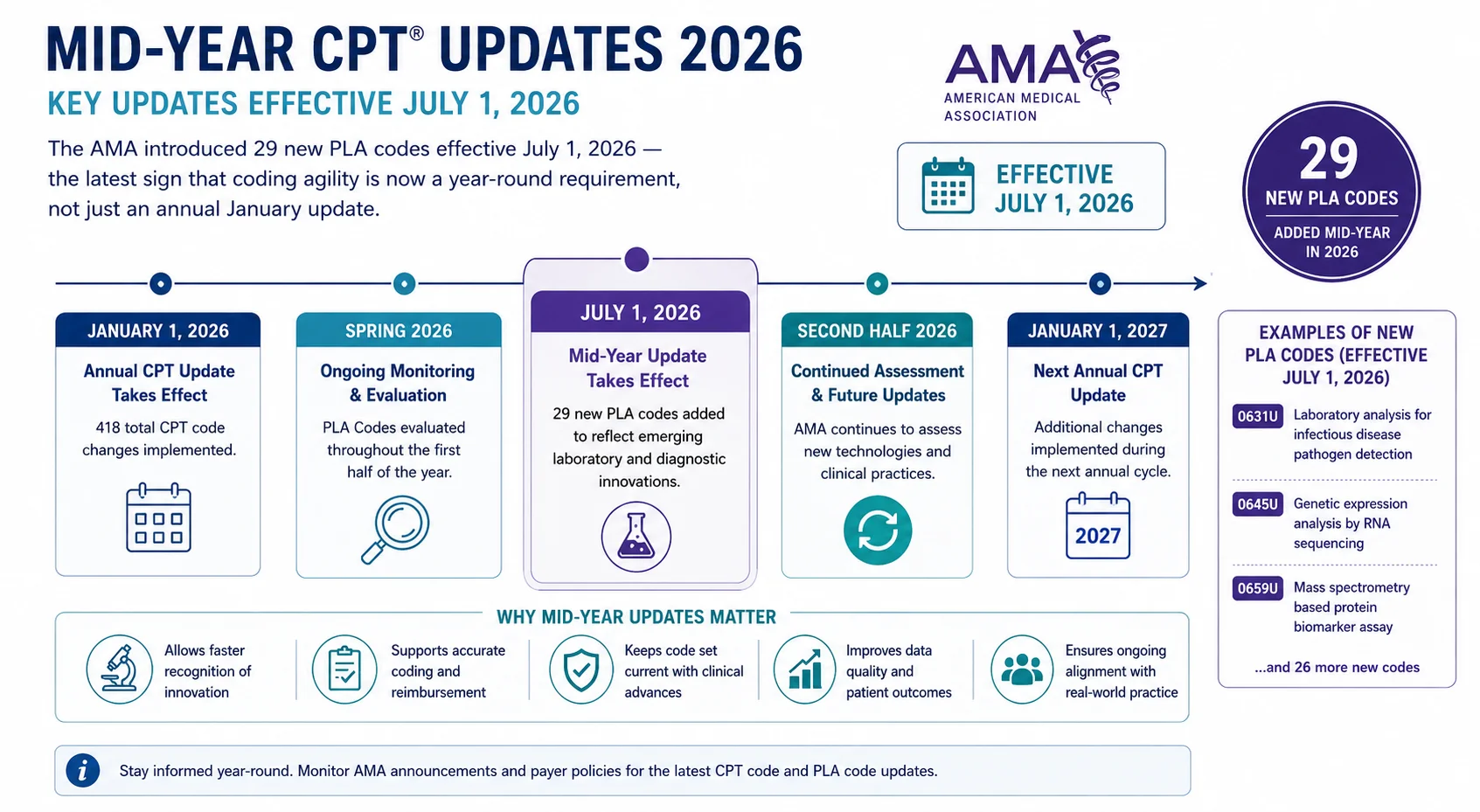
And there is one more layer added in mid-2026: <cite index=”52-1″>effective July 1, 2026, the AMA introduced 29 new PLA codes (0631U–0659U), 2 revised codes, and 4 deleted codes</cite> — meaning the update cycle did not stop at January 1. Practices need to monitor mid-year releases as well.
According to the American Medical Association, these updates are designed to ensure that the CPT code set accurately reflects modern clinical practice. For your billing team, that means one thing: if your codes have not been updated, your reimbursements are not reflecting modern reality either.
The Biggest CPT Code Changes in 2026 — By Category
1. Remote Patient Monitoring (RPM) — New and Revised Codes
Remote patient monitoring has been one of the fastest-growing billing categories since the telehealth expansions of 2020 — and the 2026 CPT update significantly expands what practices can bill for.
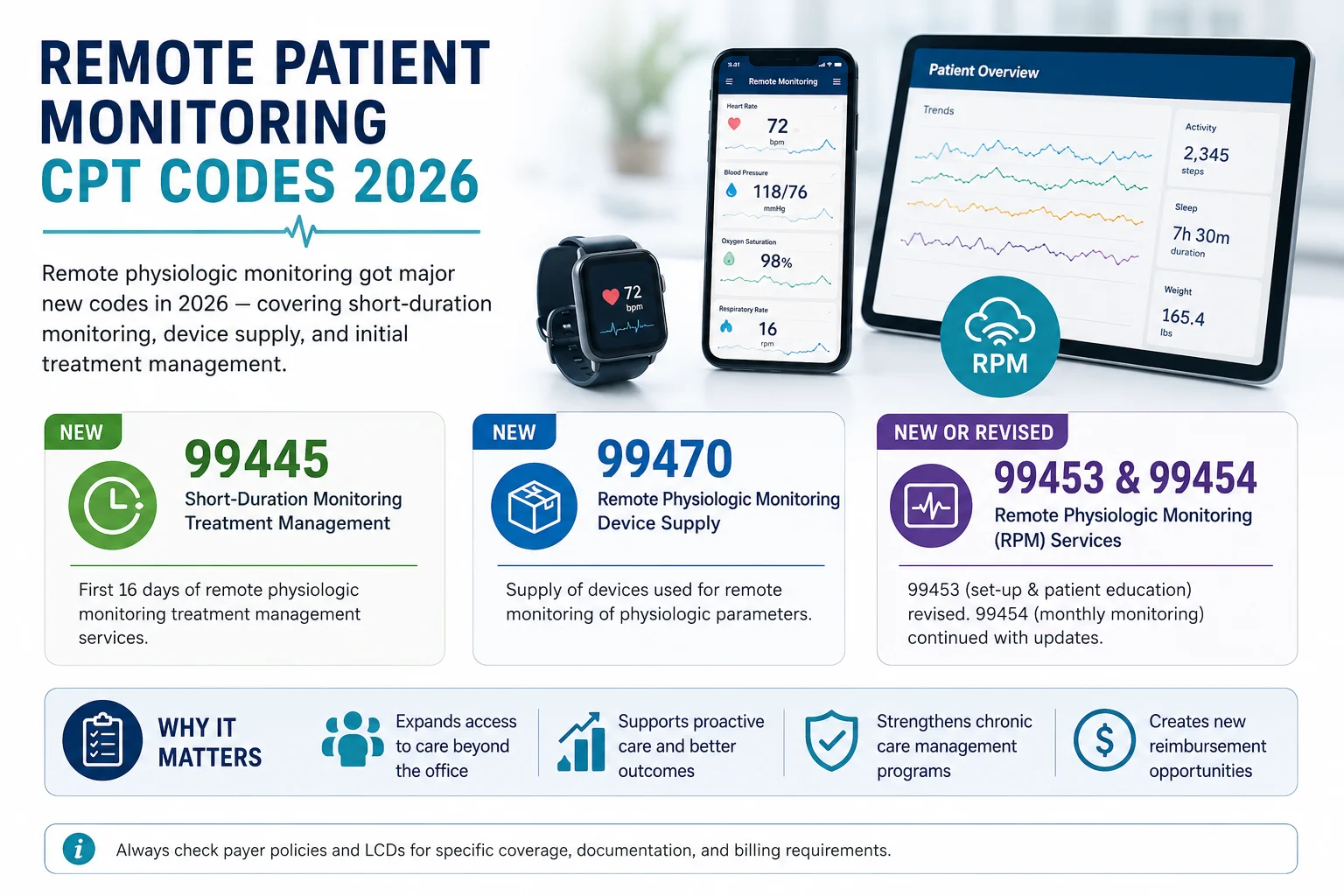
<cite index=”45-1″>Code descriptors for remote physiologic monitoring (99453, 99454) have been revised, and new codes (99445, 99470) have been added to cover device supply and initial treatment management.</cite>
Here is what changed and what it means:
99453 (Revised) — Remote monitoring of physiologic parameter(s) — setup and patient education. The descriptor has been updated to clarify which device types and service components qualify. Practices need to verify their documentation templates align with the revised definition.
99454 (Revised) — Device supply with daily recordings or programmed alert transmissions. Revised to clarify the 16-day minimum monitoring period requirement that determines when this code can be billed in a 30-day cycle.
99445 (New) — A new code specifically covering device supply for shorter-duration RPM periods. <cite index=”49-1″>New codes for short-duration remote physiologic monitoring (RPM) over 2–15 days within a 30-day period</cite> now have dedicated billing codes — meaning practices that were previously unable to bill for monitoring episodes under 16 days now have a proper code for those services.
99470 (New) — Initial treatment management for remote physiologic monitoring. This new code captures the clinical time involved in reviewing RPM data and initiating a treatment change — a billable service that many practices were delivering without a proper code to capture it.
What your billing team needs to do: Update your RPM billing workflows to reflect the revised 99453 and 99454 descriptors. Begin using 99445 for monitoring episodes of 2 to 15 days. Add 99470 to your charge capture for initial treatment management activities tied to RPM data review. Verify your documentation templates support these revised definitions.
2. Artificial Intelligence Diagnostic Services — New Category I Codes
This is the most historically significant category in the 2026 update — and the one that is getting the least attention from most billing teams.
<cite index=”45-1″>Recognizing the growing role of technology in diagnosis, the new code set includes Category I codes for AI-driven services. These codes cover augmentative software analysis for conditions such as coronary atherosclerotic plaque assessment, perivascular fat analysis for cardiac risk, and multispectral imaging for burn wounds. These additions validate AI as a standard tool in clinical decision-making.</cite>
Why does this matter for billing? Category I CPT codes are the codes that payers actually reimburse. Previously, AI-driven diagnostic analyses existed in Category III — experimental and research codes that most payers do not cover. Moving these services into Category I means payers are now expected to develop coverage policies for them.
What your billing team needs to do: If your practice uses AI-assisted diagnostic tools — particularly in cardiology, radiology, or wound care — identify which services now have Category I codes. Contact your major payers to understand their coverage and reimbursement positions for these new codes. Start documenting AI-assisted analyses in a way that supports the new code descriptors.
3. Lower Extremity Revascularization — Complete Code Restructure
If you are in vascular surgery, interventional radiology, or interventional cardiology — this is the most urgent change in the entire 2026 update.
<cite index=”46-1″>Among the key changes in the CPT 2026 code set is a significant, comprehensive revision of the leg revascularization code family.</cite> The old lower extremity revascularization codes have been completely deleted. <cite index=”45-1″>The AMA has deleted previous codes and replaced them with 46 territory-based codes (37254–37299).</cite>
The new codes are organized by vascular territory — meaning the specific anatomical location of the revascularization determines which code is used, rather than the procedure type alone. <cite index=”47-1″>The revised codes aim to improve access to advanced therapies that enhance mobility and functional status, especially for patients with persistent symptoms, such as pain, cramping, and fatigue, who have not responded to other medical treatments like medication or structured exercise.</cite>
What your billing team needs to do: Stop using the deleted lower extremity revascularization codes immediately. Map every procedure in this category to the appropriate territory-based code from the new 37254–37299 series. Update your EHR charge capture templates, your superbills, and your billing software code lists. Every claim submitted with a deleted code is generating an automatic denial.
4. Audiology and Hearing Device Services — 12 New Codes

Audiology practices have a completely new coding structure to learn in 2026.
<cite index=”49-1″>Legacy codes 92590–92595 will be deleted and replaced with 12 new codes that better align with contemporary audiology care. Examples include 92628 for the first 30 minutes of hearing-aid candidacy evaluation, with time-based add-on code 92629.</cite>
The new audiology coding structure is time-based and service-component specific — a significant departure from the older approach of broadly categorized hearing evaluation and fitting codes. The new framework separately codes the candidacy evaluation, the hearing aid fitting, the verification process, and ongoing follow-up — giving audiologists proper credit for each distinct service component.
What your billing team needs to do: Audit every current use of codes 92590 through 92595 in your system. Map each service component to the appropriate new code. <cite index=”49-1″>Audiology practices should update documentation templates, and review payer policies to ensure proper alignment.</cite> Contact your major payers to verify they have updated their systems for the new codes — some payers lag behind AMA release dates on coverage updates.
5. Immunization — New Vaccine Codes
New CPT codes have been added for mRNA-based influenza vaccines, reflecting advancements in vaccine technology that did not have proper billing codes previously.
<cite index=”52-1″>The latest Category I updates include the addition of two new immunization codes, reflecting advancements in vaccine development — particularly mRNA-based influenza vaccines. New codes include 90616 for influenza virus vaccine, trivalent (tIRV), mRNA, 37.5 mcg/0.38 mL dosage, intramuscular use.</cite>
What your billing team needs to do: Update your vaccine administration billing codes if you administer influenza vaccines. Verify payer coverage policies for the new mRNA-based vaccine codes — coverage determinations vary by payer and may require prior authorization in some cases.
6. Mid-Year PLA Code Updates — Effective July 1, 2026
Most practices think about CPT updates once a year, in December or January. That approach is no longer sufficient.
<cite index=”52-1″>Effective July 1, 2026, the AMA introduced 29 new PLA codes (0631U–0659U), 2 revised codes (0522U, 0598U), and 4 deleted codes (0029U, 0031U, 0423U, 0577U).</cite>
PLA codes — Proprietary Laboratory Analyses codes — are directly tied to specific laboratory tests and manufacturers. They are particularly sensitive to regulatory approvals and market availability of diagnostic tools. For laboratories and practices with high lab billing volume, these mid-year updates require the same level of attention and preparation as the January release.
<cite index=”52-1″>Instead of delaying implementation until the next calendar year, the AMA now introduces certain updates mid-year to keep pace with emerging technologies and treatments, ensure accurate reporting and reimbursement sooner, and reduce lag between clinical innovation and coding recognition.</cite>
What this means for your practice: Build a process for monitoring mid-year CPT updates — not just the annual release. Subscribe to AMA CPT News updates. Assign someone on your billing team — or confirm with your billing company — that mid-year code changes are tracked and implemented on their effective dates.
What the 84 Deleted CPT Codes Mean for Your Claims
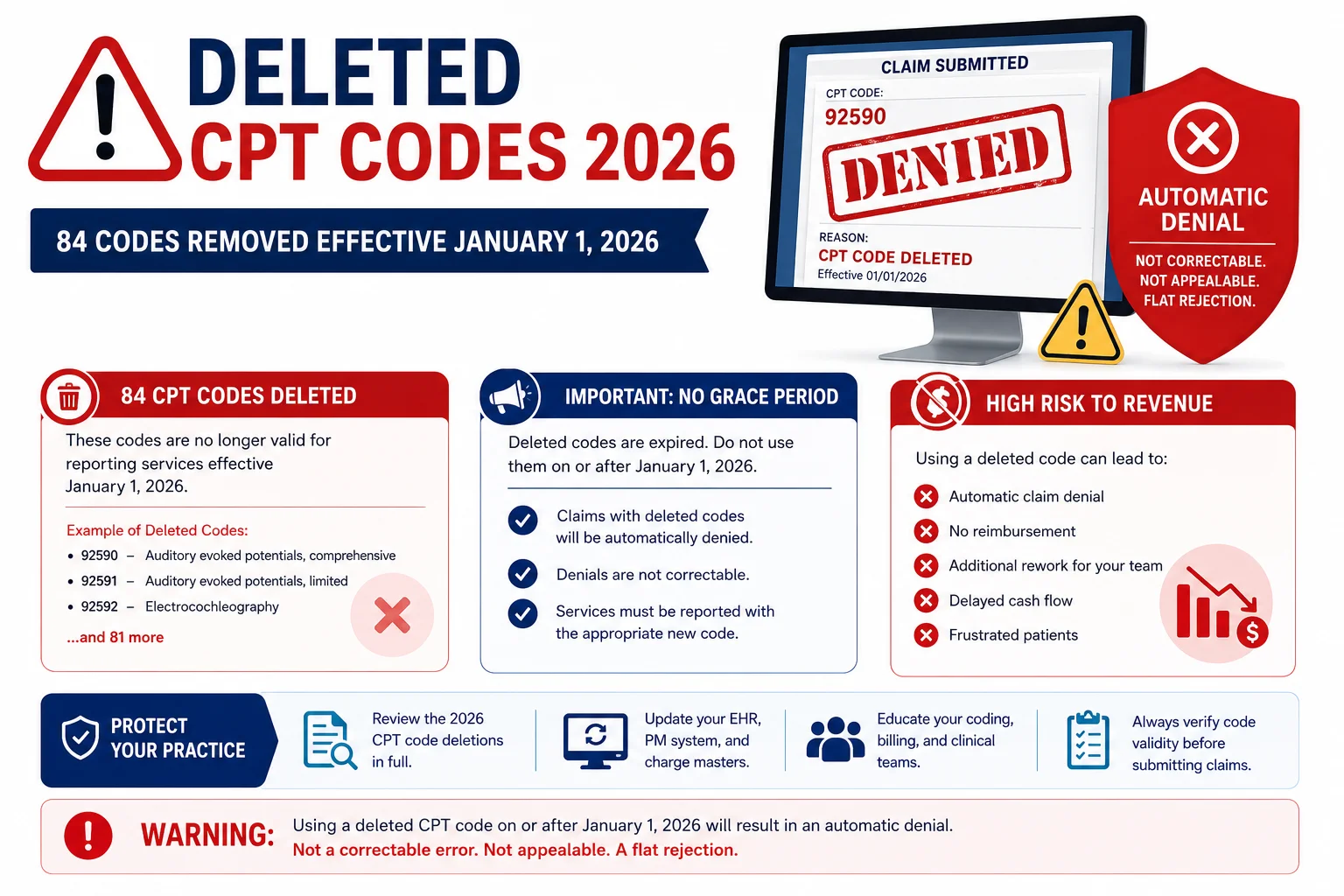
Of all the CPT code changes in 2026, the deletions are the most urgent from a denial prevention standpoint. A deleted code does not generate a soft denial that can be corrected and resubmitted. It generates a hard rejection — the claim is invalid as submitted, and resubmission requires mapping to the replacement code first.
<cite index=”51-1″>84 codes were deleted in 2026 — practices must check which ones affect them.</cite>
The categories most significantly affected by deletions are:
- Lower extremity revascularization (entire previous code family deleted, replaced by 37254–37299)
- Audiology and hearing device services (92590–92595 deleted, replaced by 12 new codes)
- Selected laboratory PLA codes (4 deleted effective July 1, 2026)
<cite index=”51-1″>For each deleted or revised code, map to the new or revised code you will use starting January 1.</cite> If your billing team has not done this mapping exercise yet — or if your billing company has not confirmed they updated their code tables — this needs to happen today, not at the next billing meeting.
The practical action: Pull a report of your 50 most-used CPT codes from 2025. Cross-reference that list against the 2026 deletions. Every deleted code your practice uses needs a mapped replacement before the next claim containing it is submitted.
The 46 Revised CPT Codes — Why Small Changes Create Big Problems
Revisions are easier to overlook than new codes or deletions — but they can be just as damaging if billing teams miss them.
<cite index=”49-1″>Across the full code set, the AMA reports 46 revisions, many of which affect bundling logic, guideline language, and descriptor terminology. Revised guidelines introduce updated service-level hierarchies and remove outdated terminology.</cite>
What does a revision mean in practice? A revised code may have:
- A changed time threshold (a service that previously required 30 minutes may now require 20, or vice versa)
- Updated bundling rules (services that were separately billable may now be bundled, or previously bundled services may now be unbundled)
- New documentation requirements added to the descriptor
- Removed terminology that changes which patients or clinical scenarios qualify
Any of these changes can silently affect your reimbursement — either generating denials you do not understand or causing you to bill at a lower level of service than you are entitled to.
The revised remote monitoring codes 99453 and 99454 are the most broadly impactful revisions for primary care, internal medicine, and chronic disease management practices. Review the updated descriptors carefully and verify your documentation templates capture what the revised codes require.
How to Do a CPT Code Audit for Your Practice Right Now
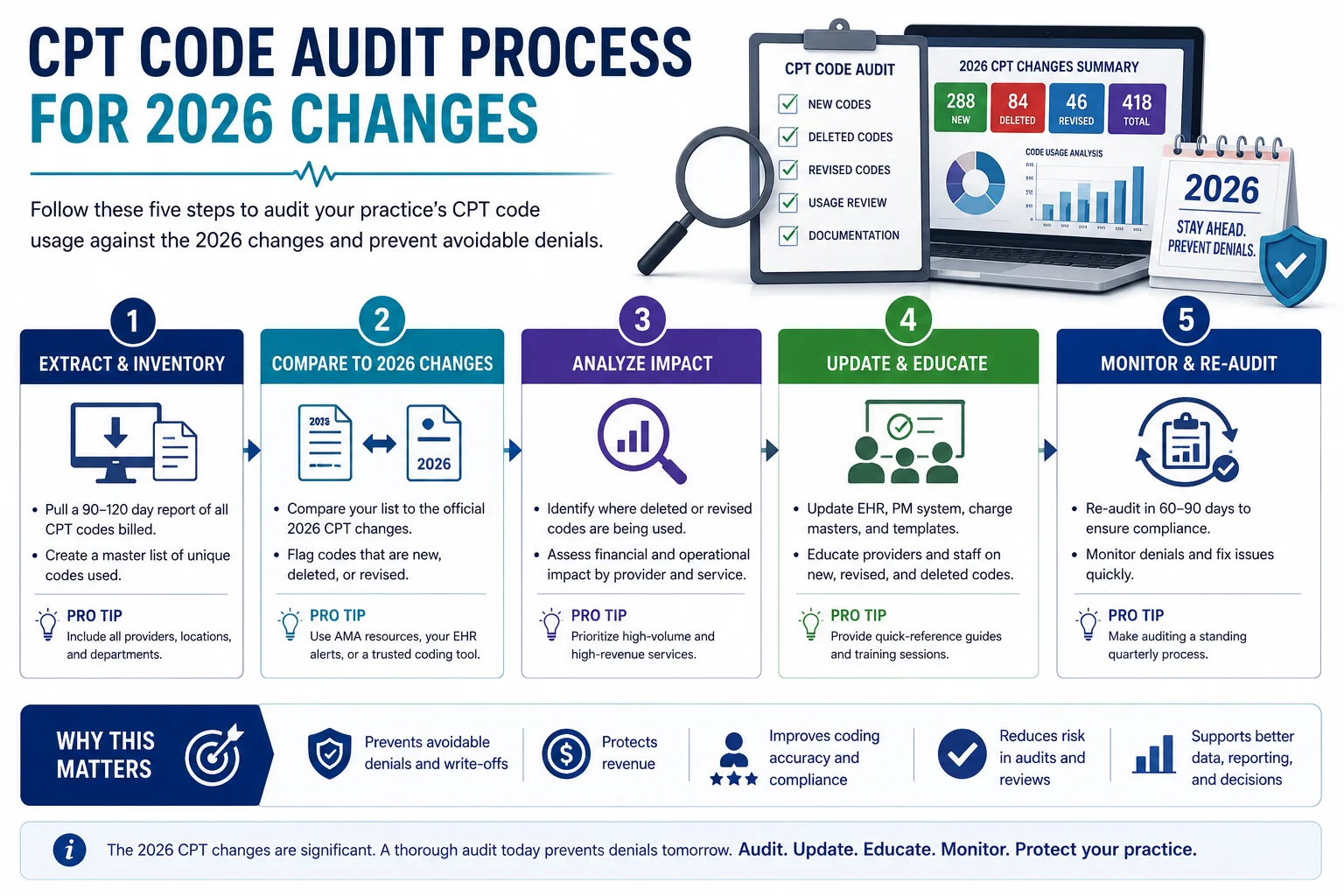
<cite index=”51-1″>Here is a practical roadmap your practice can follow to ensure you are ready for the 2026 CPT changes.</cite>
Step 1: Pull your top 50 most-used CPT codes from 2025. Your practice management system should be able to generate this report in minutes. These are your highest-risk codes — the ones that will cause the most damage if they are deleted or revised and your team does not know it.
Step 2: Cross-reference your top codes against the 2026 additions, deletions, and revisions list. <cite index=”51-1″>Compare your top 50 most-used codes this year with the 2026 changes list. Highlight codes you use that are deleted, revised, or replaced.</cite> The official AMA CPT 2026 code set is the authoritative source — or your billing company should have a complete crosswalk ready.
Step 3: Map every deleted code to its 2026 replacement. For every deleted code your practice uses, identify the new code that replaces it and document the transition rule. This is not optional — submitting a deleted code generates an automatic rejection.
Step 4: Update your EHR, superbill, and billing software. <cite index=”51-1″>Load the updated CPT file into your EHR and billing software. Update claim-edit rules, bundling logic, and other automated checks for new codes.</cite> If your billing company handles this for you — confirm in writing that they have completed their code table updates.
Step 5: Update documentation templates for revised and new codes. New codes and revised codes often come with new documentation requirements. Make sure your clinical documentation templates — encounter notes, procedure notes, telehealth templates — capture the elements the new code descriptors require. A correctly billed code that lacks supporting documentation will generate a medical necessity denial just as surely as a wrong code.
What the 2026 CPT Changes Mean for Specific Specialties
Cardiology and Interventional Cardiology
The new AI Category I codes for coronary atherosclerotic plaque assessment and perivascular fat analysis for cardiac risk are directly relevant. If your cardiology practice uses AI-assisted diagnostic tools, you now have Category I codes to bill them. Additionally, the lower extremity revascularization restructure significantly affects interventional cardiology practices — the deleted codes must be replaced with the appropriate territory-based code from the 37254–37299 series.
For specialty-specific billing expertise, see our cardiology billing services.
Primary Care and Internal Medicine
The revised and new remote physiologic monitoring codes — 99453, 99454, 99445, and 99470 — are the most significant changes for primary care. If your practice monitors chronic disease patients remotely, the expanded RPM code set creates new billing opportunities that did not exist under the 2025 code set. Review your RPM documentation workflows against the revised descriptors.
For primary care billing expertise, see our family practice billing services.
Wound Care
The new AI Category I codes for multispectral imaging for burn wounds are directly applicable to advanced wound care practices. This is a previously uncoded service that sophisticated wound care practices have been delivering without reimbursement.
For wound care billing, see our wound care billing services.
Audiology
The complete replacement of legacy codes 92590–92595 with 12 new time-based and component-specific codes is the most significant change in audiology billing in years. Every audiology practice in the country needs to update their charge capture, documentation templates, and payer verification processes for this restructure.
Mental Health and Behavioral Health
While there are no major Category I CPT restructures in behavioral health coding for 2026, the mid-year PLA code additions may affect practices that use laboratory-based diagnostic tools in treatment planning. Monitor mid-year updates through our mental health billing services.
How Pro Health Care Advisors Handles CPT Code Changes for Our Clients

One of the strongest arguments for outsourcing medical billing — particularly in a year with 418 CPT code changes — is that keeping up with these updates is a full-time professional responsibility, not something an already-stretched in-house billing team can absorb as a side task.
At Pro Health Care Advisors, <cite index=”52-1″>coding agility is a competitive advantage</cite> we build into our service model from day one. Our AAPC-certified billing team tracks every CPT code change — January releases, mid-year updates, payer-specific adoption timelines — and implements them across every client account on their effective dates.
Here is specifically what we do when CPT code changes take effect:
Code table updates on day one. Every new, deleted, and revised code is updated in our billing systems before the effective date — not after denials start appearing.
Deleted code crosswalk for every client. Before January 1 of each year, we audit every client’s most-used codes against the deletion list and map replacements proactively. No client submits a deleted code because no one noticed.
Documentation template review. For clients with revised or new codes in their specialty, we flag documentation gaps before they generate denials.
Mid-year monitoring. We track AMA mid-year releases and implement PLA code updates on their July 1 effective dates — not months later.
Payer adoption tracking. We monitor which payers have adopted coverage policies for new Category I codes and advise clients on when to begin billing new codes with confidence.
Our CodeMAXX services provide an additional layer of coding accuracy review — catching mismatches between documentation and selected codes before claims are submitted. Our medical billing and practice management services handle the full billing cycle with a 98.5 percent clean claim rate and a denial rate under 2 percent.
For more billing education including denial management, see our complete guide to medical billing denial codes and our articles and resources library.
Frequently Asked Questions — CPT Code Changes 2026
Q: When did the 2026 CPT code changes take effect? The primary 2026 CPT code changes took effect January 1, 2026. Mid-year updates — including 29 new PLA codes — took effect July 1, 2026. Any claim submitted with a deleted code after its effective date generates an automatic rejection.
Q: How many CPT codes changed in 2026? The AMA released 418 total changes in the 2026 CPT code set — 288 new codes, 84 deletions, and 46 revisions. This is one of the larger single-year update volumes in recent history, driven largely by advances in AI, remote monitoring, and surgical technique.
Q: What happens if I bill a deleted CPT code? The claim will be rejected as invalid. Unlike a denial — which is processed and then contested — a rejected claim must be corrected and resubmitted with the appropriate active code. The longer you wait to identify deleted code usage, the more claims accumulate in rejection status and the more staff time is required to correct them.
Q: Do payers automatically cover new CPT codes? Not always — and this is a critical point. New Category I codes are recognized by the AMA as billable, but individual payers set their own coverage policies. Some payers adopt new codes immediately. Others take months to publish coverage determinations. Before billing a new code, verify coverage with the specific payer — particularly for the new AI Category I codes and new immunization codes.
Q: How do I find the complete list of 2026 CPT code changes? The authoritative source is the American Medical Association CPT 2026 code set. The complete list of additions, deletions, and revisions is available through AMA’s CPT Professional Edition and licensed data files. Your billing company or EHR vendor should also provide a summary of changes relevant to your specialty.
Q: How do I know which deleted codes affect my practice? Pull a report of your most frequently used CPT codes from 2025. Cross-reference that list against the 2026 deletion list. Any match requires immediate action — identify the replacement code, update your billing system, and update your clinical documentation templates.
Q: Does Pro Health Care Advisors update codes for clients automatically? Yes. Our team updates all client code tables before effective dates, audits deleted code usage proactively, maps replacements for every client, and monitors mid-year releases. Our clients do not generate denials from using deleted codes because we handle this before it becomes a problem. Learn more through our medical billing and practice management services.
For more on how claim denials happen and how to prevent them, read our complete guide to medical billing denial codes.
The Bottom Line — 418 Changes Means 418 Opportunities to Get It Right or Wrong

Here is the straightforward reality of the 2026 CPT code changes: 418 total updates means 418 points in the billing process where your practice either gets it right and gets paid — or gets it wrong and generates a denial.
Most of those 418 changes will not affect your practice directly. But the ones that do — particularly the 84 deleted codes and the major restructures in revascularization, audiology, and remote monitoring — will generate a consistent stream of denials and rejected claims until someone fixes the root cause.
The practices that sail through these annual updates without revenue disruption are not lucky. They have billing processes — in-house or outsourced — that treat coding updates as an operational priority, not an afterthought. They audit. They map. They update. They monitor mid-year releases. And they never submit a deleted code because they identified the deletion before it cost them a claim.
If your practice has not completed a CPT code audit for 2026, or if you are not sure whether your billing company has — that gap is generating denials right now.
Pro Health Care Advisors can show you exactly where.
Schedule Your Free Consultation with Pro Health Care Advisors →
We will review your current billing performance, check for deleted or outdated codes in your claim submission history, and show you specifically what a current, compliant coding process looks like for your specialty.