Medical Billing for Small Practices 2026 — The Complete Survival Guide
Running a small medical practice in 2026 means being a clinician, an administrator, a manager, and a billing department — often all at the same time.
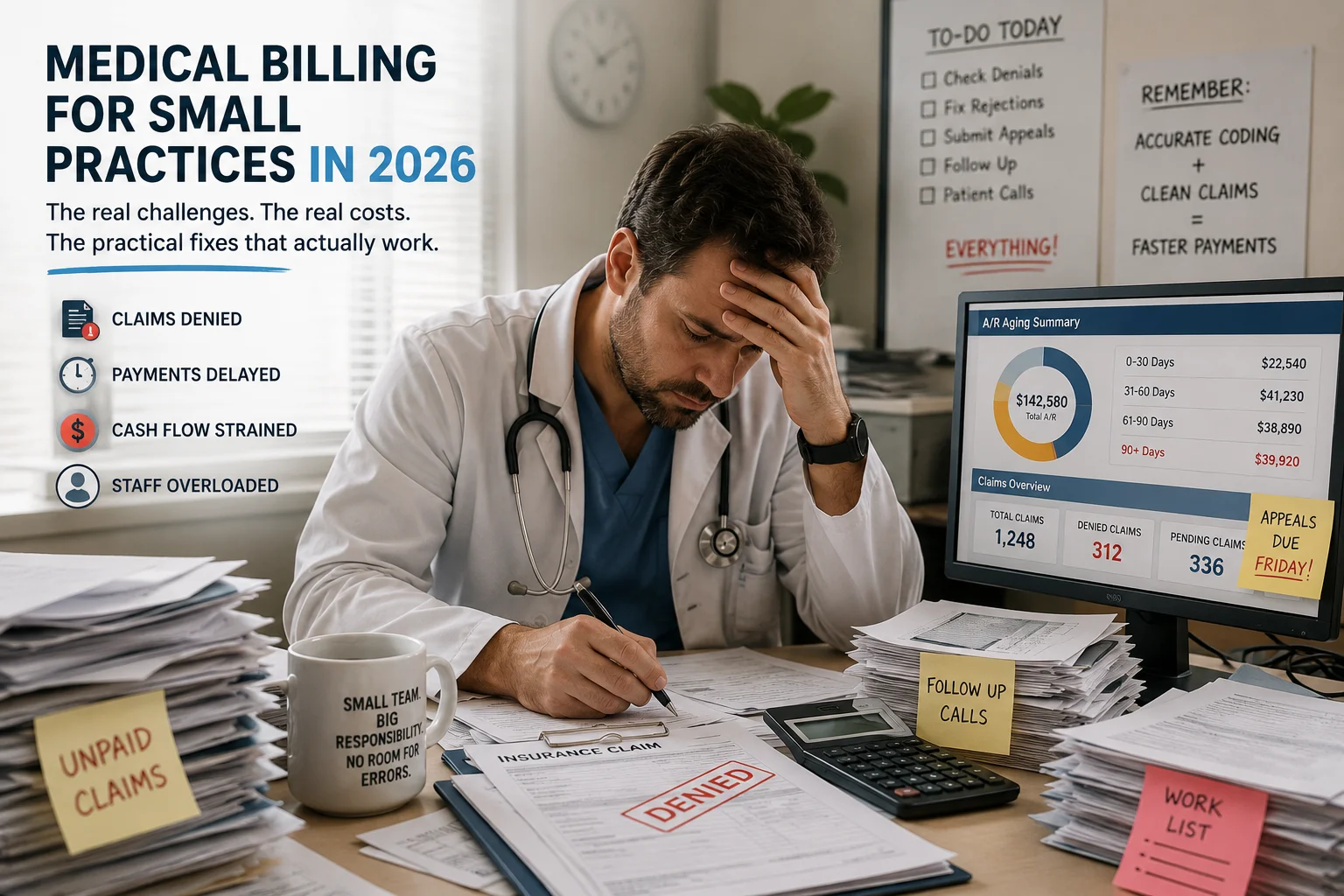
You went to medical school to take care of patients. But somewhere between charting, prior authorizations, claim submissions, denial appeals, and chasing patient balances, the clinical part can start to feel like the smallest piece of the job.
And the billing piece? Medical billing in 2026 requires precision, speed, and deep knowledge of regulations. Insurance rules are stricter. Patients are paying more out of pocket. Administrative work is increasing. All of this makes billing more complex.
Here is the number that captures the pressure most clearly: the 2026 Medicare conversion factor dropped 2.8 percent — for a typical small practice, this translates to tens of thousands of dollars in lost revenue unless volume increases or efficiency improves dramatically. That is not a hypothetical. That is money leaving your practice right now — even before a single claim gets denied.
In 2026, managing a medical practice is more challenging than ever. Costs are rising, insurance rules change often, and small practices do not have the advanced billing and coding resources that large healthcare organizations enjoy.
This guide is written specifically for small and independent practices — solo physicians, two-to-five provider groups, and specialty clinics operating without a dedicated billing department. It covers the real challenges, the real costs, and the real solutions that help small practices collect more of what they earn without burning out the people trying to make it happen.
Why Medical Billing Is Harder for Small Practices Than for Large Systems
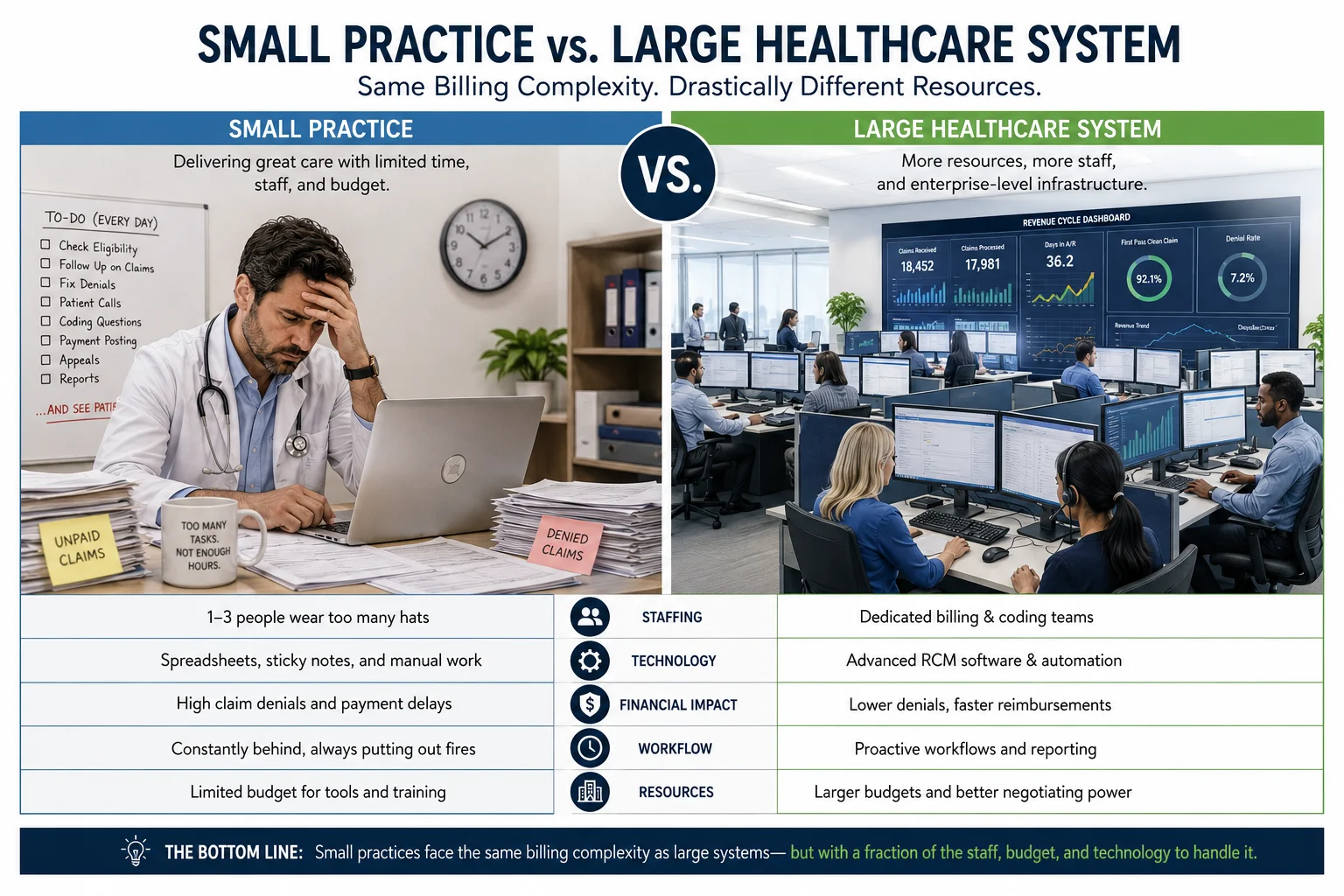
The rules are the same. The payers are the same. The prior authorization requirements are the same. The CPT code changes, the denial codes, the HIPAA regulations, the credentialing timelines — all the same.
The difference is the resources available to navigate them.
A large hospital system has a dedicated billing department with specialized coders, a prior authorization team, a denial management unit, a credentialing coordinator, and compliance officers. Small practices do not have these resources — making it genuinely difficult to navigate the billing complexity that large organizations handle with dedicated staff.
People on lean teams in small practices have to wear many hats. The people who take care of patients often have to bill, code, and check in with insurance companies. When there are not enough dedicated billing experts, mistakes, delays, and missed tasks happen more often — and that directly hurts cash flow and reimbursement rates.
In 2026, lean teams cannot afford gaps across intake, eligibility, scheduling, claims, and collections. 37 percent of software buyers cite missed business opportunities as one of the most frequent billing pain points, followed by limited functionality and workflow efficiency.
The result is a predictable pattern: small practices consistently collect less per claim than large systems — not because they deliver worse care, but because the billing infrastructure is thinner, more vulnerable to disruption, and less equipped to navigate the 2026 payer environment.
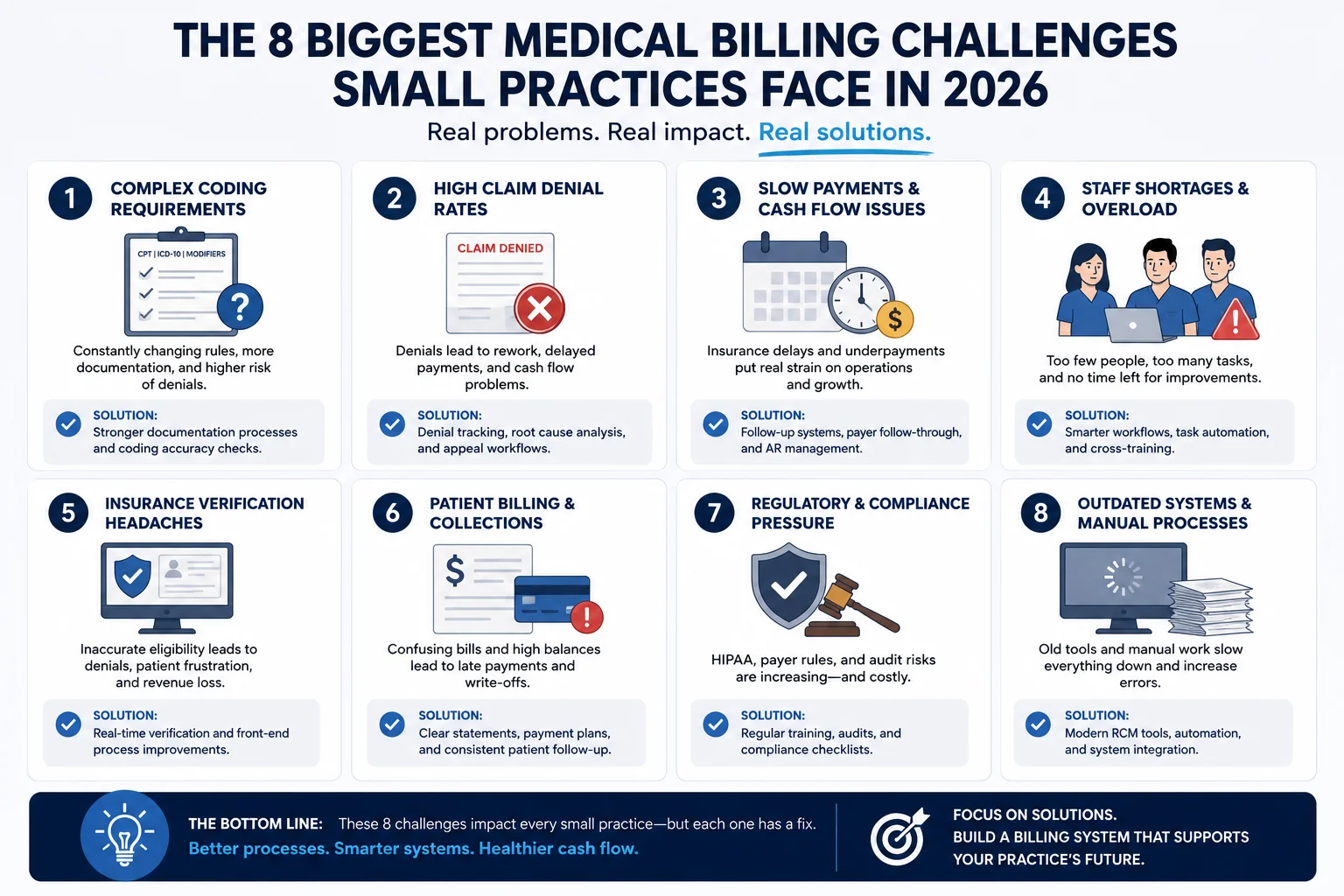
The 8 Biggest Medical Billing Challenges for Small Practices in 2026
Challenge 1 — The Medicare Conversion Factor Cut Is Shrinking Your Revenue
The 2026 Medicare Physician Fee Schedule continues the downward pressure on practice revenue. The conversion factor dropped 2.8 percent, moving from $33.29 in 2024 to $32.35 in 2025. While this may look small on paper, for a typical small practice it translates to tens of thousands of dollars in lost revenue unless volume increases or efficiency improves dramatically.
For a small practice collecting $800,000 annually in Medicare revenue, a 2.8 percent cut is $22,400 in annual revenue reduction — without a single billing mistake. The only way to offset a reimbursement rate cut is to collect more of what you are already owed on every other claim — which means tightening clean claim rates, reducing denials, and closing undercoding gaps.
To maintain margins, leaders must capture every legitimate dollar on the first submission. Every missed code or delayed claim now hurts more than ever.
What to do: Conduct a coding audit to identify undercoding patterns. Review your clean claim rate. If you are not collecting above 93 percent of net allowable charges, you have a billing performance gap that is compounding the fee schedule cut.
Challenge 2 — Claim Denial Rates Are Rising and Small Practices Are Hit Hardest
60 percent of medical group leaders reported higher claim denial rates in early 2024 compared with 2023 — and that trend has continued into 2026. Insurance companies are becoming stricter with their reviews. Even minor errors can lead to rejection. Denial rates have increased steadily, forcing practices to spend extra time and resources on rework — which not only delays payments but also increases operational costs.
For a large system, a rising denial rate is a problem their billing department can absorb — they have a dedicated appeals team. For a small practice, the same rising denial rate means the same clinician who saw patients all day is now staying late to work denials — or those denials simply sit until the appeal window closes.
Claim denials in medical billing are not just paperwork — they can seriously affect your practice’s revenue. And for a small practice with thin margins, a denial rate above 10 percent can be the difference between a sustainable month and a cash flow crisis.
What to do: Identify your top five denial codes. Map them to their root causes using our complete medical billing denial codes guide. Fix the upstream process generating each pattern — not just the individual claim. For structured denial management support, see our creative collection solutions.
Challenge 3 — Prior Authorization Is Consuming Clinical and Administrative Time
Prior authorization requirements have expanded dramatically — and for a small practice with no dedicated PA coordinator, the burden falls directly on clinical and front-desk staff.
The American Medical Association reports physicians now spend 14.5 hours per week on prior authorization. In a small practice, that is time the physician or a nurse is spending on the phone with insurance carriers instead of seeing patients. From prior authorization requirements in cardiology to modifier-heavy coding in orthopedics, many practices are discovering that generalist billing knowledge is not enough anymore.
CO-15 denials — authorization missing or invalid — are one of the most common and most preventable denial types. But preventing them requires a systematic prior authorization tracking workflow that most small practice billing teams do not have the bandwidth to build and maintain.
What to do: Build a prior authorization tracking log for every service type that requires it — by payer. Check authorization status before every procedure, not after the service is delivered. For more on how prior authorization drives specific denial codes, see our denial codes guide.
Challenge 4 — Staff Turnover Creates Billing Gaps That Cost Real Money
Insurance payment delays are another ongoing concern. Many practices report longer waiting periods for reimbursements. Payments that once took a few weeks now take months. This disrupts financial planning and creates stress, especially for smaller practices.
But the staffing problem goes deeper than payment delays. Annual billing staff turnover in healthcare runs between 33 and 40 percent. For a small practice that relies on one or two billers, a single resignation creates an immediate billing crisis — claims pile up, denials go unworked, AR ages, and the revenue impact compounds every day until a replacement is hired and trained.
In 2026, lean teams cannot afford gaps across intake, eligibility, scheduling, claims, and collections. Missed follow-ups lead to lost appointments, delayed care, and weaker cash flow.
What to do: If your billing operation depends on one or two people, your revenue is a single resignation away from a crisis. This is one of the strongest arguments for outsourcing billing to a company where your claims are never dependent on one person showing up. Read our in-house vs outsourced medical billing guide for the full comparison.
Challenge 5 — Patient Collections Are Growing — and Getting Harder
High-deductible health plans now cover more than 57 percent of employer-sponsored insured workers. That means the patient’s share of every bill is larger — and collecting it is harder.
For small practices, this creates a difficult dynamic. You know your patients personally. Asking them for money feels different in an independent practice than in a large hospital system. But the financial reality is the same: uncollected patient balances are a growing share of revenue loss, and practices that do not have structured patient collection processes are absorbing losses that are entirely preventable.
Medical billing services for small practices handle the entire revenue cycle — from insurance verification through patient collections — so that the collection conversation is managed systematically and professionally, not awkwardly and inconsistently.
What to do: Collect copays and estimated patient responsibility at time of service, every time. Offer payment plan options for larger balances. Use online payment portals that make it easy for patients to pay without calling the office. Our creative collection solutions include patient balance management workflows designed for practices that want to recover more without damaging patient relationships.
Challenge 6 — Compliance Requirements Are Getting More Complex
With 42 CFR Part 2 updates effective February 2026, substance use disorder billing now carries tighter compliance requirements around consent and record sharing. Surgical billing lives and dies by global period rules — knowing which procedures fall under a 10-day versus 90-day global period, and when to apply modifiers like -59 and -25, is the difference between getting paid and getting denied.
For small practices, keeping up with compliance changes is genuinely difficult. There is no compliance officer. No legal department. No dedicated coder who reads every CMS update. In 2026, cybersecurity threats are also targeting healthcare practices specifically — and a data breach does not just threaten patient privacy, it can halt billing operations entirely while the practice recovers.
The HHS Office of Inspector General consistently identifies upcoding, improper place-of-service billing, and inadequate medical necessity documentation as the top compliance vulnerabilities — all billing process failures with real financial consequences.
What to do: Build compliance into your billing process — not as a separate audit exercise, but as part of every claim review. Our HIPAA compliance services and MD Audit Shield RAC service provide the compliance monitoring that small practices cannot build in-house at sustainable cost.
Challenge 7 — Telehealth Billing Errors Are a Growing Problem
Telehealth volume remains high for many small practices — but telehealth billing errors are also high. With frequent regulatory updates and payer variability, even small billing errors in telehealth claims can lead to denials or delayed payments. Practices that fail to adapt risk losing revenue from one of the fastest-growing care models.
The 2026 telehealth location rule strictly enforces patient-location-based licensing and enrollment. A provider who delivers telehealth to a patient located in a different state must be licensed and enrolled with payers in that state — and most small practices have not audited whether their telehealth billing is compliant with this rule.
What to do: Audit your telehealth claims from the past six months. Verify that every telehealth claim correctly identifies the patient’s location and that your provider is enrolled with payers in every state where telehealth patients were located. For credentialing guidance, see our physician credentialing guide.
Challenge 8 — Undercoding Is Quietly Draining Revenue Nobody Can See
This is the challenge that generates the least urgency — because it is invisible. Denied claims show up in your AR report. Undercoded claims get paid. They just get paid for less than you were entitled to.
Research consistently identifies undercoding as costing practices 6 to 9 percent of net collections. For a small practice collecting $100,000 per month, that is $6,000 to $9,000 in monthly revenue loss that never appears on any report as a problem — because the claim was paid.
Common causes in small practices: providers documenting a level 3 visit when the clinical work and time support a level 4 or 5. Procedures delivered but entered at a lower complexity than performed. Modifiers missed that would unbundle a separately billable service.
What to do: Conduct a coding audit comparing your documented encounter complexity against the CPT levels you are billing. Our CodeMAXX services specifically target the undercoding patterns that suppress net collections without generating visible denials.
What Small Practices Are Actually Spending on Billing — The Real Numbers
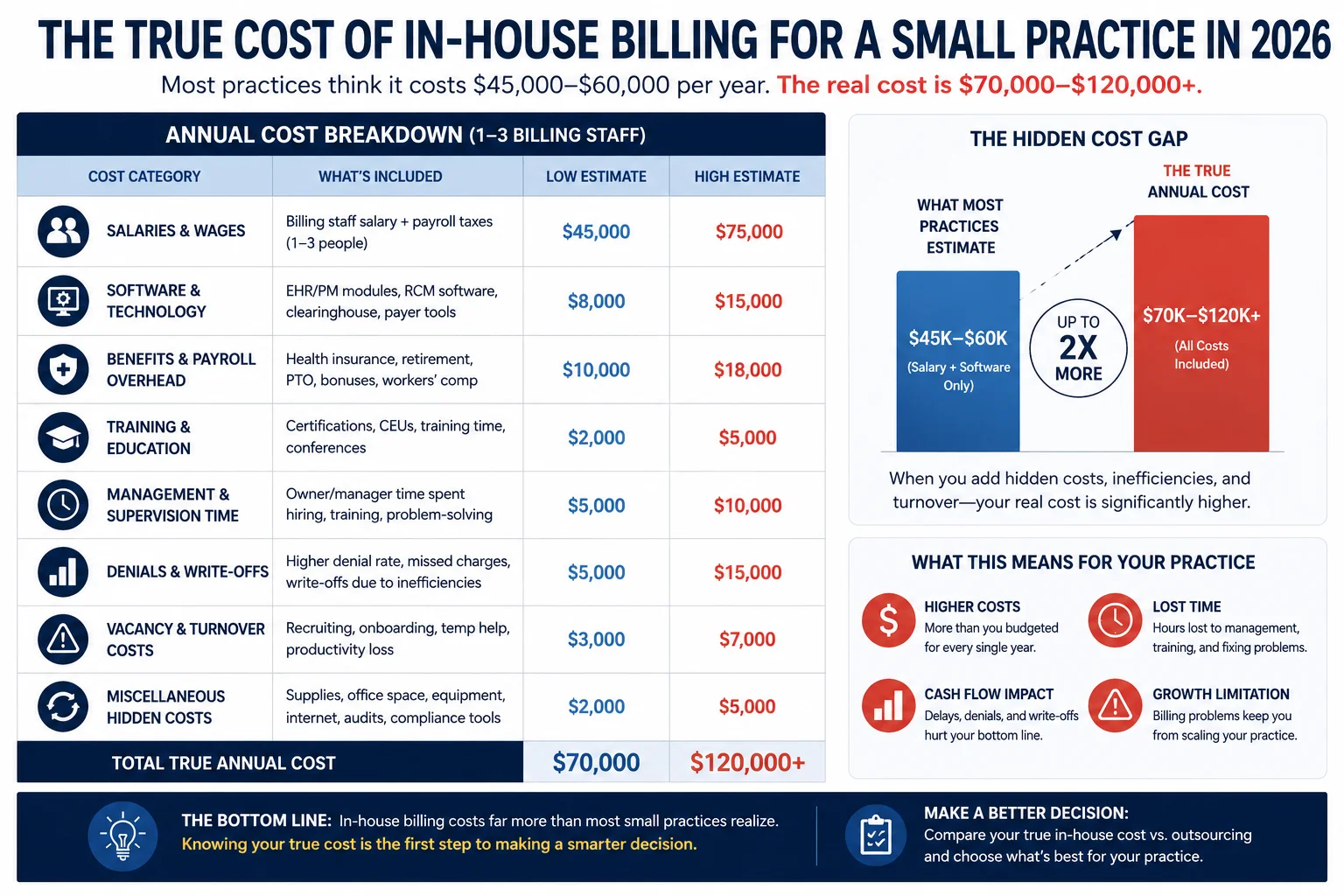
Most small practices dramatically underestimate what their billing actually costs. Here is what the real numbers look like for a small practice with one to two billers:
| Cost Component | Estimated Annual Cost |
|---|---|
| Biller salary (1 FTE) | $42,000 – $58,000 |
| Benefits + payroll taxes (28–35%) | $12,000 – $20,000 |
| Billing software + clearinghouse | $4,800 – $22,800 |
| Training + certification | $500 – $1,500 |
| Turnover + replacement (annualized) | $1,500 – $5,000 |
| Denied claim write-offs (3–5% of revenue) | $3,600 – $9,000/month |
| Undercoding losses (6–9% of net collections) | $6,000 – $13,500/month |
| Physician oversight time (opportunity cost) | $10,000 – $30,000 |
| True annual billing cost | $70,000 – $120,000+ |
Compare that to outsourced billing at 5 to 7 percent of net collections — typically $5,000 to $14,000 per month for a practice collecting $100,000 to $200,000 monthly — with a higher clean claim rate, lower denial rate, and no turnover risk.
For most small practices, the outsourced model produces more net revenue at lower total cost. For the full analysis, read our in-house vs outsourced medical billing comparison.
The 5 Things Small Practices Should Do Right Now to Improve Billing
You do not need to fix everything at once. Here are the five actions with the highest immediate impact for small practice billing in 2026:
Action 1: Run real-time eligibility verification before every appointment. Not at registration. Not from the patient’s last visit. Before every appointment. Insurance changes constantly — and every claim submitted to the wrong payer or for a non-covered service generates an avoidable denial. Real-time eligibility is the single highest-ROI change most small practices can make.
Action 2: Pull your top 10 denial codes and identify their root causes. If you do not know which denial codes appear most frequently on your EOBs, you cannot fix the upstream problems generating them. Pull your denial report, identify the top 10 codes, and match each one to its root cause using our medical billing denial codes guide. Fix the process, not just the claim.
Action 3: Conduct a coding audit on your top 5 most-billed CPT codes. Compare the complexity level you are billing against the documentation in the clinical record for 20 to 30 recent encounters. If you find systematic undercoding — and most small practices do — the revenue recovery from correcting it forward pays for itself immediately.
Action 4: Start collecting patient responsibility at time of service. Copays, estimated deductibles, and known patient balances collected before the patient leaves are dramatically easier to collect than bills sent weeks later. Build a point-of-service collection step into your check-in or check-out workflow.
Action 5: Audit your CPT code tables against 2026 deletions. The 2026 CPT update deleted 84 codes. Any claim submitted with a deleted code generates an automatic rejection. Pull your most-used codes from 2025 and verify none were deleted. For the full breakdown, see our CPT code changes 2026 guide.
When to Consider Outsourcing Billing for Your Small Practice
Not every small practice should outsource billing. But there are clear signals that the outsourced model will outperform in-house billing for a specific practice.
Your denial rate is above 8 percent. If more than 8 out of every 100 claims comes back denied, your billing process has structural problems compounding the Medicare fee cut. An outsourced billing partner with a sub-2 percent denial rate recovers that revenue immediately.
Your net collection rate is below 90 percent. If you are collecting less than 90 cents for every dollar legitimately owed, you have a billing performance gap. Top-performing outsourced billing companies collect 93 to 97 percent.
Your biller just left — or is about to. If your billing operation depends on one person and that person is unavailable, your revenue stops. Outsourcing eliminates this single point of failure.
You are spending clinical time on billing oversight. If you as the physician are reviewing billing reports or fixing billing errors — that time has a real cost that is not showing up on any report.
You have new providers joining who need credentialing. Managing billing and credentialing through two separate vendors creates coordination failures that generate unbillable claim periods. Our physician credentialing service and billing services work together to prevent credentialing gaps from becoming revenue gaps.
You do not know your clean claim rate. If you cannot answer this question immediately — your billing visibility is insufficient, and problems are likely already happening that nobody has identified yet.
How Pro Health Care Advisors Serves Small and Independent Practices

Pro Health Care Advisors was built to give small and independent practices access to the billing expertise, technology, and workflow infrastructure that large hospital systems take for granted.
98.5% Clean Claim Rate. Our AAPC-certified team submits at 98.5 percent — the difference from the 85 to 90 percent in-house average shows up in faster payments and lower denial volume from month one.
Under 2% Denial Rate. Compared to the national average of 11 to 13 percent — our sub-2 percent denial rate means your clinical work gets paid consistently on first submission.
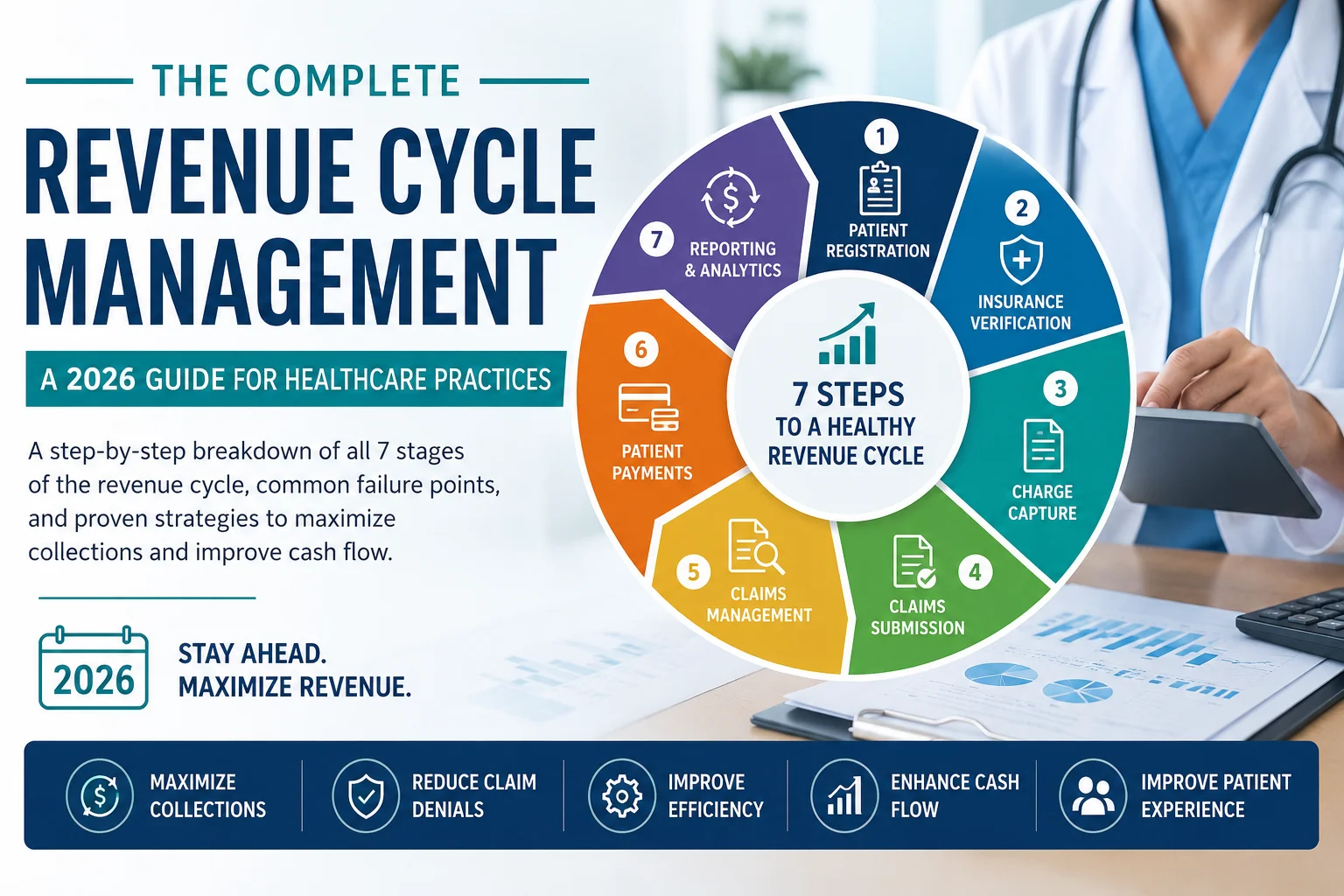
Full Revenue Cycle Management. Every step managed through our medical billing and practice management services. For what the full revenue cycle includes, see our complete RCM guide.
AAPC-Certified Coding. Our coders catch undercoding patterns that in-house teams consistently miss — recovering the 6 to 9 percent of net collections most small practices leave on the table. See our CodeMAXX services.
Physician Credentialing. New provider? We handle the entire enrollment process — CAQH, PECOS, Medicaid, commercial payers — with proactive follow-up. See our physician credentialing service.
Audit Protection. Our MD Audit Shield RAC service provides the compliance monitoring and audit response support small practices cannot build in-house.
HIPAA Compliance. Our HIPAA compliance services include signed BAA management, security protocols, and breach response planning.
30+ Specialties Served. Cardiology, family practice, mental health, wound care, and more. See our full specialties list.
Percentage-Based Pricing. We charge a percentage of net collections — we only make more money when you collect more money. No flat fees. No contracts that reward submission volume over collection performance.
Frequently Asked Questions — Medical Billing for Small Practices 2026
Q: What is the biggest billing challenge for small practices in 2026? The combination of the 2.8 percent Medicare conversion factor cut and rising claim denial rates — now affecting 60 percent of medical group leaders — is the most damaging double challenge. Each reduces collections individually. Together they compress margins significantly for practices without tight billing operations.
Q: How much does medical billing cost for a small practice? When you count all true costs — salary, benefits, software, training, turnover, and uncollected denied claims — in-house billing for a small practice typically runs $70,000 to $120,000 per year. Outsourced billing at 5 to 7 percent of net collections typically costs less while producing higher net collection rates.
Q: Should a small practice outsource medical billing? For most small practices — particularly those with denial rates above 8 percent, net collection rates below 90 percent, or billing staff turnover risk — yes. Read our full comparison: In-House vs Outsourced Medical Billing.
Q: What is a good clean claim rate for a small practice? The industry benchmark is 95 percent. The best outsourced billing partners in 2026 operate at 98 percent or higher. If your small practice’s clean claim rate is below 92 percent, you have a billing process problem costing you money on every claim you submit.
Q: How do small practices handle prior authorization without a dedicated PA coordinator? Most small practices cannot afford a dedicated PA coordinator. The most effective solution is either a systematic tracking workflow your billing team manages, or outsourcing billing to a company that includes prior authorization tracking as part of their standard service.
Q: How does the 2026 Medicare fee schedule cut affect small practices specifically? The 2.8 percent conversion factor reduction means a practice collecting $800,000 annually in Medicare revenue loses approximately $22,400 per year — without a single billing error. The only offset is improved billing performance. For more on 2026 changes, see our medical billing trends 2026 guide.
Q: What billing metrics should a small practice track? At minimum: clean claim rate, denial rate by payer and code, net collection rate, days in AR, and patient collection rate. For what these metrics mean and what good performance looks like, see our revenue cycle management guide.
For more billing education and resources, visit our articles and resources library.
The Bottom Line — Small Practices Deserve the Same Billing Performance as Large Systems

The 2026 billing environment does not give small practices a break because they have fewer resources. The denial rates are the same. The prior authorization requirements are the same. The CPT code changes are the same. The compliance obligations are the same.
What can be different — and what should be different — is the billing operation supporting your practice.
When billing works smoothly, revenue flows in on time. When it does not, everything slows down. In 2026, billing errors have become more costly than ever.
Pro Health Care Advisors gives small practices access to the same AAPC-certified billing expertise, structured denial management, and full revenue cycle infrastructure that large health systems take for granted — at a cost that scales with your collections, not a flat fee that ignores whether your claims get paid.
Our 98.5 percent clean claim rate and sub-2 percent denial rate are not large-system benchmarks applied to small practices as a theory. They are numbers we maintain for small and independent practices across more than 30 specialties — every day, every month.
If you want to know where your practice stands right now — and what it would take to collect more of what you have already earned — the conversation starts here.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pressure. No pitch. Just a real look at your billing performance and an honest conversation about what better looks like for your specific practice.