Prior Authorization Rules Changed 2026 — Why This Is Not Business as Usual
If you have noticed something different about prior authorizations since January 2026, you are not imagining it.
The rules changed. Not in a small, quiet way. In a real, operational, affects-your-practice-every-single-day kind of way.
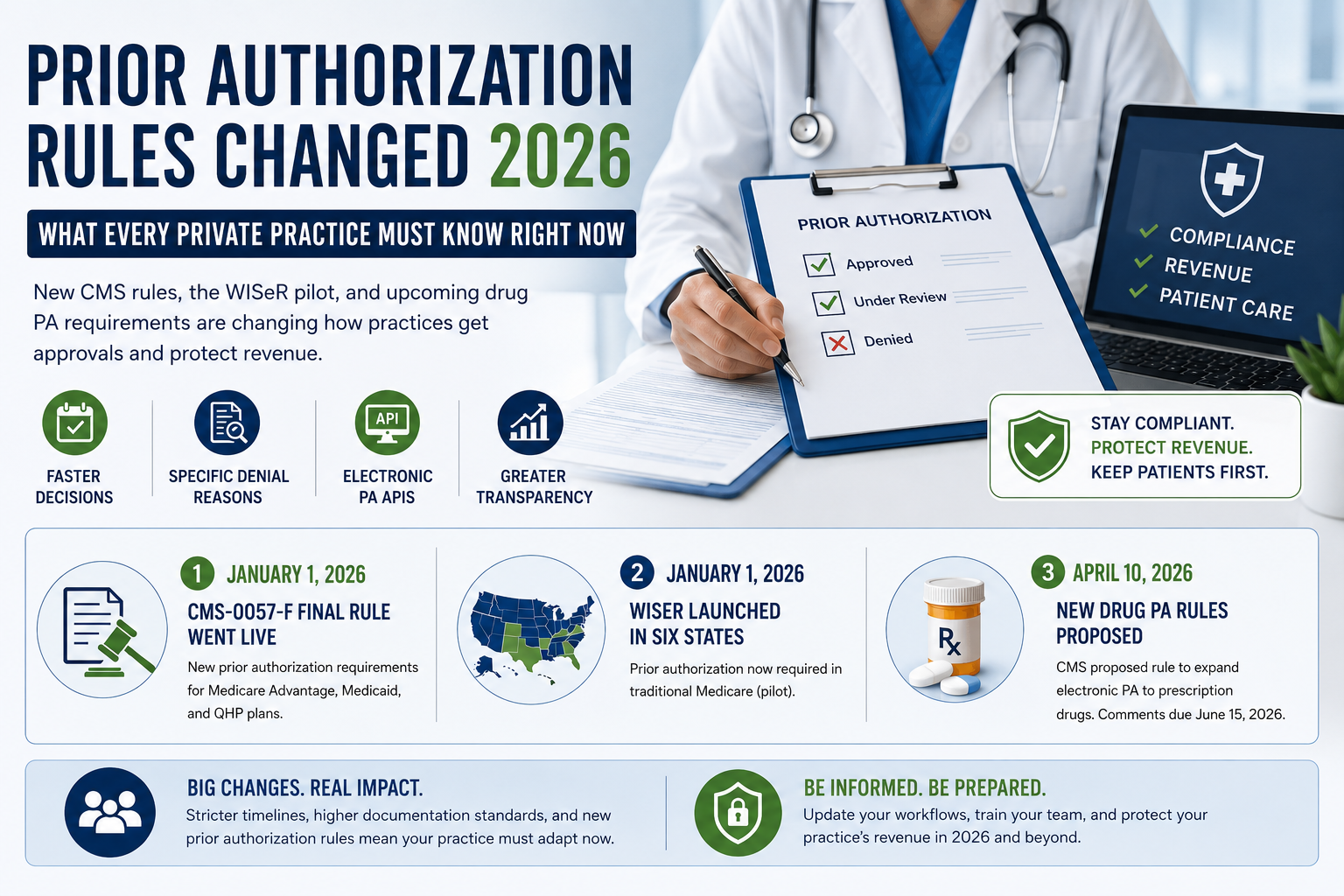
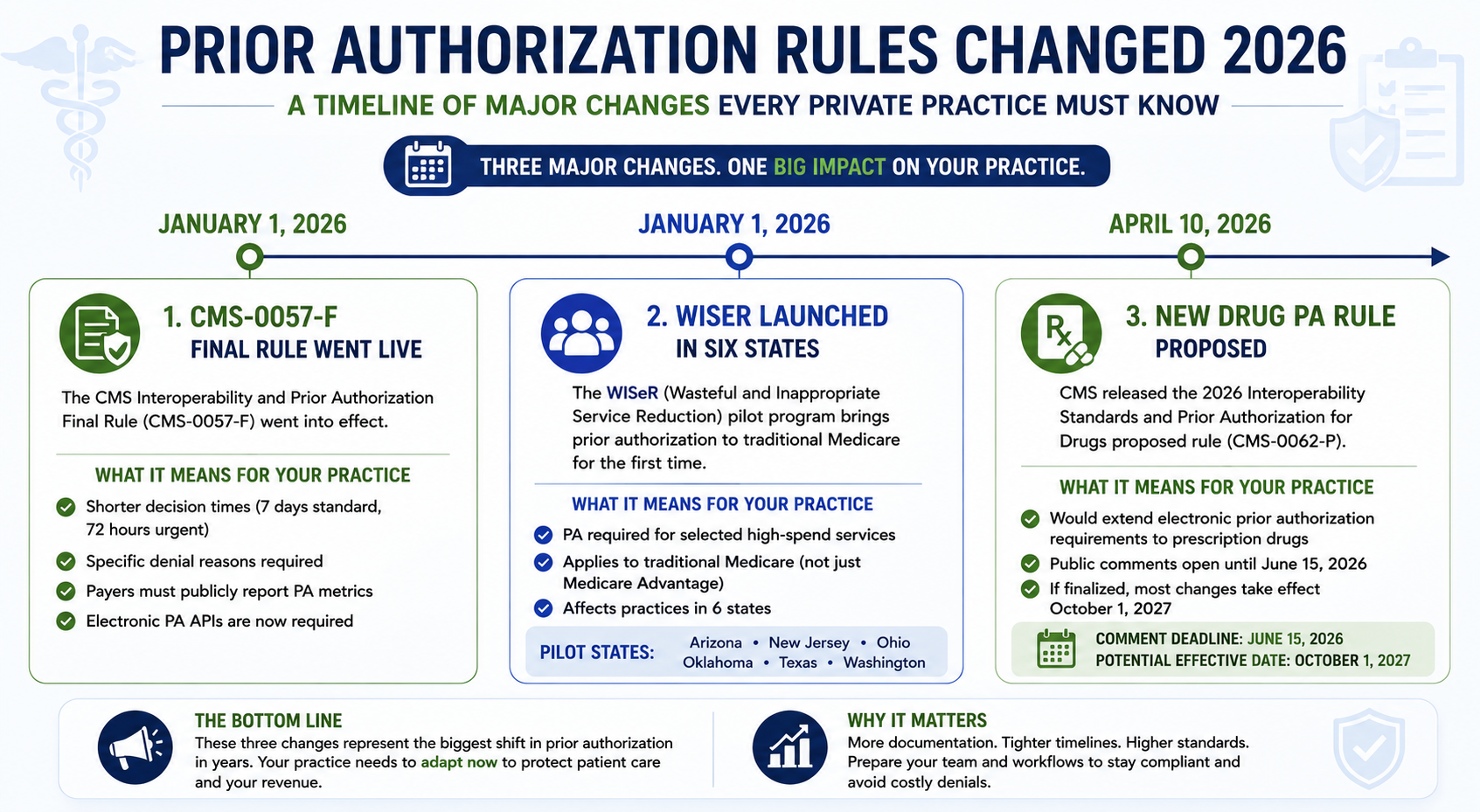
Three things shifted at the same time. A major CMS final rule kicked in that shortened decision windows and added mandatory denial reasons across Medicare Advantage, Medicaid, and commercial plans. A brand-new pilot program called WISeR brought prior authorization requirements into traditional Medicare for the very first time in decades. And a new proposed rule released in April 2026 is already setting up the next wave of changes — this time targeting prescription drug authorizations.
For private practices, this means more paperwork, tighter timelines, higher documentation standards, and a faster path to claim denial if your team is not caught up.
This guide breaks all of it down — what changed, when, who it affects, and exactly what your practice needs to do to protect its revenue and its patients in 2026.
Note from the ProHealth Care Advisors team: We work directly with private practices on prior authorization workflows and revenue cycle health. Everything in this guide reflects the actual CMS rules and operational guidance in effect as of May 2026. Visit ProHealth Care Advisors for hands-on support with your PA process.
The Big Picture — What Actually Changed on January 1, 2026
Three separate changes came into force in January 2026. Each one matters on its own. Together, they represent the biggest shift in prior authorization since the Affordable Care Act.
Change 1 — CMS-0057-F Final Rule Went Live
The CMS Interoperability and Prior Authorization Final Rule — officially called CMS-0057-F — went into operational effect on January 1, 2026. This rule had been finalized in January 2024 and gave payers two years to prepare. That preparation period is now over. The rule is active.
What it requires from payers — and what it means for your practice — is covered in detail below.
Change 2 — WISeR Launched in Six States
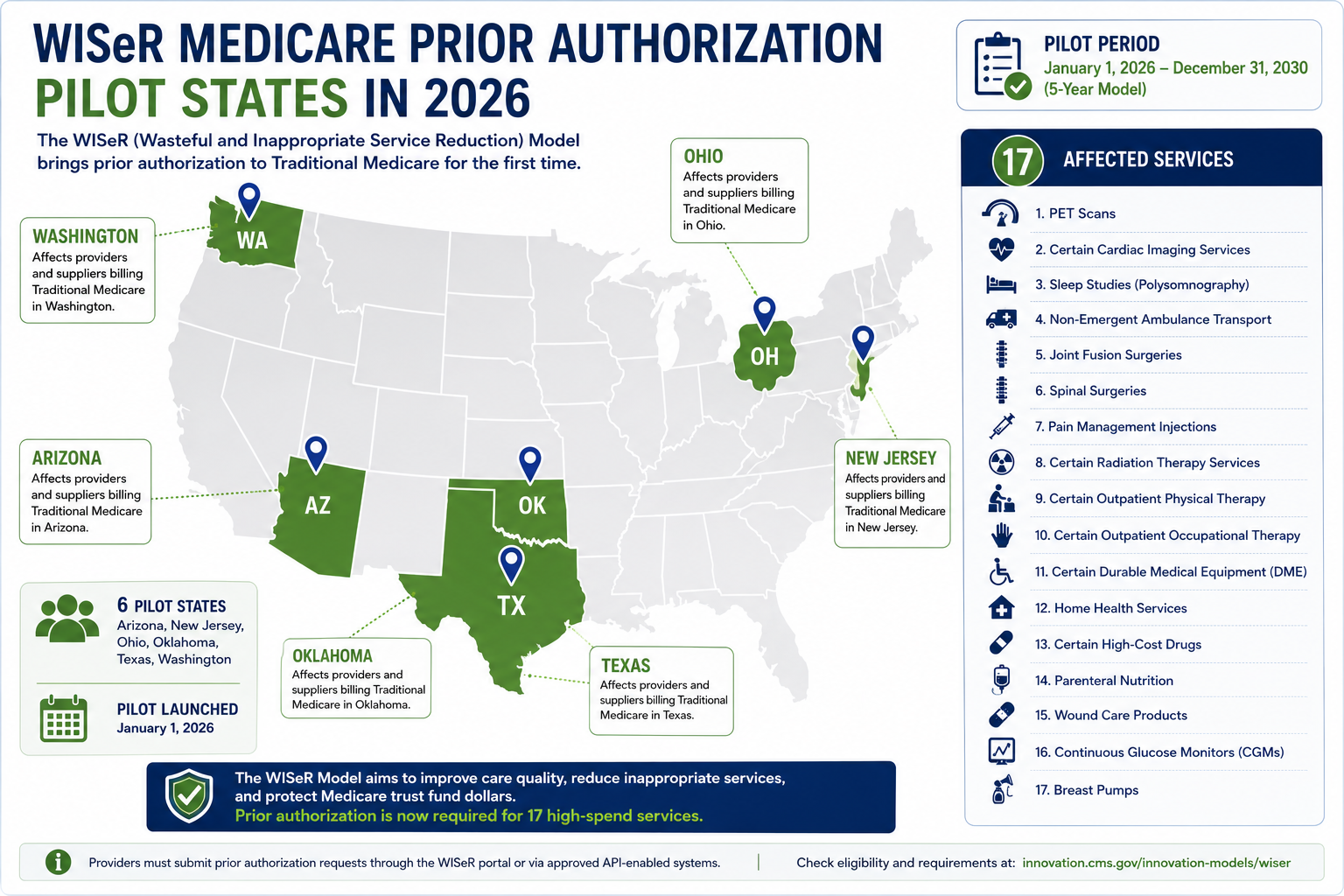
Also on January 1, 2026, the Center for Medicare and Medicaid Innovation launched a pilot program called the Wasteful and Inappropriate Service Reduction Model — known as WISeR. For the first time in decades, traditional Medicare now requires prior authorization for certain services. If your practice is in Arizona, New Jersey, Ohio, Oklahoma, Texas, or Washington, this affects you directly.
Change 3 — CMS Proposed New Drug PA Rules in April 2026
On April 10, 2026, CMS released the 2026 Interoperability Standards and Prior Authorization for Drugs proposed rule (CMS-0062-P). This rule proposes to extend electronic prior authorization requirements to prescription drugs — something the 2024 final rule did not cover. Public comments are open until June 15, 2026, and if finalized, most changes would take effect October 1, 2027. But practices should be watching this now.
What CMS-0057-F Actually Changed — And What It Means for Your Practice
CMS-0057-F applies to Medicare Advantage organizations, state Medicaid and CHIP fee-for-service programs, Medicaid managed care plans, CHIP managed care entities, and Qualified Health Plans on the Federal Exchange. If you bill any of these payers — and most private practices do — this rule directly affects your daily workflow.
Here is what changed in plain language:
Decision windows are shorter. Much shorter.
Before January 2026, payers could take up to 14 days to respond to a standard prior authorization request. That window is now cut to 7 calendar days. Urgent requests must be decided within 72 hours. This sounds like good news — and it is for patients. But it also means your practice needs to submit complete, documentation-ready requests the first time, because there is less buffer time to go back and forth.
Denials must now include a specific reason.
Under the old system, payers could issue vague denial language like “not medically necessary” with no further explanation. CMS-0057-F changed that. Every denial must now include a specific reason tied to coverage criteria. This matters because a specific reason is something you can actually appeal. Vague denials were designed to be difficult to challenge. Specific denials are something your team can work with.
Payers must publicly report PA metrics.
Starting in 2026, impacted payers are required to publicly report approval rates, denial rates, and appeal outcomes. This creates real accountability that did not exist before. It also gives your practice team a way to identify payers with unusually high denial rates on specific service types — information you can use to prepare stronger first submissions.
Electronic prior authorization APIs are required — with more coming.
CMS-0057-F requires impacted payers to implement FHIR-based Prior Authorization APIs. This means your electronic health record or practice management system can connect directly to payer systems to check whether PA is required, access documentation requirements, and submit requests — all without picking up the phone or logging into a payer portal. The API requirements have a full compliance deadline of January 1, 2027, but many payers have already begun implementation.
What this means for private practices right now:
If your PA workflow still relies heavily on phone calls and portal logins, you are running an inefficient process in a world that has moved on. The practices that updated their workflows to match these new rules are already seeing faster approvals and fewer denials. The ones that have not are absorbing the cost in staff time, delayed reimbursements, and preventable claim denials.
For help auditing your current PA process, see our Prior Authorization Support Services page.
WISeR — The Biggest Medicare Prior Auth Change in Decades
This is the change that caught many practices off guard — particularly those in the six pilot states who had never dealt with prior authorization requirements in traditional Medicare.
What WISeR is:
WISeR stands for Wasteful and Inappropriate Service Reduction. It is a six-year pilot program launched by the Center for Medicare and Medicaid Innovation, running from January 1, 2026 through December 31, 2031. It operates in six states: Arizona, New Jersey, Ohio, Oklahoma, Texas, and Washington.
The program uses artificial intelligence and human clinical review to evaluate prior authorization requests for 17 specific outpatient services that CMS identified as being at high risk for overutilization, fraud, waste, or abuse.
The 17 services currently covered under WISeR include:
Epidural steroid injections for pain management, percutaneous vertebral augmentation, spinal cord stimulators, peripheral nerve stimulators, knee replacement procedures, and several other outpatient procedures. The full current list is maintained on the CMS WISeR Model page.
How WISeR actually works:
Your practice submits a prior authorization request before providing one of the covered services. AI technology screens the request first, then a licensed clinician reviews any case where denial is being considered. CMS has stated that contractors are not incentivized to deny claims — they are measured on getting the determination right. Standard decisions come back within 72 hours. Expedited cases within 48 hours.
Once a prior authorization is approved, it is valid for 120 calendar days from the date of approval. If a request is denied, your practice can resubmit with additional documentation, and there is no limit on the number of resubmissions. Peer-to-peer clinical review is also available after a denial.
Providers with strong compliance records may eventually qualify for a “gold card” exemption — meaning they could bypass the WISeR review process for certain services based on their track record. Details on the gold card program are still being finalized as of mid-2026.
What private practices in WISeR states need to do:
First, know which services are on the list. If your practice provides any of the 17 covered services, you need a PA step built into your workflow before scheduling or performing those services.
Second, strengthen your medical necessity documentation. AI screening is looking for specific clinical indicators. Thin documentation that might have slipped through before will flag under WISeR. Every request needs to clearly justify the medical necessity of the service based on the patient’s documented clinical picture.
Third, train your billing staff on the 120-day approval validity window. Approvals expire. If a patient’s service date falls outside the window, you need a new authorization.
Fourth, track your WISeR approval and denial patterns from the start. If you are seeing higher-than-expected denials on a specific service type, that is a documentation workflow problem — and it is fixable.
For practices outside the six WISeR states: pay attention. The pilot runs through 2031, and if CMS deems it effective, expansion to additional states and services is likely. Building strong PA documentation habits now prepares you regardless of whether your state is currently included.
External resource: KFF — Examining the Potential Impact of Medicare’s New WISeR Model for an independent analysis of WISeR’s likely effects.
The April 2026 Drug PA Proposed Rule — What Is Coming Next
On April 10, 2026, CMS released CMS-0062-P, which proposes to extend prior authorization electronic requirements to prescription drugs. This is significant because the 2024 final rule only covered non-drug items and services, leaving a major gap in the electronic PA system.
If finalized, CMS-0062-P would:
- Require impacted payers to support electronic prior authorization for drugs covered under the medical benefit, including provider-administered therapies under Medicare Part B
- Set shorter, standardized timeframes for drug PA decisions
- Require payers to expand their FHIR-based Prior Authorization APIs to include drug-related requests
- Increase transparency in how drug PA decisions are made and communicated
Public comments on this proposed rule are open until June 15, 2026. If you want your practice’s voice included, the CMS comment submission portal is where to go.
Most changes, if finalized, would go into effect October 1, 2027. This gives practices roughly 16 months from now to prepare. But preparation should start before the rule is finalized — the direction of travel is clear, and practices that wait for implementation dates to act tend to scramble.
External resource: CMS — 2026 Interoperability Standards and Prior Authorization for Drugs Proposed Rule for the full rule text and fact sheet.
How These Changes Affect Private Practice Revenue Right Now
Let us talk about money — because that is ultimately what makes these regulatory changes feel real in a day-to-day clinical environment.
The first-pass PA approval rate gap is widening.
Industry baseline for first-pass prior authorization approval sits around 75%. The top-performing practices are hitting 92% or higher. That 17-point gap represents real, recoverable revenue. With decision windows now shorter and documentation standards higher under the 2026 rules, practices that have not updated their workflows are falling further behind that 92% benchmark every month.
Denials are costing more to work.
A denied PA request used to be an inconvenience. Under the new rules, it is a more complex process — because specific reasons mean specific appeal arguments, and appeal arguments require clinical staff time. Practices that did not build a denial management workflow before 2026 are now absorbing that administrative cost unplanned.
Cash flow is more sensitive to PA delays.
With tighter 7-day decision windows, a PA that falls through the cracks — a request that was submitted with incomplete documentation and did not surface as a priority — can delay a patient’s service and push a reimbursable encounter out by weeks. That delay multiplied across dozens of patients adds up to a meaningful cash flow disruption for a private practice.
Practices with strong PA workflows are actually benefiting from the 2026 changes.
Here is the counterintuitive part. Practices that have solid documentation standards, use electronic PA tools, and track denial patterns are finding that the 2026 rules work in their favor. Shorter payer decision windows mean faster approvals. Mandatory denial reasons mean more successful appeals. Public payer reporting means better data for first-submission strategy. The rules reward preparation.
For a full evaluation of how your current PA performance compares to 2026 benchmarks, our Revenue Cycle Health Check walks through the key metrics.
7 Steps to Update Your Prior Authorization Workflow for 2026
This is the practical section. Use it as a working checklist.
Step 1 — Identify every payer you bill that is covered by CMS-0057-F. Medicare Advantage, Medicaid managed care, CHIP, and Federal Exchange QHPs all fall under the new rules. Pull your payer mix and mark each one.
Step 2 — Verify that each covered payer’s decision timelines are being met. Under CMS-0057-F, standard decisions must come back within 7 days. Urgent within 72 hours. If payers are exceeding these windows, you have grounds to escalate. Document the dates you submit and the dates you receive decisions.
Step 3 — Build a documentation template for every service that regularly requires PA. Templates should include the clinical indicators payers look for, the specific diagnosis and procedure codes, and the patient-specific medical necessity language your clinicians need to provide. Do not leave this to individual staff discretion.
Step 4 — If your practice is in a WISeR state, map all 17 covered services against your service mix. For every service that overlaps, add a PA step to your scheduling workflow before the appointment is booked. PA approval must be in hand before service delivery.
Step 5 — Build a same-day denial routing process. Every denial should be routed on the day it is received to a designated person responsible for triage, appeal preparation, or peer-to-peer review request. Sitting on denials is where practices lose money they actually earned.
Step 6 — Track your PA outcomes by payer and by service type. Monthly data on approval rates, denial rates, and appeal outcomes by payer gives you the intelligence to improve first-submission quality. Without this data, you are reacting to problems instead of preventing them.
Step 7 — Ask your billing vendor or team whether they are using FHIR-based electronic PA tools. The 2026 rules are pushing the industry toward electronic submission. If your practice is still managing PA primarily through phone calls and manual portal entries, you are spending significantly more staff time than practices using integrated electronic tools.
For support implementing any of these steps, see our Medical Billing and Practice Management Services page.
Georgia Private Practices — What These Changes Mean Specifically for You
Georgia is not one of the six WISeR pilot states, which means traditional Medicare prior authorization requirements have not expanded for Georgia practices yet. But the rest of the 2026 changes apply fully.
Georgia Medicaid managed care — through Amerigroup, Peach State Health Management, and WellCare — falls under the CMS-0057-F requirements. Each CMO has its own documentation standards layered on top of the CMS baseline rules, and each has its own history of denial patterns that your PA team needs to know.
The 7-day standard and 72-hour urgent decision windows apply to your Medicaid managed care claims. The mandatory denial reason requirement applies. And the electronic PA API requirements — as payers complete their implementation through January 2027 — will change how your team submits requests.
For Georgia private practices that have been struggling with Medicaid PA delays or high denial rates, the 2026 rules create a real opportunity to push back more effectively. A specific denial reason from Amerigroup or Peach State is something your team can appeal with a documented clinical argument. That was harder to do under the old vague denial language.
For more on how Georgia Medicaid’s specific requirements interact with the new CMS rules, see our Georgia Medical Billing Guide for private practices.
External resource: Georgia Medicaid Division — Provider Information for current Georgia Medicaid PA requirements.
Frequently Asked Questions — Prior Authorization Rules Changed 2026
What is CMS-0057-F and when did it take effect?
CMS-0057-F is the CMS Interoperability and Prior Authorization Final Rule, finalized in January 2024 and effective January 1, 2026. It requires impacted payers — including Medicare Advantage, Medicaid managed care, CHIP, and Federal Exchange QHPs — to respond to standard PA requests within 7 days, provide specific reasons for all denials, and publicly report their PA metrics.
What is the WISeR model and which states does it affect?
WISeR stands for Wasteful and Inappropriate Service Reduction. It is a six-year Medicare prior authorization pilot launched January 1, 2026, in Arizona, New Jersey, Ohio, Oklahoma, Texas, and Washington. It covers 17 outpatient services identified as high-risk for overuse or fraud, using AI and human clinical review to evaluate requests. Standard decisions come back within 72 hours.
Does the 7-day PA decision window apply to all insurance payers?
It applies to Medicare Advantage organizations, state Medicaid and CHIP fee-for-service programs, Medicaid managed care plans, CHIP managed care entities, and Qualified Health Plans on the Federal Exchange. It does not apply to fully insured commercial plans or self-funded employer plans, though many commercial payers are adopting similar timelines voluntarily.
What happens if a payer takes longer than 7 days to decide on a prior authorization?
Under CMS-0057-F, impacted payers are required to meet the 7-day standard decision window. If a payer is consistently exceeding this window, you can document the pattern and escalate through the payer’s grievance process or report the violation to CMS. The new public reporting requirements also mean these patterns will become visible in payer compliance data.
My practice is not in a WISeR state. Does any of this still apply to me?
Yes. CMS-0057-F applies regardless of which state your practice is in, as long as you bill Medicare Advantage, Medicaid managed care, CHIP, or Federal Exchange QHPs. The WISeR pilot is state-limited for now, but the new CMS final rule requirements are national.
What is the new proposed rule on drug prior authorizations?
On April 10, 2026, CMS released CMS-0062-P, which proposes to extend electronic prior authorization requirements to prescription drugs and provider-administered therapies under the medical benefit. Public comments are open until June 15, 2026. If finalized, most changes would take effect October 1, 2027.
How do I know if my current prior authorization process is ready for the 2026 rules?
The key metrics to check are your first-pass PA approval rate (target 90% or higher), your average time from PA submission to decision by payer, and your denial overturn rate. If you do not have visibility into those numbers right now, that is a workflow gap that needs to be addressed before it costs your practice more. Our Revenue Cycle Health Check is a good starting point.
Will WISeR expand to more states after 2026?
Possibly. CMS has designed WISeR as a test model, running through December 31, 2031. If the pilot demonstrates meaningful reduction in fraud, waste, and abuse without significant negative patient impact, CMS could expand it to additional states or service categories. Practices outside the current six states should treat this as a reason to strengthen PA documentation habits now rather than waiting.