Mental Health Billing 2026 — The Complete Guide for Therapists, Psychiatrists, and Behavioral Health Practices
Here is a number that stops most behavioral health practice owners cold.
For a typical three-therapist group practice, billing errors, denials, and write-offs translate to $85,000 to $120,000 in lost annual revenue.
Not because the care was not delivered. Not because the patients did not have insurance. Because the mental health billing process failed somewhere between the session and the payment — and most of the time, nobody caught it until months later, when the revenue was already gone.
Mental health providers face denial rates averaging 16 to 20 percent — more than double the 5 to 10 percent rate for general medical practices. Recent Office of Inspector General reports show that approximately 61 percent of mental health Medicare claims contain some type of regulatory error. Most practices never appeal denied claims — they simply write off the revenue.
According to the National Institute of Mental Health, nearly 1 in 5 US adults lives with a mental illness — meaning the volume of behavioral health claims being processed is enormous, and the financial impact of billing errors compounds at scale.
This guide is for therapists, psychiatrists, psychologists, counselors, and behavioral health practice managers who want to understand exactly why mental health billing is this difficult — and what it takes to stop losing revenue to billing errors that are almost entirely preventable.
Why Mental Health Billing Is More Complex Than General Medical Billing
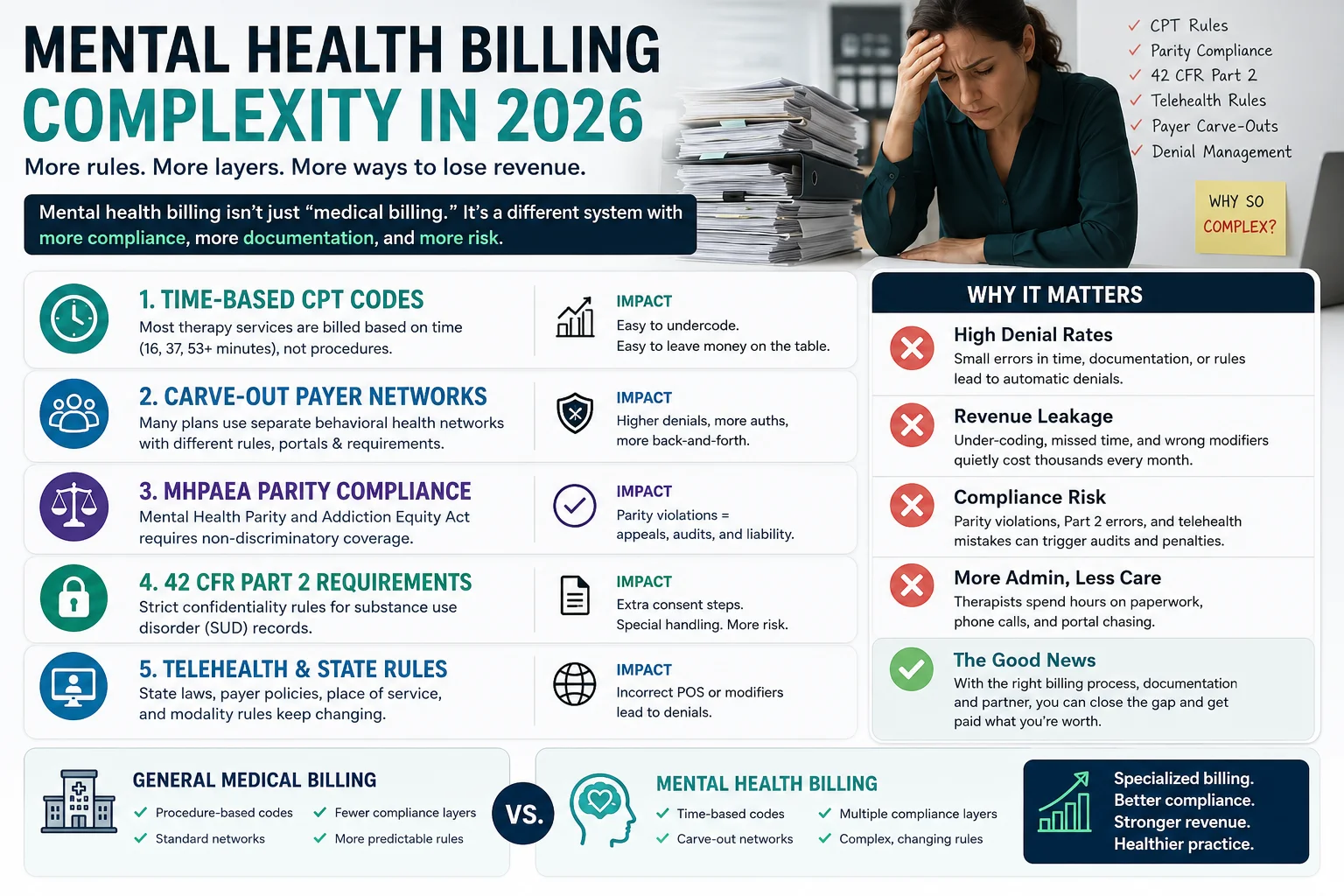
Most billing systems — and most billing teams — are built for medical billing. They understand procedure codes, diagnosis codes, and fee-for-service claims.
Mental health billing is fundamentally different in ways that generic billing processes consistently fail to handle:
Mental health billing is more complicated compared to other specialties because of interactions with federally backed programs like Medicare and Medicaid, commercial payors, and self-pay patients. The dependence on specific, time-based CPT and ICD-10 codes makes mental health billing intricate — based on session duration, billers must carefully use codes like 90832 or 90837.
Here is what makes it specifically different:
Time-based CPT codes. Unlike most medical procedures where a code corresponds to what was done, mental health CPT codes correspond to how long the session lasted. A 45-minute session uses a different code than a 60-minute session. Billing the wrong time-based code — even by a few minutes of undocumented time — generates a denial or creates audit risk.
Carve-out payer networks. Many commercial insurance plans — Anthem, Cigna, UnitedHealthcare — delegate mental health benefits to separate managed behavioral health organizations (MBHOs): Magellan, Carelon Behavioral Health, Optum Behavioral Health. When a patient has a carve-out plan, the claim must go to the MBHO — not to the commercial carrier on the insurance card. A practice that does not identify carve-outs at eligibility verification will submit claims to the wrong entity, generating denials that look like coverage problems but are actually routing errors.
Mental Health Parity compliance. The Mental Health Parity and Addiction Equity Act (MHPAEA) requires insurance plans to cover mental health services comparably to medical services — but parity violations remain common and create specific denial appeal opportunities that most billing teams do not know to use.
42 CFR Part 2 confidentiality requirements. For practices treating substance use disorders, 42 CFR Part 2 — updated effective February 2026 — creates strict patient consent and record-sharing requirements that directly affect what documentation can be shared with payers.
Multiple overlapping regulations. Between HIPAA privacy rules, 42 CFR Part 2 requirements, Mental Health Parity Act protections, state licensing laws, and payer-specific policies, mental health providers navigate more complex regulations than almost any other specialty. Missing even one requirement can trigger denials or audit findings.
The Essential Mental Health CPT Codes for 2026
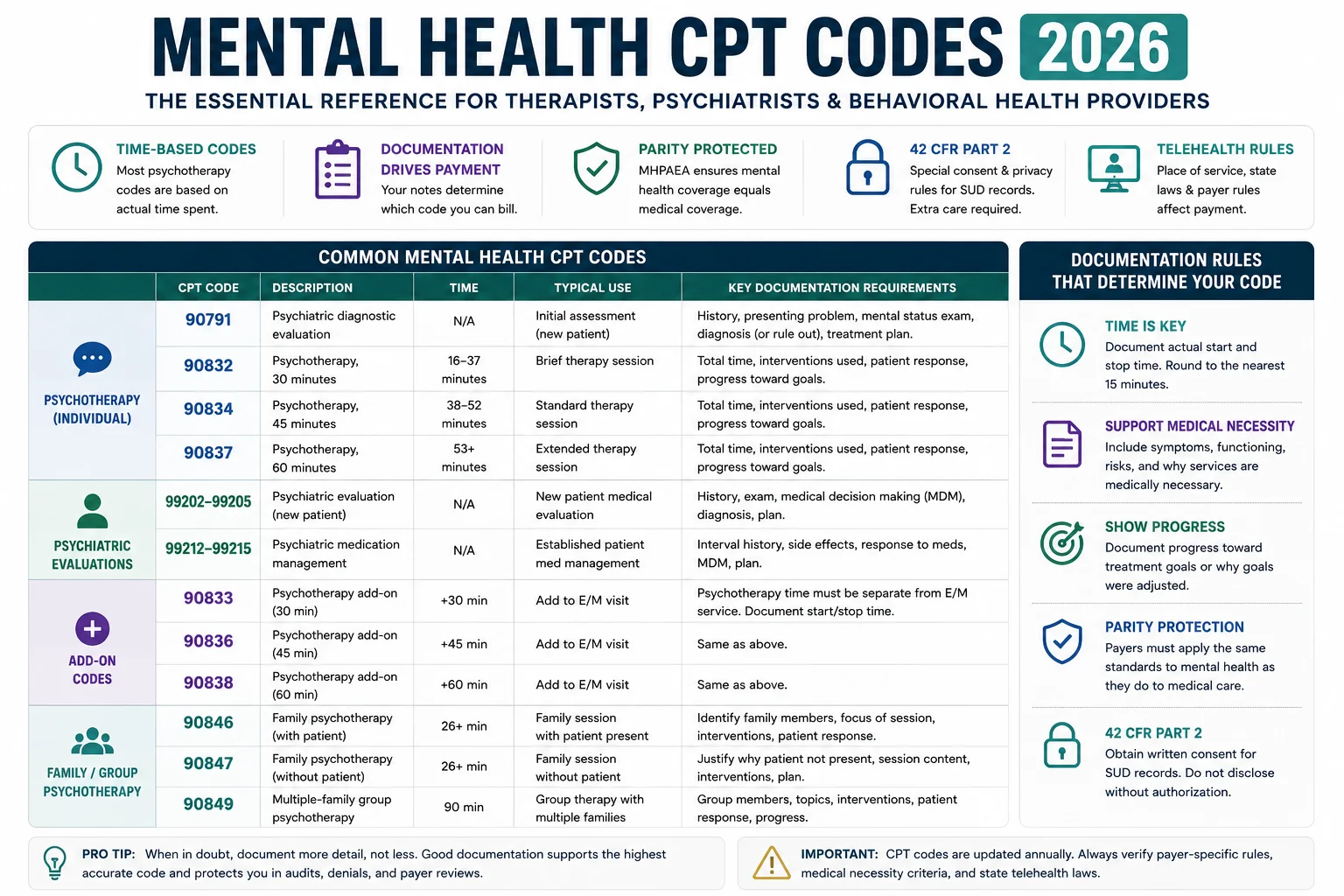
Here are the common codes that billers and coders specializing in behavioral health must know in 2026:
Diagnostic Evaluation Codes
| CPT Code | Description | Key Notes |
|---|---|---|
| 90791 | Psychiatric diagnostic evaluation without medical services | Initial evaluation — no prescribing component |
| 90792 | Psychiatric diagnostic evaluation with medical services | Initial evaluation — includes prescribing/medication review |
Individual Psychotherapy Codes — Time-Based
| CPT Code | Session Duration | Billable Time Range |
|---|---|---|
| 90832 | 30-minute psychotherapy | 16–37 minutes |
| 90834 | 45-minute psychotherapy | 38–52 minutes |
| 90837 | 60-minute psychotherapy | 53+ minutes |
CPT time descriptors are the primary audit lever for psychotherapy codes. Payers frequently apply edits that require documentation of session start and stop times and total psychotherapy minutes when reviewing 90837 claims.
Critical rule: Simply writing “60-minute session” is insufficient. Document the exact start time and stop time on every session note. This is the single most audited element of mental health billing.
Family and Group Therapy Codes
| CPT Code | Description |
|---|---|
| 90846 | Family psychotherapy without patient present |
| 90847 | Family psychotherapy with patient present |
| 90853 | Group psychotherapy |
Add-On and Crisis Codes
| CPT Code | Description |
|---|---|
| 90833 | Individual psychotherapy add-on (30 min) with E/M |
| 90836 | Individual psychotherapy add-on (45 min) with E/M |
| 90838 | Individual psychotherapy add-on (60 min) with E/M |
| 99483 | Cognitive impairment assessment |
| 90839 | Crisis psychotherapy, first 60 minutes |
| 90840 | Crisis psychotherapy, each additional 30 minutes |
Telehealth Modifiers for Mental Health in 2026
Telehealth modifiers include: modifier 95 or GT (when required by the payer), audio-only modifiers FQ or FR (for programs that distinguish audio-only from video), and modifier 59 or related X modifiers for distinct procedural services. Confirm the right place of service for each encounter based on where the patient is located.
| Modifier | Use |
|---|---|
| 95 | Synchronous telehealth (most commercial payers) |
| GT | Medicare/Medicaid telehealth (live video) |
| FQ | Audio-only telehealth |
| FR | Supervision via telehealth |
Place of service codes for telehealth mental health in 2026:
- POS 02 — Telehealth (patient not at home)
- POS 10 — Patient’s home as originating site
What Changed in Mental Health Billing in 2026 — The Key Updates
1. 42 CFR Part 2 Full Enforcement — February 16, 2026
Full enforcement of updated 42 CFR Part 2 began February 16, 2026. These regulations govern the confidentiality of substance use disorder patient records — and the 2026 update made significant changes to how these records can be shared with payers, other providers, and healthcare operations.
Work only with billing vendors who understand Part 2 requirements and have appropriate safeguards in place. Consider consulting with legal counsel specializing in behavioral health to ensure your Part 2 compliance program is robust.
What this means for billing: practices treating substance use disorders must ensure that their billing documentation does not inadvertently disclose Part 2-protected information without appropriate patient consent. Billing claims, prior authorization requests, and appeal documentation all need to be reviewed for Part 2 compliance before submission.
2. MHPAEA Parity Enforcement Is Now Aggressive
The 2024 MHPAEA final rule strengthened nonquantitative treatment limitation standards. For behavioral health organizations, the 2024 rule has two direct billing implications: prior authorization denials for mental health or SUD services not required for comparable medical services are now legally vulnerable to challenge under parity. Payers must make their comparative analysis available to plan participants and state regulators upon request — creating an audit trail that behavioral health organizations can access and use in denial appeals.
Health plans are now required to conduct and provide comparative analyses proving their mental health utilization management is not more restrictive than medical processes. For your billing team, this means you can push back harder on arbitrary session limits and prior authorization denials.
This is a significant billing opportunity that most practices are not using. When a prior authorization is denied for a mental health service — and that same payer does not require prior authorization for a comparable medical service — you now have a legal basis to challenge the denial under parity. Your billing team should be documenting these comparisons and including parity references in appeal letters.
3. Telehealth Extended Through 2027 — But Rules Are Tightening
Medicare’s extension of telehealth flexibilities through 2027 offers rare stability for tele-mental health and addiction treatment programs. According to the CMS Telehealth Services page, this extension specifically covers mental health and substance use disorder services — good news for practices that have built significant telehealth volume.
However, in 2026, 40 to 60 percent of therapy sessions occur via telehealth — and this creates billing compliance challenges because telehealth rules keep changing.
Key telehealth billing errors causing denials in 2026 include: missing or incorrect telehealth modifiers, incorrect place of service codes, inadequate time-based documentation, and authorization and eligibility failures.
Telehealth compliance continues evolving in 2026. Errors in POS selection, modifier usage, or consent documentation are among the most common audit flags. High telehealth utilization patterns can increase audit risk, especially when practices bill nearly 100 percent of visits as virtual services.
4. Electronic Prior Authorization Is Now Mandatory
CMS mandates make electronic prior authorization the standard for 2026. Payers are eliminating faxed prior authorizations, requiring digital submission through specific electronic PA systems. Practices still using faxes and manual uploads will experience growing denials, compliance gaps, and delays.
The American Medical Association’s prior authorization resources confirm that prior authorization burden has reached a critical point — physicians now spend an average of 14.5 hours per week on PA tasks alone.
If your practice is still faxing prior authorization requests to any major commercial payer in 2026, you are already behind — and the resulting authorization gaps are generating CO-15 denials every week. For more on the 2026 prior authorization rule changes, see our prior authorization rules changed 2026 guide.
5. Social Determinants of Health Coding Now Affects Reimbursement
ICD-10 updates now emphasize coding for social and environmental factors affecting mental health — housing stability, financial strain, transportation access, food security, substance use environment. A clinician documenting “patient reports housing instability” must now translate that into accurate ICD-10 codes that capture the full clinical picture and drive reimbursement accuracy. For a 10-provider practice, missing SDoH codes could translate to thousands in lost revenue annually.
The 8 Most Common Mental Health Billing Errors — And How to Prevent Each One
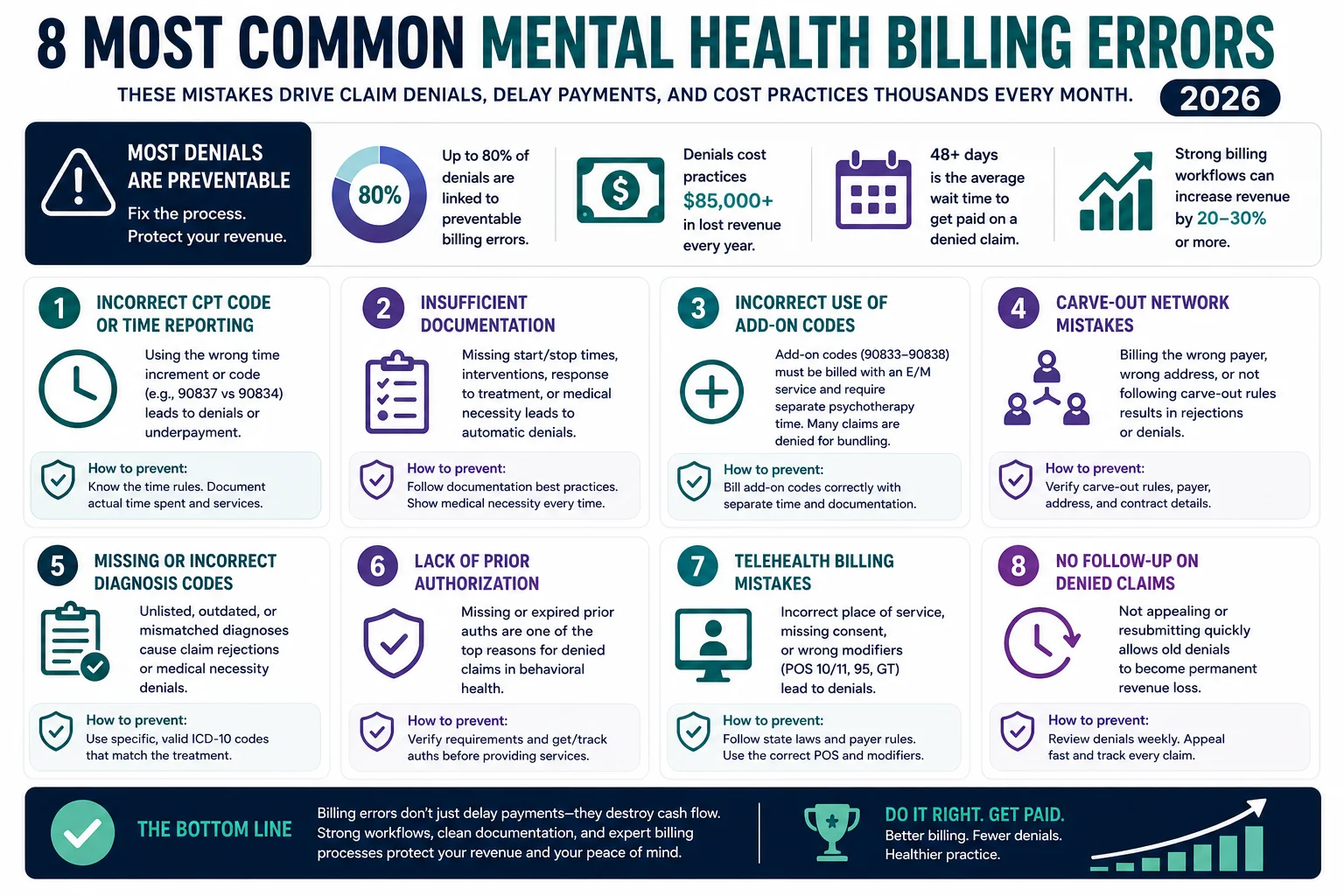
Error 1: Insufficient Time Documentation on 90837 Claims
CPT 90837 is the 60-minute individual psychotherapy code — and it is also the most audited mental health CPT code in the country. CPT 90837 is one of the most audited psychotherapy codes — higher reimbursement draws greater scrutiny.
Simply writing “60-minute session” is insufficient. Your note must document the exact start time, stop time, and total psychotherapy minutes. Anything less creates audit vulnerability — and payers are actively using analytics to identify 90837 claims without time documentation.
Fix: Build a documentation template that requires start time, stop time, and total session minutes on every psychotherapy note.
Error 2: Submitting to the Wrong Payer Due to Carve-Out Plans
A small practice that does not identify carve-out plans at eligibility verification will submit claims to the wrong entity — generating denials that look like coverage problems but are actually routing errors. Miss the 90-day timely filing window on those misdirected claims and the revenue is gone permanently.
Fix: Build a carve-out identification step into your eligibility verification process. When verifying insurance, specifically check whether mental health benefits are managed by a separate MBHO — and capture that payer information before the first claim goes out.
Error 3: Missing or Wrong Telehealth Modifiers
Telehealth billing requires specific modifiers — and the correct modifier depends on the payer, the modality (video vs. audio-only), and the patient’s location. Using modifier 95 when a payer requires GT, or failing to append FQ for audio-only sessions, generates denials that are entirely avoidable.
Fix: Build a payer-specific telehealth modifier reference list. Do not assume the same modifier works for every payer. For our prior authorization and telehealth workflows, the payer-specific detail matters enormously.
Error 4: Missing Prior Authorization — Especially for Ongoing Therapy
Commercial payers require prior authorization for ongoing outpatient therapy, and IOP or PHP programs require concurrent review every 7 to 10 days. Missing a concurrent review window means the claims for that period deny. For a week of IOP at $4,000 to $6,000 per patient, one missed review window is a significant cash flow hit.
Fix: Build a systematic prior authorization tracking workflow — not a spreadsheet that gets checked inconsistently, but a structured process that flags upcoming authorization expirations before services are rendered. Our creative collection solutions include prior authorization management as part of our denial prevention workflow.
Error 5: Not Appealing Denials Under Parity Law
Denial abandonment is the quiet killer. The average behavioral health first-pass denial rate runs 18 to 22 percent. Of those denials, an estimated 65 percent are never appealed — they are written off because no one has time to work them. For a practice billing $300,000 annually, that is approximately $20,000 to $40,000 in recoverable revenue abandoned every year.
Specifically for mental health practices, many of these abandoned denials are parity violations that would be overturned on appeal if the billing team knew to reference MHPAEA. A prior authorization denial for outpatient psychotherapy when the same payer does not require PA for comparable medical services is a parity violation — and it is now legally required to be challenged.
Fix: Build a denial appeal workflow that specifically identifies potential parity violations. When a mental health PA is denied, check whether a comparable medical service requires the same authorization. If not, document the comparison and include the MHPAEA reference in your appeal. See our complete denial codes guide for appeal strategies.
Error 6: Billing Under the Wrong NPI When Supervised
Mental health practices with supervised clinicians — interns, residents, supervised counselors — must bill correctly for supervised services. Billing under the supervisor’s NPI when the services should be billed under the supervised clinician’s NPI (or vice versa) generates compliance violations and potential audit findings.
Fix: Establish clear internal billing protocols for supervised clinician billing that match each payer’s specific requirements. Not all payers handle supervised billing the same way. Our physician credentialing service handles NPI setup and payer enrollment for supervised providers.
Error 7: Incorrect Place of Service Code for Telehealth
Place of service codes for behavioral health are one of the most common billing errors in 2026 — the wrong two-digit field, and clean claims get denied. POS 02 is used when the patient is at a facility; POS 10 is used when the patient is at home.
Fix: Train billing staff on the 2026 telehealth POS requirements. Build a quick reference into your billing workflow — POS 10 for patients at home, POS 02 for patients at another facility. Always confirm which POS codes each payer contract recognizes for telehealth.
Error 8: Credentialing Gaps for New Providers
Credentialing gaps create billing gaps: Revenue is often lost during the period between a provider’s start date and payer enrollment approval. Confirm provisional billing policies with each payer before a new clinician begins seeing patients.
Commercial credentialing takes 90 to 120 days. During that window, the provider cannot bill insurance.
Fix: Start credentialing every new provider the day their start date is confirmed — not the day they arrive. Submit to all payers simultaneously. And manage credentialing through the same company that handles your billing so enrollment status and billing workflows are synchronized. See our physician credentialing guide for full details.
Mental Health Prior Authorization in 2026 — What Changed and What to Do
Prior authorization is the single biggest operational challenge in mental health billing. CMS mandates make electronic prior authorization the standard for 2026. Payers are eliminating faxed prior authorizations, requiring digital submission through specific ePA systems.
Here is what has specifically changed and what your practice must do:
Decision windows are shorter. Under CMS-0057-F, standard prior authorization requests must now be decided within 7 calendar days — down from 14 days previously. Urgent requests must be decided within 72 hours. This means your practice needs to submit complete, documentation-ready requests the first time, because there is less buffer time to go back and forth.
Denial reasons must now be specific. Payers can no longer issue vague “not medically necessary” denials. Every denial must now include a specific reason tied to coverage criteria — which makes appeals more actionable because a specific reason is something you can actually challenge.
Parity gives you new appeal leverage. When a mental health PA is denied — particularly for outpatient therapy, IOP, or PHP — evaluate whether a comparable medical service would require the same authorization. If not, you have a parity violation on your hands that can be appealed under MHPAEA with documented comparative analysis.
Electronic submission is mandatory. If you are still faxing prior authorization requests to commercial payers in 2026, you are generating avoidable denials. Every major commercial payer now has an electronic PA portal or ePA integration. Your billing workflow must route PA requests through these systems.
For the complete 2026 prior authorization rule picture — including the WISeR pilot program, the new proposed drug PA rule, and what all of this means operationally — see our prior authorization rules changed 2026 guide.
Mental Health Denial Rates in 2026 — Why They Are So High and What Drives Them
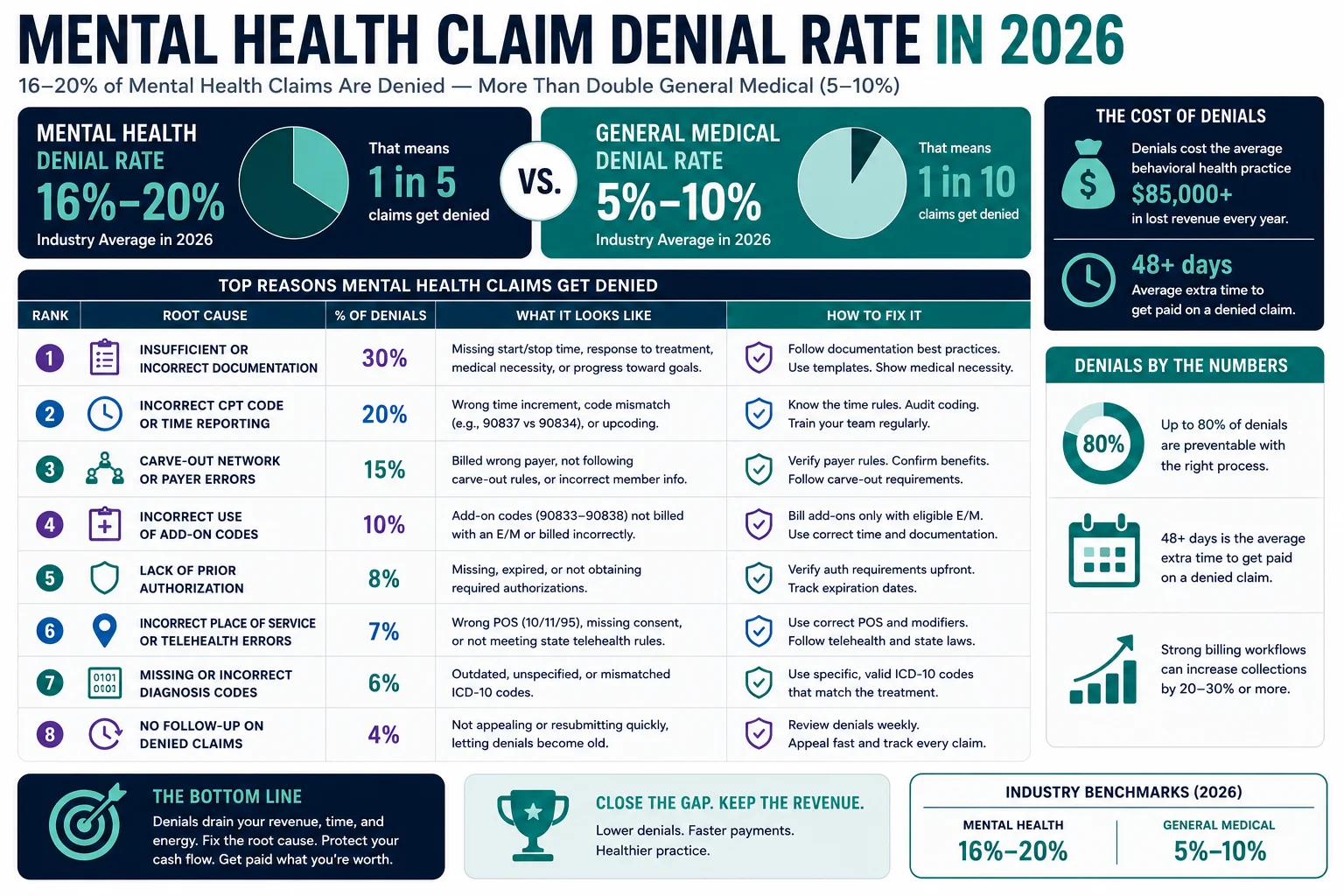
Mental health providers face denial rates averaging 16 to 20 percent — more than double the 5 to 10 percent rate for general medical practices.
This is not a random distribution. The same denial types appear repeatedly across mental health practices nationwide — which means they are almost entirely preventable. Here are the most common denial drivers in behavioral health billing in 2026:
Authorization errors (CO-15): Missing authorization, expired authorization, or authorization obtained for the wrong service or provider. In mental health, this is amplified by the carve-out problem — authorization obtained from the commercial carrier when the MBHO manages benefits generates a denial regardless of the authorization’s validity.
The HHS Office of Inspector General has specifically identified mental health billing as a high-priority audit focus area — with approximately 61 percent of reviewed Medicare mental health claims containing documentation or coding errors.
Eligibility verification failures (OA-23, CO-22): Patient’s mental health benefits managed by a carve-out MBHO that was not identified at verification. Insurance changed since the last check. Benefits were verified for the wrong payer entity.
Incorrect psychiatric coding: Wrong time-based code selected, or time documentation insufficient to support the billed code. 90837 billed without documented start/stop times. Add-on codes billed incorrectly alongside primary codes.
Telehealth modifier mistakes: Wrong modifier for the payer, wrong place of service code, or missing modality documentation in the clinical note.
Poorly documented session times: Time-based coding miscalculations are a major risk in behavioral health billing. If the exact time range is not recorded — such as simply stating “60-minute session” without start and stop times — claims for 90832, 90834, or 90837 may trigger audits or denials.
Session limit violations: Authorization and session limit violations are a frequent source of behavioral health denials. When services exceed approved units, payers often deny claims automatically regardless of medical necessity.
For a complete breakdown of denial codes — including CO-15, CO-11, CO-50, and OA-23 — and exactly what to do when each one appears on your EOB, see our complete medical billing denial codes guide.
Behavioral health billing is uniquely complex. Generic medical billing processes often fail to capture the nuances of psychiatry and substance abuse claims.
Pro Health Care Advisors provides specialized mental health and behavioral health billing through our mental health billing and credentialing services — with AAPC-certified billers who understand the specific requirements of behavioral health coding, carve-out network routing, parity appeal strategies, and 42 CFR Part 2 compliance.
Here is specifically what we do for mental health practices:
Carve-out identification at eligibility verification. Every patient insurance check includes identification of behavioral health carve-out MBHOs — ensuring claims are routed to the correct entity from the first submission.
Time-based coding review. Our AAPC-certified coders verify that every psychotherapy claim includes the documentation required to support the billed time-based code — catching documentation gaps before they become CO-50 denials or audit findings. Our CodeMAXX services add a dedicated coding accuracy layer for exactly these patterns.
Electronic prior authorization management. We manage ePA submissions through payer-specific electronic systems — eliminating the CO-15 denials generated by faxed or manual authorization submissions.
Parity-based denial appeals. When mental health authorization denials appear that may violate MHPAEA, our billing team identifies the parity basis for appeal and includes the documented comparative analysis in the appeal letter.
42 CFR Part 2 compliant billing documentation. For substance use disorder practices, we ensure that billing documentation handles Part 2-protected information in compliance with the February 2026 update.
Telehealth modifier accuracy. Our billing team maintains a payer-specific telehealth modifier and POS reference — ensuring every telehealth claim uses the correct modifier and place of service code for each specific payer.
Credentialing for supervised providers. We handle NPI setup and payer enrollment for supervised clinicians — preventing the billing gaps that generate when a supervised provider starts seeing patients before their enrollment is active. See our physician credentialing service for details.
Denial recovery. Our creative collection solutions recover the denied claims that most mental health billing teams write off — including aged claims from previous billing operations.
The result: a 98.5 percent clean claim rate and a denial rate under 2 percent — compared to the 16 to 20 percent denial rate the average mental health practice absorbs.
Frequently Asked Questions — Mental Health Billing 2026
Q: What CPT code is used for a 60-minute therapy session? CPT 90837 is the individual psychotherapy code for sessions of 53 minutes or more. Documentation must include the exact start time, stop time, and total minutes of psychotherapy. 90837 is the most audited mental health CPT code — time documentation is not optional, it is mandatory.
Q: What is a carve-out in mental health billing and why does it matter? A carve-out is when a commercial health plan delegates mental health benefits to a separate managed behavioral health organization (MBHO) — such as Magellan, Optum Behavioral Health, or Carelon Behavioral Health. When a patient has a carve-out plan, the mental health claim must be submitted to the MBHO, not to the commercial carrier on the insurance card. Submitting to the wrong entity generates a denial — and if the timely filing window closes before the error is caught, the revenue is permanently lost.
Q: What changed in 42 CFR Part 2 in 2026? Full enforcement of updated 42 CFR Part 2 regulations began February 16, 2026. These regulations govern confidentiality of substance use disorder patient records. The 2026 update changed consent requirements and record-sharing rules — billing documentation for SUD treatment must now be reviewed for Part 2 compliance to ensure protected information is not inadvertently disclosed in claims or prior authorization requests.
Q: Why are mental health claim denial rates so much higher than other specialties? Mental health billing has several features that generate above-average denials: time-based codes that require precise documentation, carve-out payer routing that is missed at eligibility verification, prior authorization requirements for ongoing therapy, complex telehealth modifier rules, and 42 CFR Part 2 compliance requirements. The average behavioral health denial rate is 16 to 20 percent — compared to 5 to 10 percent for general medical practices — primarily because generic billing processes were not built for these specific requirements.
Q: What is MHPAEA and how does it affect billing? The Mental Health Parity and Addiction Equity Act requires health plans to cover mental health and substance use disorder services comparably to medical and surgical services. Under the 2024 MHPAEA final rule — now fully enforced — payers must prove their mental health utilization management is no more restrictive than for comparable medical services. For billing, this means prior authorization denials for mental health services that would not be required for comparable medical services can be challenged as parity violations in the appeal process.
Q: How long does it take for mental health providers to get credentialed? Commercial payer credentialing typically takes 90 to 120 days. During that period, a new provider cannot bill insurance for services rendered. Start credentialing every new provider the day their start date is confirmed. For our complete credentialing timeline guide, see our physician credentialing guide.
Q: Does Pro Health Care Advisors handle behavioral health billing specifically? Yes. Our mental health billing services include specialized billing for therapists, psychiatrists, psychologists, and behavioral health group practices — with AAPC-certified coders who understand carve-out routing, time-based codes, parity appeals, and 42 CFR Part 2 compliance. For more on how mental health billing fits into the broader revenue cycle, see our revenue cycle management guide.
For more billing education and resources, visit our articles and resources library.