Physician Credentialing 2026 — The Complete Step-by-Step Guide Every Practice Needs
Here is a scenario that plays out in medical practices across the country every single week.
A new physician joins the practice on July 1st. They start seeing patients on day one. They deliver real care to real patients — 20, 30, 40 visits a week. And then, three months later, the billing team discovers that the physician was not yet credentialed with three of the practice’s major payers when those visits happened.
The claims cannot be submitted retroactively. Or they can be submitted — but without the credentialing on file, the payer denies every single one. Hundreds of visits. Tens of thousands of dollars in services already delivered. Revenue that can never be recovered.
This is not a rare edge case. Provider credentialing and insurance enrollment are the foundation of medical billing — yet they are consistently underestimated by practices that discover their revenue impact only after a new physician has already seen 200 patients without being able to bill for a single one.
A provider who sees patients before credentialing is complete cannot legally collect reimbursement from most payers for those visits. That is not a technicality — it is real money your practice will never recover.
In 2026, the physician credentialing process has also gotten more complex. New NCQA standards, updated CMS enrollment requirements, continuous payer monitoring programs, and expanded telehealth credentialing requirements have all added layers to a process that was already demanding.
This guide covers everything — what credentialing is, how it differs from enrollment, every step in the 2026 process, the real timelines by payer type, what changed in 2026 that affects your practice right now, and how to prevent credentialing gaps from costing you revenue you have already earned.
What Is Physician Credentialing — And Why Does It Matter?
Credentialing is like a background check combined with a job application — except the employer is every insurance company you want to work with, and each one has its own forms, its own process, and its own timeline.
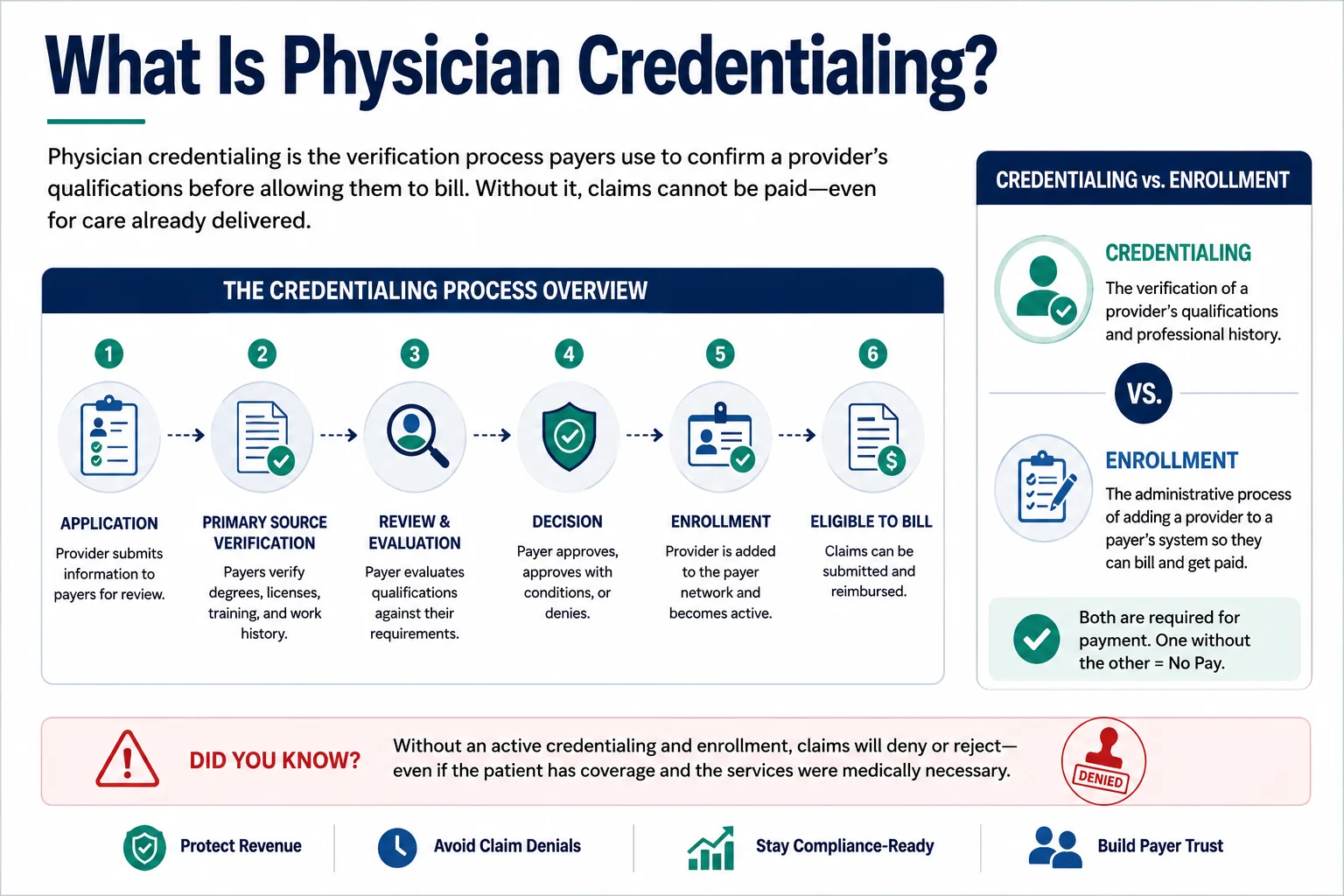
More formally: physician credentialing is the process by which payers — Medicare, Medicaid, and commercial insurance carriers — verify that a healthcare provider has the education, training, licenses, certifications, and professional history required to deliver care and receive reimbursement from that payer.
Credentialing is not the same as payer enrollment — though the two terms are often used interchangeably. Here is the actual distinction:
Credentialing is the verification of a provider’s qualifications. It confirms that the physician is who they say they are, that their license is valid, that their malpractice history is acceptable, and that they meet the payer’s standards for participation.
Payer enrollment is the contractual step that follows credentialing — joining the payer’s network, agreeing to fee schedules, and establishing the billing relationship that allows claims to be submitted and paid.
Privileging is the hospital or facility-level authorization for a provider to perform specific procedures — separate from payer credentialing but sometimes run in parallel.
All three must happen before the first clean claim goes out. Each step in the credentialing process depends on the one before it being done correctly.
The financial consequence of getting this wrong is not a delayed payment. It is a permanent revenue loss for services already rendered — because retroactive credentialing is not possible with most payers, and retroactive billing windows are narrow enough that a 90-day credentialing delay often means the claims can never be filed.
What Changed in Physician Credentialing in 2026
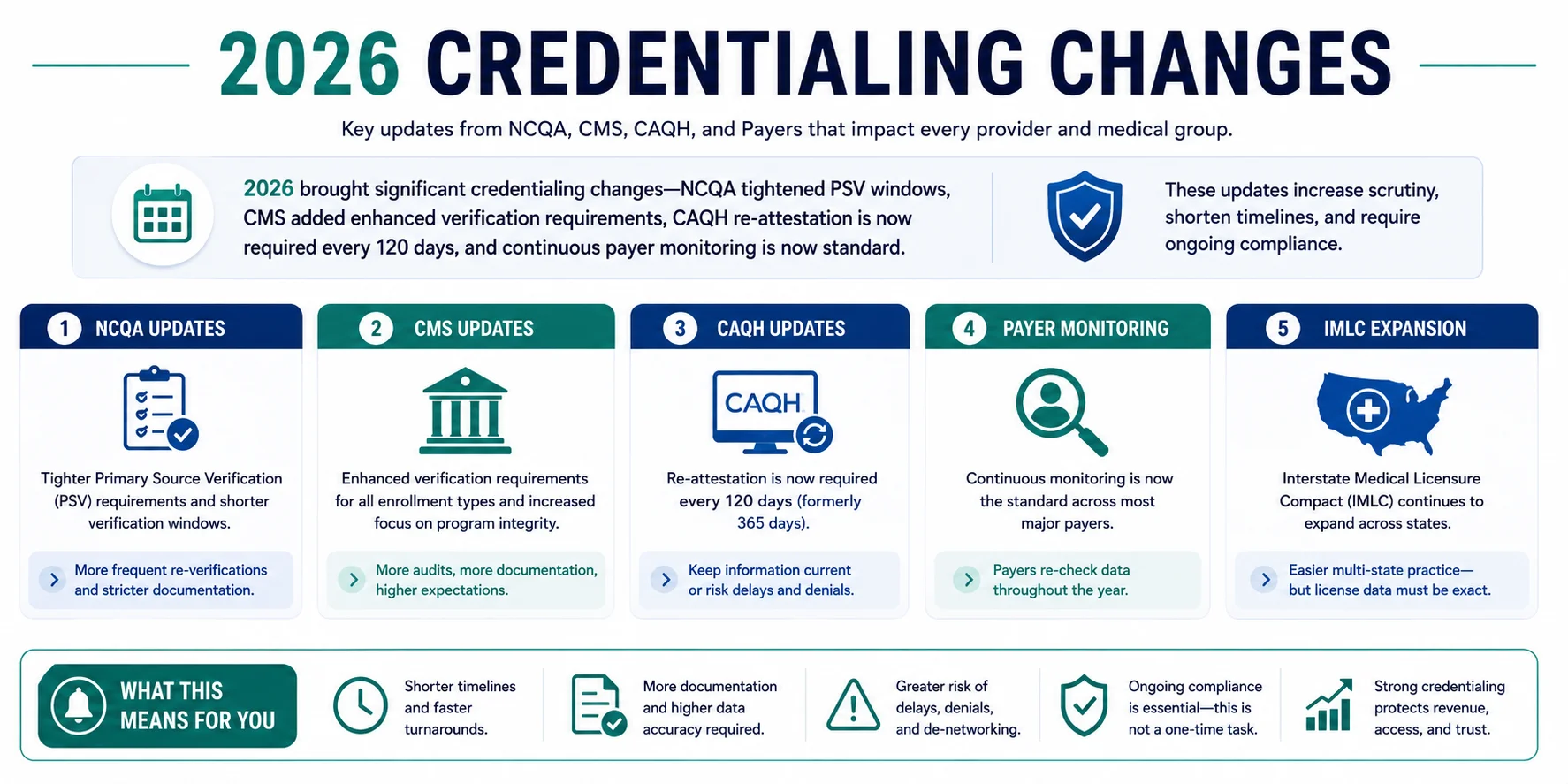
This is not a year to rely on last year’s credentialing knowledge. Provider credentialing in 2026 involves several changes that affect enrollment timelines, documentation requirements, and ongoing compliance obligations. Here is what specifically changed and what your practice needs to know:
NCQA Tightened Credentialing Windows
The NCQA rolled out its updated 2025 Credentialing Product Suite, representing the most significant shift in provider verification requirements in years. NCQA reduced credentialing windows from 180 to 120 days. This means payers aligned with NCQA standards — which includes most major commercial carriers — now have shorter internal windows for processing initial credentialing applications. For practices, this cuts both ways: it should speed up approvals for complete applications, but it also means incomplete or inaccurate applications get rejected faster rather than held for correction.
CMS Added Enhanced Primary Source Verification for Medicare and Medicaid
CMS updated its enrollment standards effective January 2026, adding enhanced primary source verification requirements for Medicare and Medicaid participation. PSV now requires direct verification of licenses, DEA registrations, board certifications, and sanctions with the issuing authorities — not just self-reported data from the provider. What was previously verified every few years may now be reviewed annually or even continuously. CAQH ProView remains the backbone of provider credentialing data. In 2026, CAQH requires additional data fields and more frequent attestations. Providers must regularly confirm profile accuracy, not just quarterly. Failure to update CAQH profiles can stall payer enrollments.
CAQH Re-Attestation Is Now Required Every 120 Days
The provider’s CAQH profile must be complete, fully attested, and authorized before any application is submitted. In 2026, re-attestation is required every 120 days. Previously, providers could go up to 180 days between CAQH attestations. The shorter window means providers and their credentialing teams need a systematic calendar to prevent CAQH profiles from expiring mid-enrollment — which automatically stalls every payer application that depends on that profile.
Continuous Payer Monitoring Is Now Standard
Several major commercial payers have implemented continuous monitoring programs that check provider license status, sanctions, and exclusion lists on a rolling basis rather than only at initial credentialing and scheduled revalidation. This is a significant operational shift. Previously, a credentialing issue discovered between revalidation cycles might go undetected for months. Now, payers are checking continuously — and a lapsed license or new sanction can trigger automatic suspension of billing privileges without advance notice.
IMLC Expanded to 40 States — Telehealth Credentialing Changed
The Interstate Medical Licensure Compact (IMLC) has expanded to 40 participating states in 2026, providing an accelerated, legally compliant pathway for physicians to secure multiple licenses — drastically speeding up the commercial process of getting credentialed with insurance companies across state lines.
For telehealth practices specifically, the 2026 location rule is now strictly enforced: payers now strictly audit the exact physical location of the patient at the time of the virtual visit. It is no longer enough for the provider to be licensed in their home state — if a physician or therapist treats a patient located across state lines, that provider must hold an active, valid license and completed provider enrollment within that specific encounter state.
Fast-Track Options Now Available With Some Payers
Several payers introduced fast-track options in 2026 for practices in underserved areas or for in-demand specialties. UnitedHealthcare offers 45-day processing for primary care providers in counties with physician shortages. Knowing which payers offer expedited enrollment — and which applications qualify — is part of managing credentialing timelines strategically.
The Complete Physician Credentialing Process — Step by Step
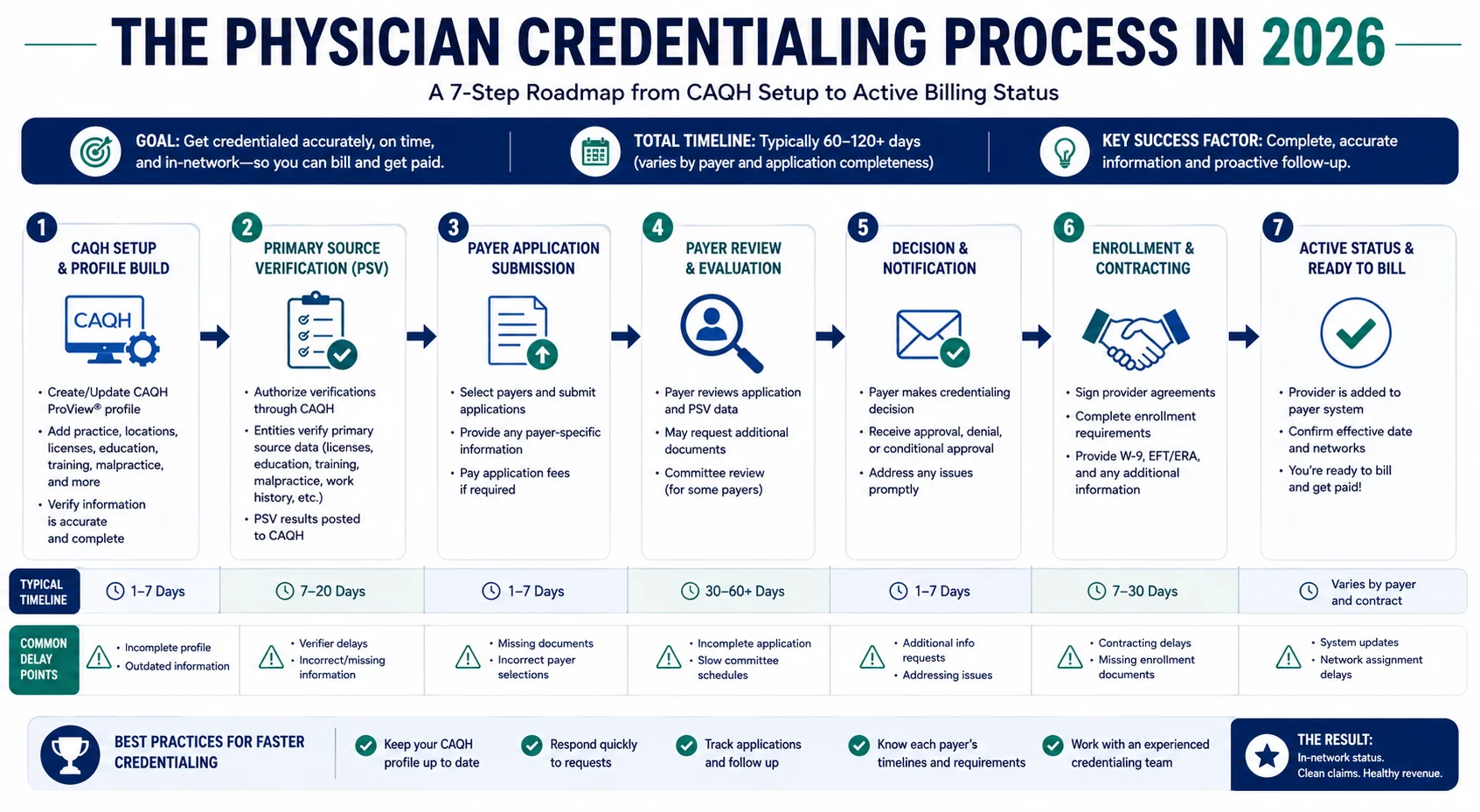
Here is the complete physician credentialing process as it works in 2026 — step by step, with the real timelines and the points where most practices lose time.
Step 1 — Establish or Update the CAQH ProView Profile
Every credentialing process in 2026 starts here. The CAQH ProView database is the universal provider data repository used by most major commercial payers and many state Medicaid programs to verify provider credentials.
A complete CAQH profile includes the provider’s education and training history, work history (typically 10 years), current malpractice insurance information, DEA registration, state license(s), board certifications, hospital affiliations, and references.
The provider’s CAQH profile must be complete, fully attested, and authorized before any application is submitted. In 2026, re-attestation is required every 120 days.
Common delays at this step: Missing or expired documents in the CAQH profile. Providers who have not attested their profile — even if it is complete — cannot have it accessed by payers. A profile flagged as incomplete will stall every downstream application simultaneously.
Timeline: Setting up a new CAQH profile from scratch: 3 to 7 business days with all documents ready. Updating an existing profile: 1 to 2 business days.
What to do right now: If your CAQH profile has not been attested within the past 90 days, attest it today. Outdated CAQH profiles remain one of the most common credentialing problems in 2026 — incorrect provider data, outdated addresses, or missing attestations can immediately stall the enrollment process.
Step 2 — Gather the Complete Documentation Package
Before submitting to any payer, compile the complete credentialing document package. Every application that goes out will draw from this same set of documents — having them complete upfront prevents the document request cycle that adds weeks to individual payer timelines.
The standard 2026 credentialing documentation package includes:
- Current, unexpired state medical license(s) — in every state where the provider will see patients
- DEA registration (if applicable)
- NPI number(s) — both individual Type 1 and group Type 2
- Board certification certificates
- Medical school diploma and transcripts
- Residency and fellowship completion documentation
- 10-year work history with no unexplained gaps
- Current professional liability / malpractice insurance certificate with tail coverage documentation
- Hospital affiliations
- CV / curriculum vitae
- CAQH ProView authorization number
For a physician starting with a group practice on June 1, enrollment applications should be submitted no later than March 1 — or February 1 for Medicaid, which has the longest processing times.
Common delays at this step: Gaps in work history, expired licenses submitted as current, missing tail coverage documentation, or board certification that expired and was not renewed before the application.
Step 3 — Medicare Enrollment Through PECOS
If your practice accepts Medicare — and most practices do — the provider must enroll through PECOS (Provider Enrollment, Chain, and Ownership System), which is CMS’s official online enrollment portal. Electronic submissions process significantly faster than paper. There is almost never a reason to submit a paper Medicare application in 2026.
PECOS enrollment requires:
- Internet-based PECOS account for the provider
- Completed CMS-855 form (individual provider) or CMS-855B (group/organization)
- NPI verification
- Social Security Number or Employer Identification Number
- Current state license information
- Malpractice coverage documentation
CMS updated its enrollment standards effective January 2026, adding enhanced primary source verification requirements for Medicare participation. CMS now directly verifies licenses and exclusion status during the enrollment review — meaning any discrepancy between submitted documentation and primary source records will pause the application.
Timeline: Medicare PECOS enrollment typically takes 30 to 90 days for a complete application. Applications with missing or inconsistent information take significantly longer.
Critical detail: Medicare does not allow retroactive billing beyond the effective date of enrollment. If a provider begins seeing Medicare patients before PECOS enrollment is complete, those claims cannot be submitted retroactively once enrollment is approved.
Step 4 — Medicaid Enrollment
Medicaid credentialing is handled state by state, and the timelines are the most unpredictable of any payer category. Federal rules require states to process applications within 45 to 90 days, but many states consistently miss this standard.
Each state Medicaid program — or Medicaid managed care organization — has its own application portal, its own document requirements, and its own processing timeline. Practices that bill multiple state Medicaid programs must manage these separately.
In states with Medicaid managed care structures — like Georgia (GAMMIS), California (Medi-Cal managed care), and Florida (Medicaid MCOs) — enrollment must often be completed both at the state level and separately with each individual managed care organization. Missing one of these layers creates “silent denials” where claims process but reimbursement goes to the wrong entity or does not come at all.
Timeline: State Medicaid enrollment: 45 to 120 days depending on the state. Medicaid MCO enrollment (in managed care states): additional 30 to 60 days per MCO after state-level enrollment.
What to do: Submit Medicaid applications at the same time as Medicare — not after. Waiting for Medicare to complete before starting Medicaid adds months to the total credentialing timeline.
Step 5 — Commercial Payer Credentialing and Enrollment
Commercial payers — Blue Cross Blue Shield, Aetna, UnitedHealthcare, Cigna, Humana, and regional carriers — each have their own credentialing application portals, their own document checklists, and their own internal review timelines.
Several major commercial payers have implemented continuous monitoring programs that check provider license status, sanctions, and exclusion lists on a rolling basis. This means that even after credentialing is complete, ongoing compliance is essential — a lapsed license or new sanction discovered through continuous monitoring can trigger immediate suspension of billing privileges.
For new providers joining a group practice, the application must also include the group’s Tax ID, the group NPI (Type 2), and documentation of the provider’s affiliation with the group. Differences in NPI details, taxonomy codes, provider names, or practice addresses across documents frequently trigger additional payer reviews and verification requests.
Timeline: Commercial payer credentialing typically takes 60 to 120 days per payer. Some payers — particularly regional BCBS plans — can run longer. UnitedHealthcare offers 45-day processing for primary care providers in counties with physician shortages in 2026 — one of several fast-track options now available if your practice qualifies.
What to do: Submit commercial payer applications simultaneously — not sequentially. Every payer you submit to on the same day is 60 to 120 days closer to complete enrollment than if you wait for one to finish before starting the next.
Step 6 — Application Follow-Up and Status Tracking
Submitted applications do not process themselves. Payer credentialing departments will request additional documentation, note discrepancies, or simply lose applications — all of which require proactive follow-up.
Industry reports show that nearly 1 out of every 3 credentialing applications requires corrections or resubmission, which significantly slows down payer approvals.
Without proactive follow-up, applications sit in payer queues — sometimes for weeks — waiting for the practice to respond to a document request or clarification. Practices that check application status only when they notice a billing problem will consistently discover that their credentialing is incomplete long after the revenue loss has already occurred.
What good follow-up looks like: Every pending application tracked in a credentialing status log — with the submission date, the last contact date, the expected processing window, and any outstanding document requests. Our physician credentialing service manages this follow-up systematically for every active application, so nothing ages without attention.
Step 7 — Re-Credentialing and Ongoing Compliance
Credentialing is not a one-time event. Every payer requires periodic re-credentialing — and the 2026 changes have made ongoing compliance more demanding than it has ever been.
Providers are no longer reviewed only every two or three years. Licenses, sanctions, and exclusions are monitored on an ongoing basis. Even minor discrepancies can trigger delays or requests for clarification.
Standard re-credentialing cycles by payer type:
- Medicare PECOS revalidation: Every 5 years for most providers
- Medicaid revalidation: Every 3 to 5 years depending on the state
- Commercial payers: Typically every 2 to 3 years
- CAQH ProView re-attestation: Every 120 days in 2026
A lapsed re-credentialing cycle does not just delay future billing — it can result in retroactive recoupment of payments received during the lapsed period. Practices need a systematic calendar for re-credentialing deadlines across every active payer enrollment.
Physician Credentialing Timelines by Payer Type — 2026 Reality
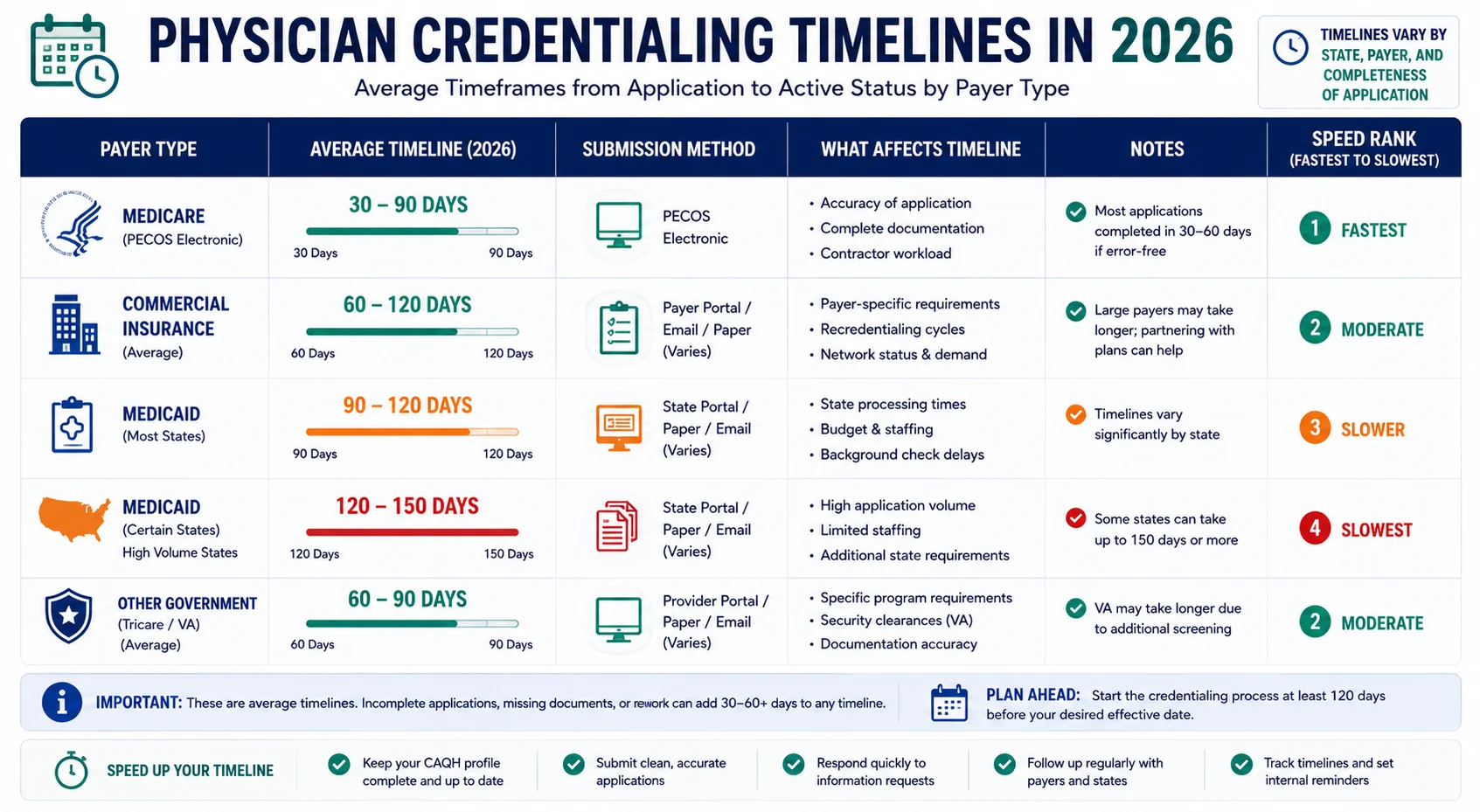
| Payer Type | Standard Timeline | With Delays | Fast-Track Available? |
|---|---|---|---|
| Medicare (PECOS electronic) | 30–90 days | 90–180 days | No (some exemptions apply) |
| Medicaid (state direct) | 45–90 days | 90–150 days | Varies by state |
| Medicaid MCOs (managed care states) | 60–120 days per MCO | Up to 150 days | Rarely |
| BCBS (major regional plans) | 60–120 days | Up to 150 days | No |
| UnitedHealthcare | 60–90 days | 90–120 days | Yes — underserved areas |
| Aetna | 60–90 days | 90–120 days | Limited |
| Cigna | 60–90 days | 90–120 days | No |
| Humana | 60–90 days | 90–120 days | Limited |
| Telehealth (multi-state) | 90–150 days | 150+ days | IMLC accelerates licensing |
The most important number in this table: When you add up simultaneous enrollment across Medicare, Medicaid, and three to five commercial payers — even on a parallel submission timeline — you are looking at a minimum of 90 days before the first payer approval comes through. Which means every new provider should start credentialing the day their start date is confirmed.
The 8 Most Common Physician Credentialing Mistakes — And How to Avoid Them
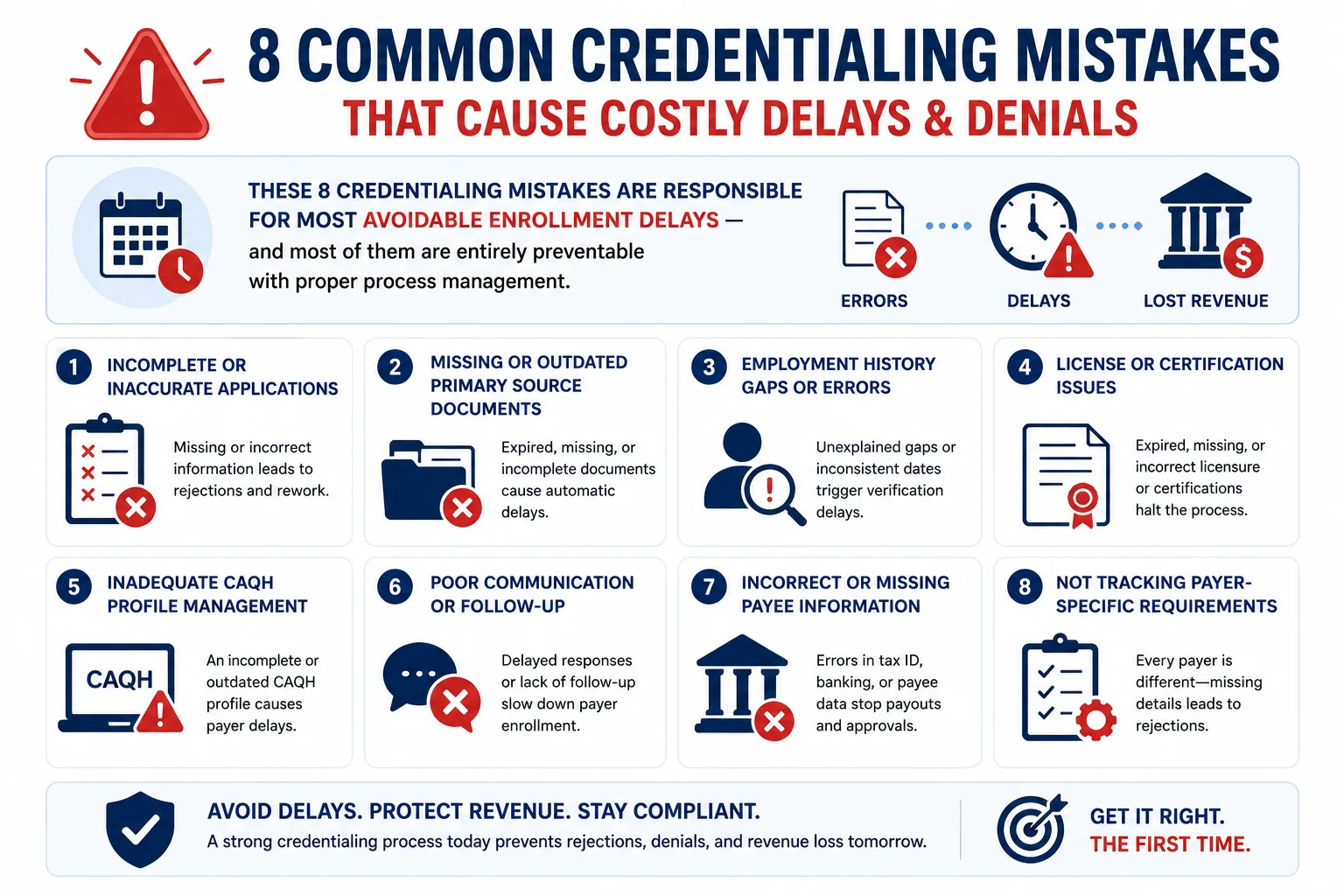
Mistake 1: Starting credentialing on the provider’s start date. The most common — and most expensive — credentialing mistake. Credentialing takes 90 to 150 days. Starting on day one means the provider sees patients for three to five months before billing is possible. For a physician starting with a group practice on June 1, applications should be submitted no later than March 1 — or February 1 for Medicaid.
Mistake 2: Letting the CAQH profile expire before submitting applications. CAQH profiles that have not been attested within 120 days are flagged as incomplete — and payers cannot access an incomplete profile. This stalls every pending application simultaneously. Check CAQH attestation status before every application submission.
Mistake 3: Submitting payer applications sequentially instead of simultaneously. Waiting for Medicare to approve before starting commercial applications adds months to the total timeline. All applications should be submitted at the same time.
Mistake 4: Not tracking application status proactively. Nearly 1 in 3 credentialing applications requires corrections or resubmission. Payers will request additional documentation and then wait — indefinitely — for a response. Applications with no follow-up sit in pending status for months until someone notices.
Mistake 5: Missing NPI or taxonomy code discrepancies across documents. Differences in NPI details, taxonomy codes, provider names, or practice addresses across documents frequently trigger additional payer reviews and verification requests. Every document in the application package must be consistent.
Mistake 6: Not understanding the retroactive billing window. Even payers that allow retroactive billing have strict time limits. If credentialing is not complete within 90 to 180 days of the provider’s start date, the retroactive window may close — and services already rendered become permanently unbillable.
Mistake 7: Treating re-credentialing as optional or low priority. Missed re-credentialing deadlines can result in suspension of billing privileges and retroactive recoupment of payments already received. With continuous payer monitoring now standard in 2026, compliance gaps are being caught faster than ever.
Mistake 8: Separating credentialing from billing management. Credentialing gaps directly create billing voids — but when credentialing and billing are managed by separate vendors, neither one knows what the other is doing. The coordination failure creates enrollment gaps that generate weeks of unbillable claims before anyone identifies the problem. Managing both through one company — like Pro Health Care Advisors — eliminates this coordination risk entirely.
Telehealth Credentialing in 2026 — What Changed and What It Costs Practices
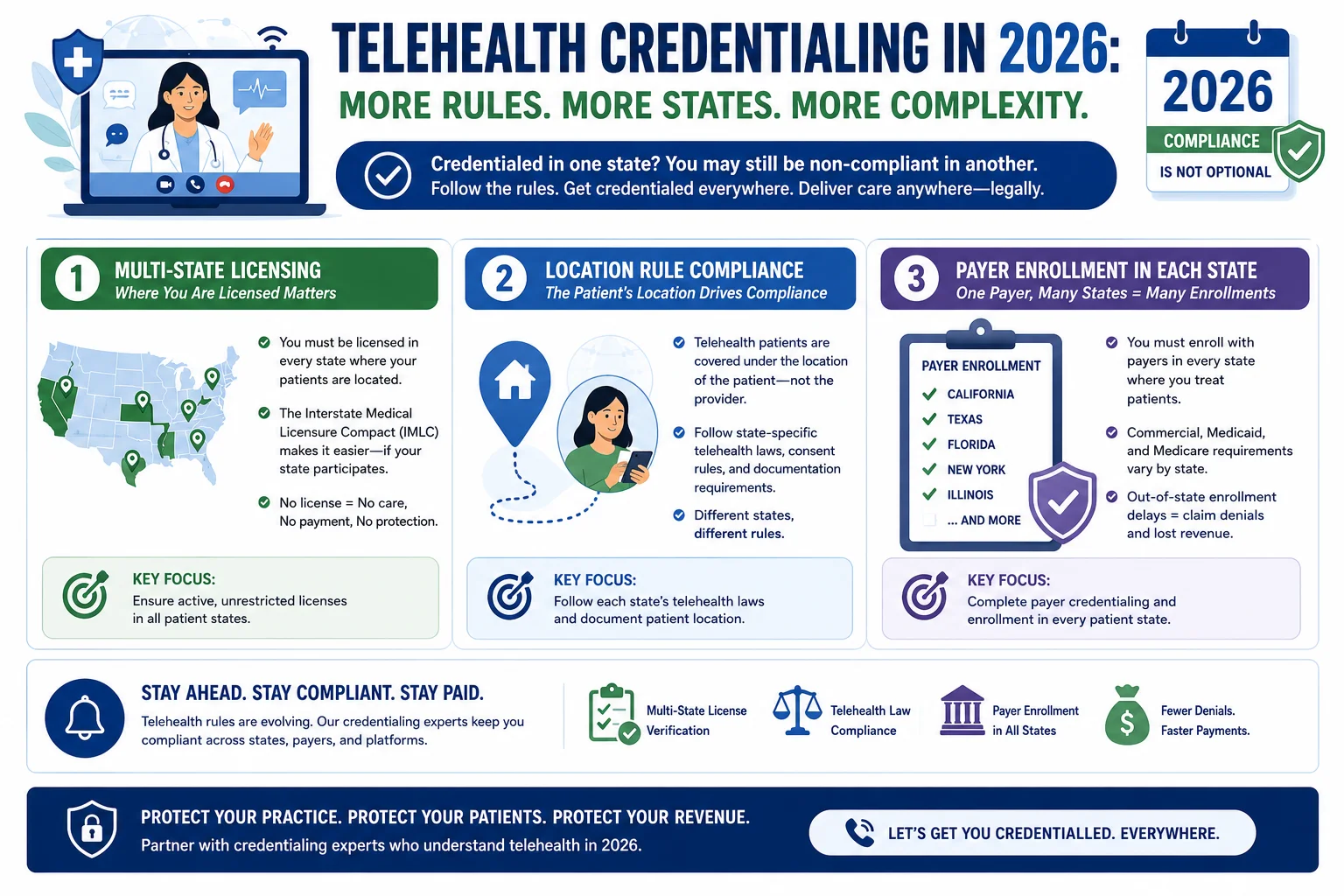
Telehealth credentialing is consistently the most underestimated credentialing challenge in 2026. Telehealth credentialing often takes longer because providers may require multi-state licenses and separate payer enrollments for multiple states. In 2026, telehealth credentialing timelines usually range between 90 and 150 days.
The key 2026 rule change that many practices have not fully implemented: payers now strictly audit the exact physical location of the patient at the time of the virtual visit. If a physician or therapist treats a patient located across state lines, that provider must hold an active, valid license and completed provider enrollment within that specific encounter state.
This means a psychiatrist licensed in Georgia who provides telehealth to a patient currently located in Florida needs an active Florida license and Florida payer enrollment — not just a Georgia license. The IMLC expansion to 40 states helps with the licensing portion, but payer enrollment must still be completed state by state.
Practices with telehealth volume need to audit their providers’ multi-state enrollment status against the states where their telehealth patients are actually located — not just where they are officially registered.
How Pro Health Care Advisors Manages Physician Credentialing

Physician credentialing is one of the services where the gap between doing it right and doing it casually is measured in tens of thousands of dollars. Our physician credentialing service is built around the process discipline that prevents the mistakes most practices make.
Here is specifically what we manage for every credentialing client:
CAQH ProView Setup and Maintenance — Complete CAQH profile setup for new providers, with 120-day attestation tracking to ensure profiles never expire mid-enrollment.
Document Collection and Verification — We collect and verify the complete documentation package — licenses, DEA, malpractice, board certifications, work history — before submitting to any payer, catching discrepancies before they generate application delays.
Simultaneous Multi-Payer Submission — We submit to Medicare (PECOS), Medicaid, and commercial payers simultaneously — not sequentially — to compress the total credentialing timeline.
Active Application Follow-Up — Every pending application is tracked in our status management system. We follow up proactively with payer credentialing departments before applications stall in pending status.
Re-Credentialing Calendar Management — We track every active enrollment’s re-credentialing deadline and initiate re-credentialing 90 days before expiration — so billing privileges are never interrupted by a missed renewal.
Telehealth Multi-State Enrollment — For providers delivering telehealth across state lines, we manage multi-state licensing coordination and state-specific payer enrollment to keep pace with the 2026 location rule requirements.
Billing Coordination — Because we manage both credentialing and medical billing for our clients, we can coordinate enrollment status directly with our billing team — eliminating the coordination failure that creates unbillable claim periods when credentialing and billing are handled separately.
For more on how credentialing fits into the broader revenue cycle, read our complete guide to revenue cycle management.
Frequently Asked Questions — Physician Credentialing 2026
Q: How long does physician credentialing take in 2026? It depends on the payer type. Medicare PECOS enrollment typically takes 30 to 90 days for a complete application. Commercial payers run 60 to 120 days. Medicaid varies by state — 45 to 150 days. When enrolling with multiple payers simultaneously, the total credentialing process typically takes 90 to 150 days from complete application submission to the first approved enrollment. Telehealth credentialing across multiple states adds additional time.
Q: What is CAQH ProView and why does it matter for credentialing? CAQH ProView is the universal provider data repository used by most major commercial payers and state Medicaid programs to access and verify provider credentials. A complete, attested CAQH profile is required before most payer applications can be processed. In 2026, CAQH requires re-attestation every 120 days — an expired profile stalls all pending applications simultaneously.
Q: Can a provider see patients before credentialing is complete? Technically yes — but the financial consequences are severe. Claims for services rendered before credentialing is approved cannot be submitted to most payers. Some payers allow retroactive billing within a limited window (typically 90 to 180 days), but once that window closes, the revenue from those visits is permanently lost.
Q: What is the difference between credentialing and payer enrollment? Credentialing is the verification of a provider’s qualifications — confirming their license, education, training, and professional history. Payer enrollment is the contractual step that follows — joining the payer’s network and establishing billing privileges. Both must be complete before a provider can bill a specific payer.
Q: What changed in physician credentialing in 2026? Several significant changes took effect: NCQA reduced credentialing windows from 180 to 120 days. CMS added enhanced primary source verification for Medicare and Medicaid enrollment. CAQH re-attestation is now required every 120 days instead of every 180 days. Major commercial payers implemented continuous monitoring programs. The IMLC expanded to 40 states. And the telehealth location rule is now strictly enforced, requiring state-specific enrollment for every state where patients receive virtual care.
Q: How do I prevent credentialing delays from costing my practice revenue? Start credentialing at least 90 to 120 days before a new provider’s start date — earlier for Medicaid. Submit all payer applications simultaneously. Keep CAQH profiles attested. Track every pending application with proactive follow-up. Manage re-credentialing calendars for all active enrollments. And — most importantly — manage credentialing through the same company that handles your billing so enrollment status and billing workflows stay synchronized.
Q: Does Pro Health Care Advisors handle physician credentialing? Yes. Our physician credentialing service manages the complete enrollment process — CAQH setup, PECOS enrollment, commercial payer applications, Medicaid enrollment, application follow-up, and re-credentialing tracking. We also manage the coordination between credentialing status and billing workflows to eliminate the gaps that create unbillable claim periods. For more information, contact us for a free consultation.
For more on how physician credentialing fits into your practice’s financial operations, read our guides on revenue cycle management, medical billing trends 2026, and how to reduce claim denials. For more billing resources, visit our articles and resources library.