Medical Billing vs In-House Billing | The Real Cost Comparison for Doctors in 2026
Most doctors make the medical billing vs in-house billing decision the same way.
They look at what their biller earns — say, $50,000 per year — add a rough estimate for software, call it $60,000 total, and conclude that outsourcing at 6 or 7 percent of collections would cost more.
Then they never look at the full picture.
They do not count the benefits and payroll taxes that add 25 to 35 percent on top of the salary. They do not count the software, clearinghouse fees, and statement processing costs. They do not count the training, certification, and continuing education. They do not count what happens during the two weeks their biller is on vacation, or the $5,000 to $12,000 it costs to replace them when they leave — which happens more than one in three years on average, given industry turnover rates approaching 40 percent.
And most importantly, they do not count the denied claims that never get worked, or the systematic undercoding that quietly reduces net collections by 6 to 9 percent without ever appearing as a line item on any report.
When you count all of it, the math almost always tells a different story.
This guide is the complete medical billing vs in-house billing cost comparison for 2026 — with real numbers, real examples, and a straightforward framework for figuring out which model makes more financial sense for your specific practice.
Why This Decision Is More Consequential in 2026 Than Ever Before
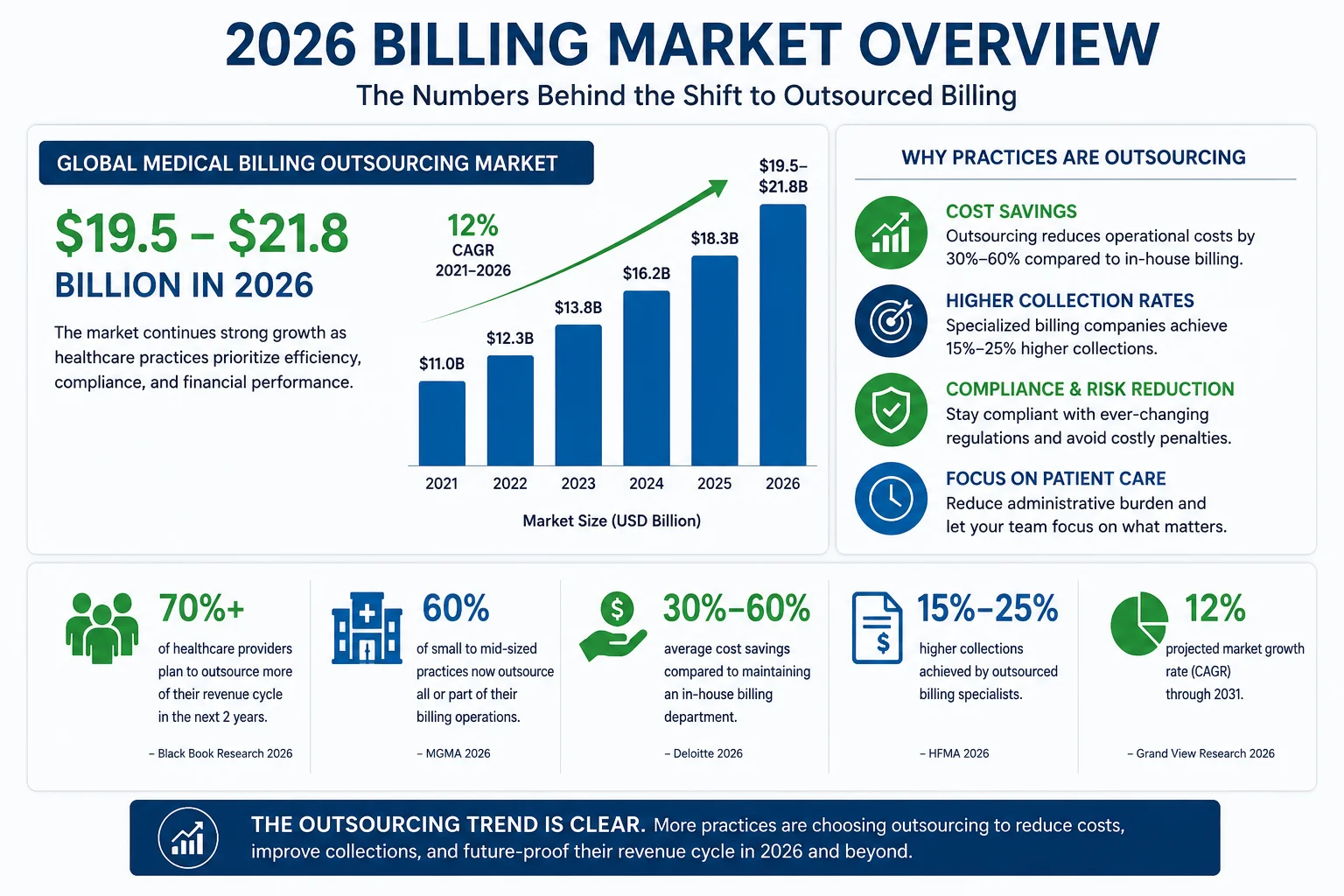
According to GetPracticeHelp’s 2026 billing analysis, the medical billing outsourcing market reached an estimated $19.5 to $21.8 billion in 2026 and is projected to grow at approximately 12 percent annually through 2035. That growth is not driven by marketing. It is driven by practice owners doing the actual math and realizing the outsourced model outperforms in-house billing on nearly every measurable dimension.
Three forces are making this decision more important in 2026 than at any prior point:
Billing complexity is rising. Prior authorization requirements have expanded. Payer rules change more frequently. The 2026 CPT update included 418 total changes — 84 deleted codes alone. Keeping an in-house billing team current on all of this requires a training investment most practices do not budget for.
Staffing is harder and more expensive. Annual turnover in medical billing roles runs between 33 and 40 percent. Hiring and onboarding a replacement biller costs $4,000 to $12,000 per hire, plus 60 to 90 days of reduced productivity during the transition. In major cities, experienced billers now command $50,000 to $65,000 in base salary.
Denial rates keep rising. The national initial claim denial rate hit 11.8 percent in 2024 and continued rising into 2026. For practices without structured denial management workflows — which describes most in-house billing operations — denied claims pile up in AR queues, age past appeal windows, and get written off as uncollectable.
According to Coherent Market Insights’ 2026 billing market report, outsourcing can save mid-sized hospitals between $200,000 and $500,000 per year. Outsourcing partners typically have denial rates up to 20 percent lower and reimbursement cycles 10 to 15 percent faster than in-house operations.
The True Cost of In-House Medical Billing — Every Line Item
Here is the complete in-house billing cost breakdown for a small to mid-size practice with one to two billers. These are real 2026 numbers — not estimates designed to make outsourcing look better.
Visible Costs — What You Know You Are Paying
Biller salary: According to MZ Billing’s 2026 cost analysis, a full-time medical biller earns $35,000 to $45,000 in smaller markets and $50,000 to $65,000 in major cities. Coding specialists command $50,000 to $75,000. Practice managers overseeing billing earn $60,000 to $90,000. For this comparison, use $52,000 as a mid-range biller salary.
Benefits and payroll taxes: Benefits add 25 to 40 percent on top of base salary. Health insurance alone costs $8,000 to $15,000 per employee annually. Adding retirement contributions, payroll taxes, workers compensation, and paid time off — the true employment cost per biller is $65,000 to $85,000 annually, not the $52,000 salary figure.
Billing software subscription: Practice management and billing software runs $300 to $1,500 per month. Annual cost: $3,600 to $18,000.
Clearinghouse fees: Electronic claim submission through a clearinghouse costs $0.25 to $0.45 per claim. For a practice submitting 2,000 claims per month, that is $6,000 to $10,800 per year.
Statement printing and mailing: Patient statements sent by mail cost $0.65 to $1.25 per statement. For 500 statements per month, that is $3,900 to $7,500 per year.
Training and certification: AAPC and AHIMA certification costs $300 to $600 per exam. Annual continuing education requirements add $500 to $1,500 per certified biller.
Hidden Costs — What Most Practices Are Not Counting
Staff turnover and replacement: With billing staff turnover at 33 to 40 percent annually, the average practice replaces a biller every 2.5 to 3 years. According to Revenue Synergy’s cost analysis, the cost of replacing a biller is $4,000 to $7,000 per hire, plus 2 to 3 months of reduced productivity during onboarding — effectively adding $1,500 to $3,000 to annual billing costs when amortized.
Denied claim write-offs: In-house billing teams typically work only the highest-value denials. Low and mid-value denied claims get deprioritized, aged past appeal windows, and written off. For a practice collecting $150,000 per month with a 10 percent denial rate, even 50 percent denial write-off (extremely conservative) is $7,500 per month — $90,000 per year — in revenue that was earned but never collected.
Undercoding losses: Research consistently identifies undercoding as costing practices 6 to 9 percent of net collections. This never appears as a denial or a write-off — undercoded claims get paid, just for less than the documentation supports. On a practice collecting $1.2 million annually, undercoding at 7 percent is $84,000 per year in invisible revenue loss.
Physician oversight time: Every hour a physician spends reviewing billing reports, fixing billing questions, or handling EOB disputes is an hour not spent on patient care. At a physician’s hourly rate, even two hours per week of billing oversight represents $10,000 to $30,000 in annual opportunity cost.
Office space and equipment: Dedicated workspace, computers, and office equipment for billing staff — often overlooked as a “billing cost” but real nonetheless. $5,000 to $12,000 per year for a small practice.
What the Real Total Looks Like
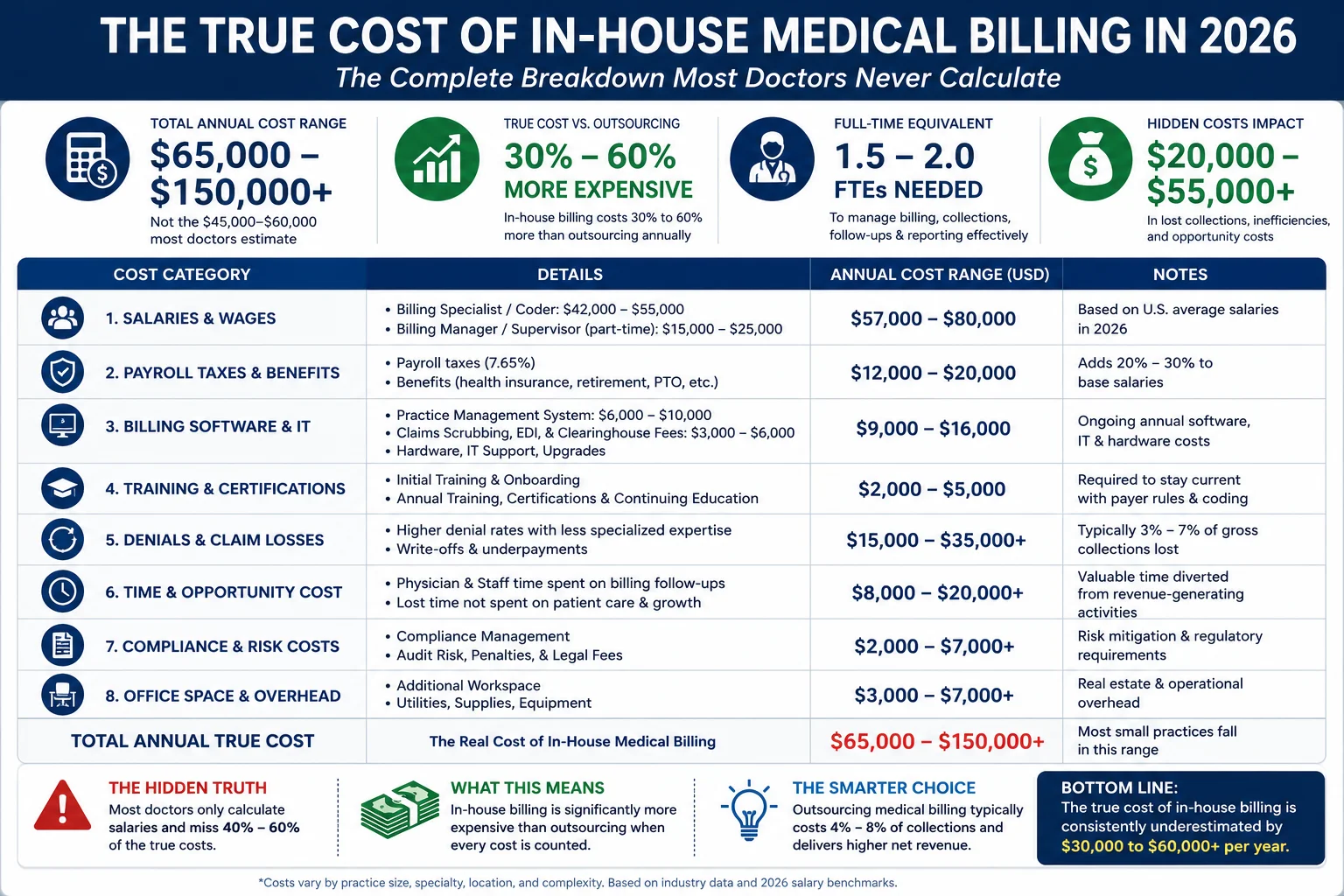
| Cost Component | Annual Cost |
|---|---|
| Biller salary (1 FTE, mid-range) | $52,000 |
| Benefits + payroll taxes (30%) | $15,600 |
| Billing software + clearinghouse | $9,600 |
| Statement printing + mailing | $5,700 |
| Training + certification | $1,000 |
| Turnover cost (amortized) | $2,500 |
| Office space + equipment | $8,000 |
| Physician oversight (2 hrs/week) | $15,000 |
| Subtotal — Operational Costs | $109,400 |
| Denied claim write-offs (conservative) | $18,000–$90,000+ |
| Undercoding losses (7% of collections) | $42,000–$168,000+ |
| True Annual Billing Cost | $65,000–$150,000+ |
According to 247 Medical Billing Services’ 2026 comparison, in-house billing salaries alone typically range from $55,000 to $75,000 in 2026, with benefits and payroll taxes adding 20 to 30 percent. When all costs are included, total in-house billing overhead consistently runs $65,000 to $150,000 or more annually — far exceeding the $45,000 to $60,000 most practices estimate when they only count salary and software.
The True Cost of Outsourced Medical Billing — What You Actually Pay
Most outsourced medical billing companies use a percentage-of-collections model — meaning you pay a percentage of what they actually collect for you, not a flat fee regardless of performance.
Pricing by Practice Size and Specialty
| Practice Type | Typical Outsourcing Rate |
|---|---|
| Solo practitioner | 8–12% of collections |
| Small group (2–5 providers) | 6–9% of collections |
| Mid-size practice (5–10 providers) | 5–8% of collections |
| Large group (10+ providers) | 4–7% of collections |
| High-complexity specialties (cardiology, oncology, behavioral health) | 8–12% of collections |
| Moderate complexity (family practice, internal medicine) | 5–8% of collections |
According to DrCatalyst’s 2026 billing cost guide, most medical billing companies charge between 4 and 8 percent of monthly collections, with solo practices often paying 10 to 12 percent due to lower volume.
What Is Included at That Price
When you pay 5 to 7 percent of collections to a reputable billing company, what you receive includes:
- Real-time insurance eligibility verification before every appointment
- Prior authorization tracking and management
- AAPC-certified claim coding and submission
- Pre-submission claim scrubbing
- Payment posting and ERA reconciliation
- Denial management and appeals
- AR follow-up and aged claim recovery
- Real-time reporting and dashboard access
- Credentialing support (at many companies including Pro Health Care Advisors)
- Compliance monitoring
That is not a comparable cost to one biller’s salary — it replaces a biller, a coder, a denial management specialist, and a credentialing coordinator, all with a team that specializes in one thing.
Side-by-Side Cost Comparison — Four Practice Sizes
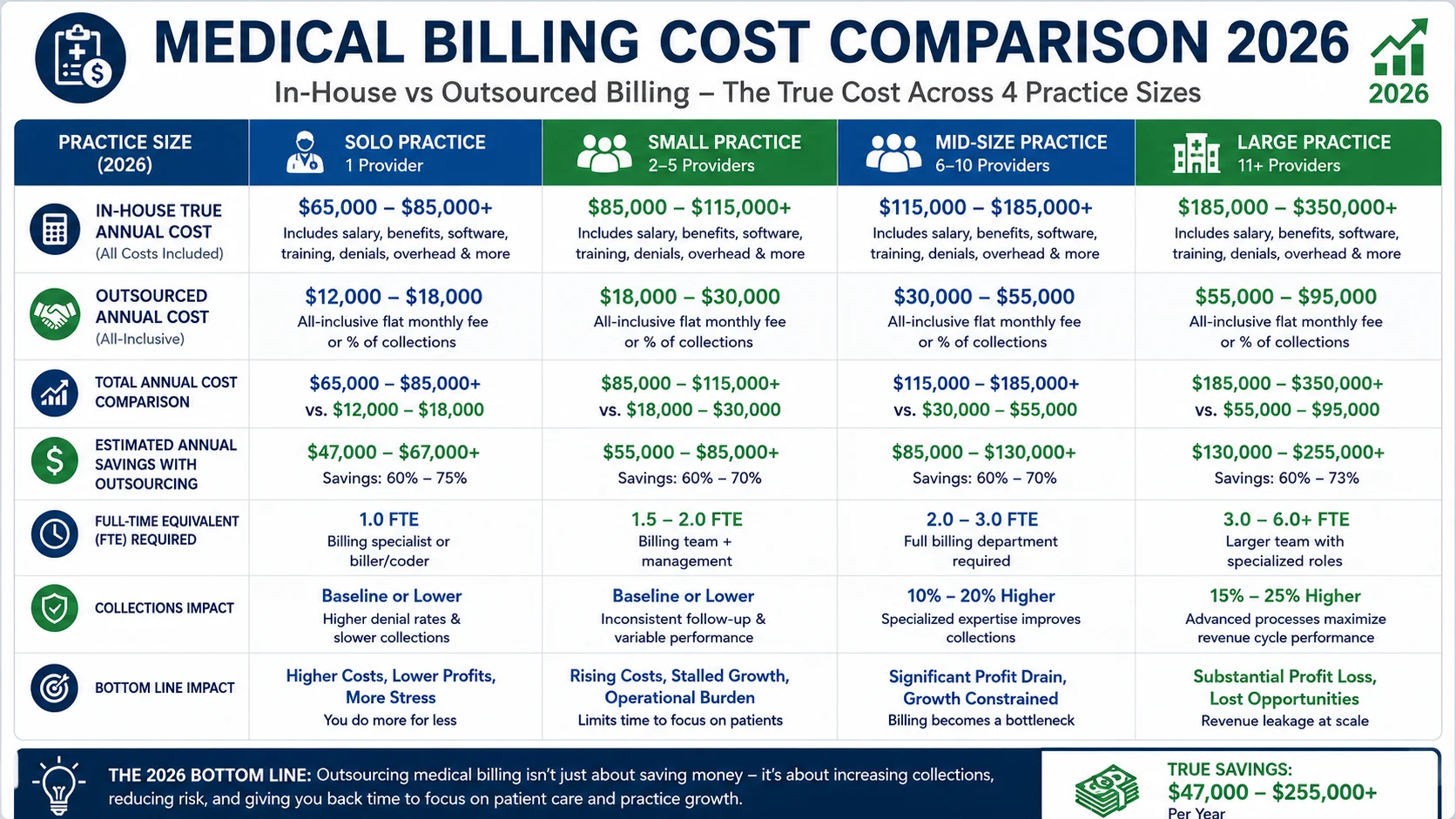
Example 1 — Solo Practitioner Collecting $400,000/Year
In-house billing:
- 1 part-time biller: $32,000 salary + $9,600 benefits = $41,600
- Software + clearinghouse: $8,400
- Denial losses (10% denial rate, 50% abandoned): $20,000
- Undercoding (7%): $28,000
- True annual cost: ~$98,000 (24.5% of collections)
Outsourced at 8%:
- Service fee: $32,000
- Improved collections (5% improvement): +$20,000
- Net effective cost: ~$12,000 (3% of collections)
Example 2 — Small Group Practice, 3 Physicians, $1.2M/Year
According to Revenue Synergy’s detailed example, a 3-physician family practice with 2 in-house billing staff has the following real costs: lead biller $52,000 + billing assistant $40,000 + benefits at 30% ($27,600) + software $9,600 + clearinghouse $8,400 + statements $7,200 + training $2,400 + office overhead $8,000 + administrator oversight $13,500 + amortized recruiting $3,000 = $171,700 per year, or 14.3% of collections.
The same practice outsourced at 5.5 percent of collections pays $66,000 in service fees plus approximately $4,500 in remaining internal oversight = $70,500 per year, or 5.9% of collections.
Direct annual savings: $101,200
Then the revenue improvement: if denial rate drops from 10 percent to 2 percent and AR falls from 42 days to 28 days — conservative outcomes for a practice switching to a high-performance billing company — the combined revenue improvement easily exceeds $150,000 annually.
Example 3 — Mid-Size Practice, 5 Providers, $2.5M/Year
In-house billing (3 staff):
- 3 billers/coders: ~$170,000 fully loaded
- Software + overhead: $25,000
- Denial losses: $50,000
- Undercoding: $87,500
- True annual cost: ~$332,500 (13.3% of collections)
Outsourced at 6%:
- Service fee: $150,000
- Revenue improvement: +$100,000–$250,000
- Net effective cost: well under 5% of collections
Example 4 — Large Group, 10+ Providers, $5M+/Year
At this scale, in-house billing becomes more economically competitive — but only if the practice has invested in a genuine billing infrastructure: AAPC-certified staff, structured denial management, systematic prior authorization tracking, real-time reporting, and active compliance monitoring. For large practices already operating at this level, the in-house model can be competitive. For large practices that have grown their billing team reactively rather than strategically, the outsourced model often still delivers better net revenue.
The Revenue Performance Gap — The Number Most Practices Ignore
Here is where the medical billing vs in-house billing comparison gets decisive.
The average in-house billing operation collects 85 to 90 percent of allowable charges. A high-performing outsourced billing partner with active denial management typically collects 93 to 97 percent.
On a practice collecting $200,000 per month, that 6 to 8 percent collection rate improvement is $12,000 to $16,000 in additional revenue every single month. Every year. Without seeing a single additional patient.
According to Dr Billing Service’s 2026 comparison guide, many practices experience 5 to 15 percent revenue improvement after outsourcing. Even at 5 percent improvement on a $1.2 million practice, that is $60,000 in additional annual revenue — which more than covers the outsourcing fee for most practices.
The correct question in the medical billing vs in-house billing decision is not “which option costs less?” It is “which option produces the most net revenue after all costs are accounted for?” For most practices under $1.5 million in annual collections, outsourcing produces a clear net financial benefit. For larger practices, the answer requires practice-specific modeling — but the performance gap still needs to be honestly evaluated.
When In-House Billing Actually Makes More Sense
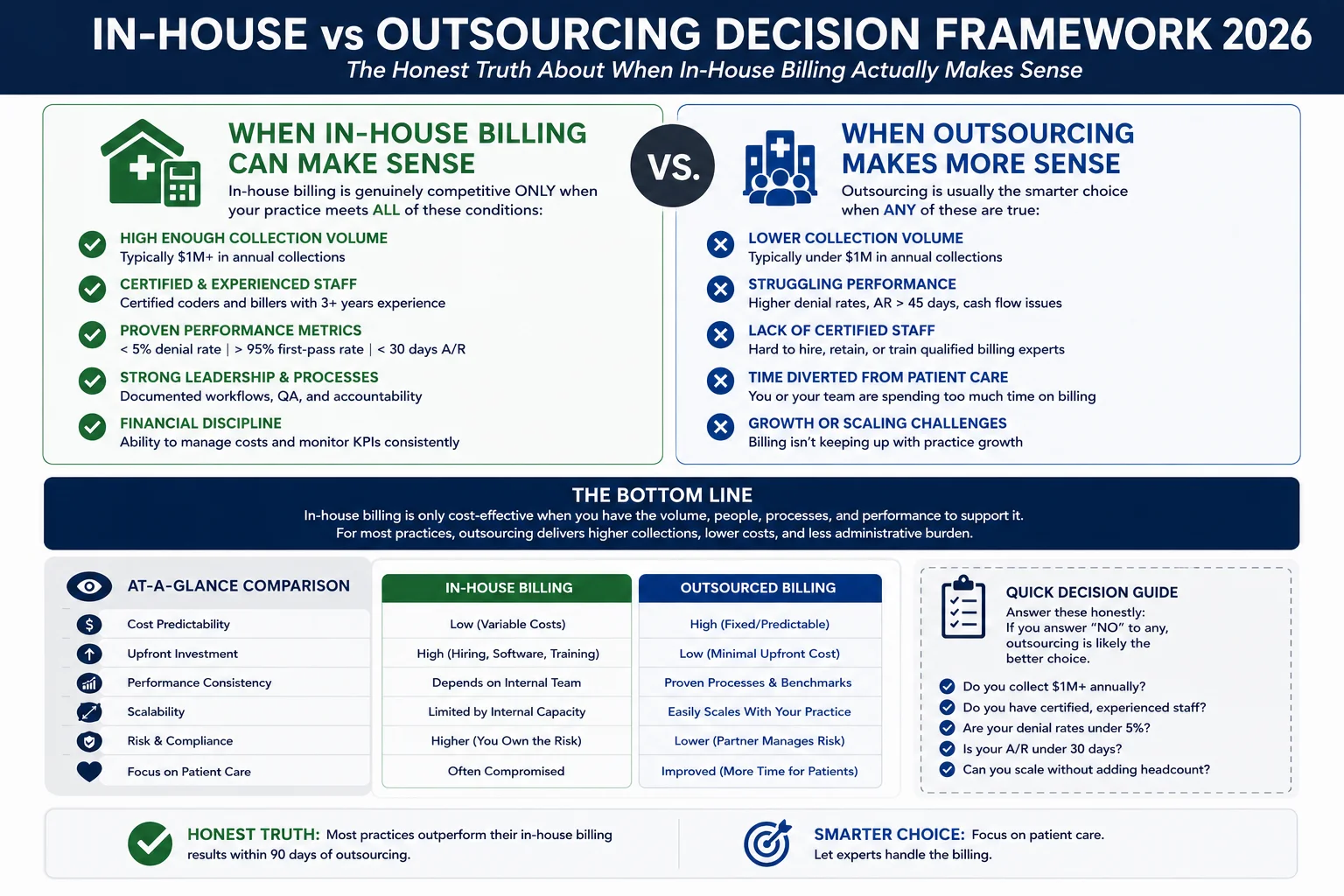
In the interest of an honest comparison, here is when in-house billing genuinely makes sense:
Your practice collects $1.5 million or more annually AND you have invested in genuine billing infrastructure. At 10 or more providers with $5 million or more in collections, a well-built in-house billing team can be cost-competitive — but only with AAPC-certified coders, structured denial management, systematic prior authorization tracking, and active compliance monitoring.
Your in-house team performs at a certified, measurable level. If your team maintains a clean claim rate above 95 percent, a denial rate below 5 percent, and a net collection rate above 93 percent — with data to prove it — you have a genuinely strong in-house operation worth keeping.
You have a high-volume, low-complexity specialty. Cash-pay practices or practices with very simple, standardized billing — some concierge medicine models, for example — have lower billing complexity where the in-house cost advantage is more competitive.
For most practices that do not clearly meet these conditions — which is the majority of small and mid-size practices in the country — outsourcing produces better net revenue at lower total cost.
The critical mistake most doctors make is comparing their estimate of in-house costs against the list price of outsourcing, without accounting for denied claim write-offs, undercoding losses, and the true total cost of in-house operations. That comparison almost always underestimates in-house costs and overestimates the net cost of outsourcing.
The Hidden Costs Nobody Mentions in the Medical Billing vs In-House Billing Debate
The Single Point of Failure Problem
When your billing depends on one or two people, a single resignation, medical leave, or extended vacation creates an immediate billing crisis. Claims pile up. Denials age past appeal windows. AR grows. By the time a replacement is hired and trained, you have 60 to 90 days of billing backlog that can take months to recover.
The Compliance Exposure Problem
CMS updates guidelines. State Medicaid programs revise authorization requirements. CPT codes change annually. Keeping in-house billers current on all regulatory changes requires training investment that most practices do not budget for. When compliance falls behind, the consequences range from avoidable denials to audit findings. For our HIPAA compliance approach, see our HIPAA compliance services.
The Technology Gap Problem
Medical billing software in 2026 includes AI-assisted coding, predictive denial management, and automated prior authorization tracking. Quality outsourced billing companies invest in these tools continuously and apply them across their entire client base. Most in-house teams work with practice management software that has not been significantly updated in years.
For more on how AI is reshaping billing operations in 2026, see our AI in medical billing guide.
How Pro Health Care Advisors Compares on the Numbers That Matter

If you are evaluating the medical billing vs in-house billing question for your practice, the most useful thing you can do is get your own numbers — not industry averages, but the actual performance metrics for your current billing operation:
- What is your current clean claim rate?
- What is your current denial rate by payer?
- What is your net collection rate?
- What are your days in AR?
- What is your patient collection rate?
If you cannot answer all five of these questions immediately, your billing visibility is insufficient — and problems are likely happening that nobody has identified yet.
Pro Health Care Advisors provides medical billing and revenue cycle management for practices across the United States. Our numbers for 2026:
98.5% clean claim rate — compared to the 85 to 92 percent average for in-house billing operations.
Under 2% denial rate — compared to the national average of 11.8 percent.
Full revenue cycle management — eligibility verification, prior authorization, AAPC-certified coding, payment posting, denial management, AR follow-up, and patient collections. See our medical billing and practice management services.
Physician credentialing — our physician credentialing service handles the entire enrollment process, eliminating the credentialing gaps that create revenue voids for new providers.
Audit protection — our MD Audit Shield RAC service protects your practice from RAC audit findings.
30+ specialties — cardiology, family practice, mental health, wound care, and more. See our full specialties list.
Frequently Asked Questions — Medical Billing vs In-House Billing 2026
Q: Is outsourcing medical billing cheaper than in-house billing? For most practices under $1.5 million in annual collections — yes, when you count all true costs. The true cost of in-house billing for a small practice typically runs $65,000 to $150,000 per year when salary, benefits, software, turnover, denial write-offs, and undercoding losses are all included. Outsourced billing at 5 to 7 percent of collections typically costs less and produces higher net collections due to better clean claim rates and lower denial rates.
Q: What percentage do outsourced medical billing companies charge in 2026? Most charge between 4 and 8 percent of net collections. Solo practices typically pay 8 to 12 percent due to lower volume. Large groups with 10+ providers often negotiate 4 to 6 percent. High-complexity specialties — cardiology, behavioral health, oncology — typically pay toward the higher end of the range. Flat-fee models also exist but remove the performance incentive alignment.
Q: What is a typical in-house medical billing cost per year? For a small practice with one biller, the true all-in annual cost is typically $65,000 to $95,000 in operational costs — plus $18,000 to $90,000 in denied claim write-offs and $42,000 to $168,000 in undercoding losses, depending on practice size and billing performance. The commonly cited figure of $45,000 to $60,000 accounts only for salary and software — not the full cost picture.
Q: When does in-house billing make financial sense? In-house billing is most competitive for large practices (10+ providers, $5M+ in collections) with certified billing staff, structured denial management, and documented performance metrics — clean claim rate above 95 percent, denial rate below 5 percent, net collection rate above 93 percent. For most small and mid-size practices, the outsourced model produces better financial outcomes.
Q: What is the revenue improvement from switching to outsourced billing? Most practices see 5 to 15 percent revenue improvement after switching to a high-performance outsourced billing company — driven by lower denial rates, higher clean claim rates, and recovery of previously abandoned denied claims. On a practice collecting $1.2 million annually, a 5 percent revenue improvement is $60,000 in additional annual revenue.
Q: What should I look for in an outsourced billing company? Ask for their clean claim rate (should be above 97%), their denial rate (should be below 5%, ideally below 2%), their net collection rate (should be above 93%), and whether they have AAPC-certified coders. Confirm HIPAA compliance with a signed BAA. Verify payer-specific experience for your specialty and state. And confirm that pricing is percentage-based — not flat fee. For our denial prevention approach, see our medical billing denial codes guide.
For more on the revenue cycle and billing trends shaping 2026, see our medical billing trends guide and our revenue cycle management complete guide.
For more billing resources, visit our articles and resources library.
The Bottom Line — The Real Medical Billing vs In-House Billing Decision
The medical billing vs in-house billing decision is not a comparison between what you pay a biller and what you pay a billing company. It is a comparison between the total cost of two complete billing systems — including performance, technology, staffing risk, compliance exposure, and the revenue impact of denial rates and collection rates.
When that complete comparison is made honestly, with all costs on the table, the outsourced model outperforms in-house billing for most small and mid-size practices in 2026. Not by a small margin. By $30,000 to $100,000 per year or more in combined cost savings and revenue improvement, for practices at typical size and billing performance levels.
The practices that have made this calculation correctly are not paying more for billing. They are collecting more revenue, spending less on administrative overhead, and eliminating the staffing and compliance risks that in-house billing creates.
Pro Health Care Advisors will run that calculation for your practice — with your actual numbers, not industry averages.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pitch. No pressure. Just a real look at what your billing is actually costing you — and what better billing would be worth.