MEDICAL BILLING DENIAL CODES 2026 — COMPLETE CO, PR, OA GUIDE WITH FIX STEPS
Your claim came back denied.
There is a code on the explanation of benefits — two letters, a dash, and a number. Maybe it says CO-16. Maybe PR-96. Maybe OA-23. And if you are not sure what it means or what to do next, that claim is probably going to sit in a queue, age past its appeal window, and eventually get written off as uncollectable.
That is exactly how the US healthcare system loses over $262 billion every year to claim denials — and why nearly 60 percent of denied claims are never resubmitted at all. Not because the claims were invalid. Because nobody on the billing team knew what the code meant or what the correct next step was.
This guide fixes that.
Whether you are a biller, a practice manager, a physician who just wants to understand why your revenue is not matching your patient volume, or an administrator building a denial management process from scratch — this is the reference you need. Every major medical billing denial code group is covered here: what CO means, what PR means, what OA means, which codes you see most often, why they happen, and exactly what to do when they show up on your EOB.
Bookmark this page. You will come back to it.
What Are Medical Billing Denial Codes — And Why Do They Exist?
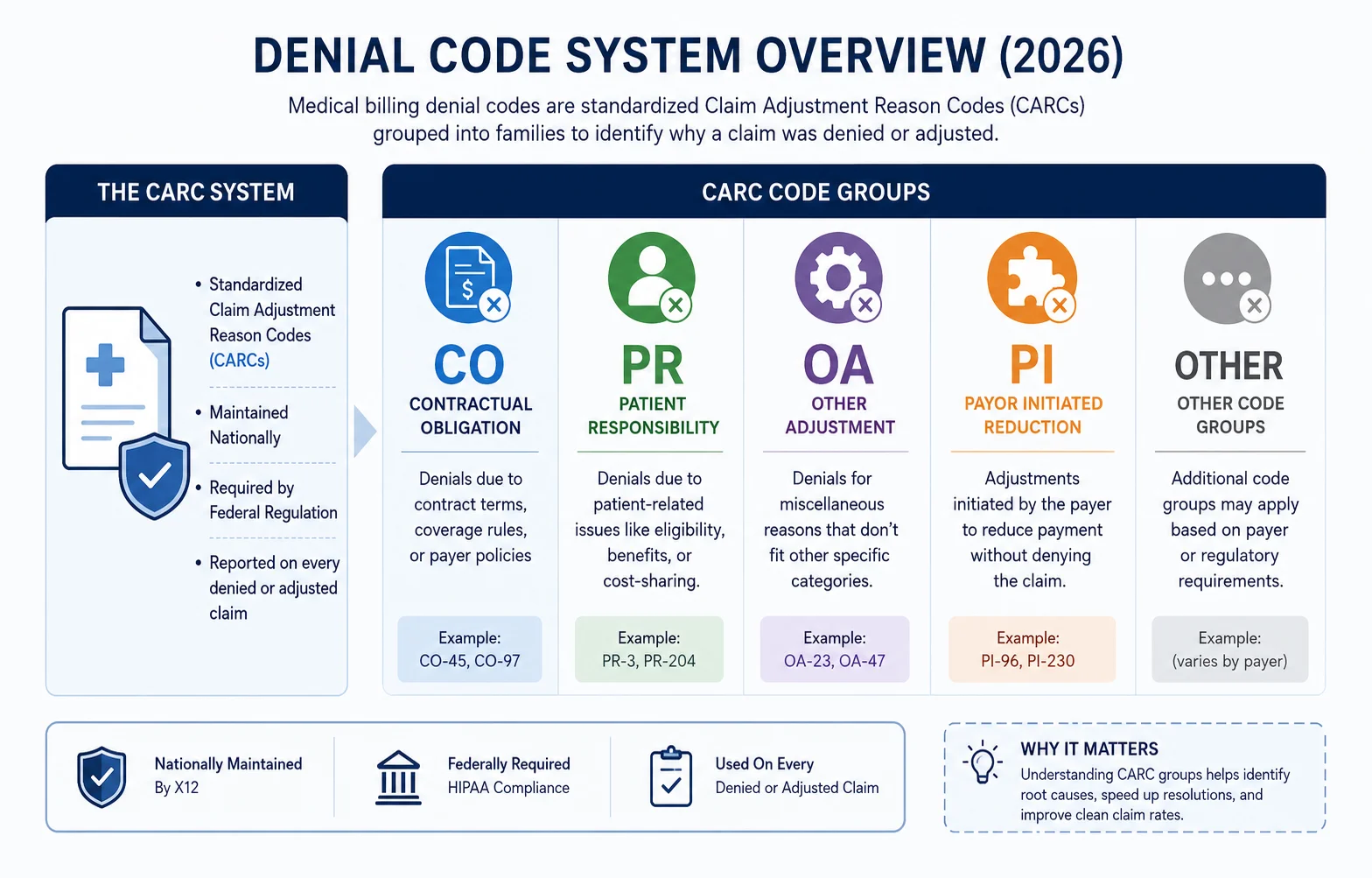
When a payer — Medicare, Medicaid, or any commercial insurance carrier — processes a claim and does not pay it in full, federal regulation requires them to explain exactly why. That explanation arrives through standardized codes called Claim Adjustment Reason Codes, or CARCs.
Every CARC is paired with a two-letter group code prefix that tells your billing team immediately who is financially responsible for the adjustment. Understanding that prefix is the single most important skill in denial management — because it determines your next action before you even look at the specific code number.
Here are the four group code prefixes and what each one means:
| Group Code | Full Name | What It Means | Patient Owes? |
|---|---|---|---|
| CO | Contractual Obligation | Provider absorbs the adjustment per payer contract | No |
| PR | Patient Responsibility | Patient owes this amount — copay, deductible, coinsurance | Yes |
| OA | Other Adjustments | Neither contractual nor patient responsibility — miscellaneous | No |
| PI | Payer Initiated | Payer’s internal adjustment — rare on standard EOBs | No |
Think of it this way: if you see PR on a denial code, the carrier is saying “the patient owes this, not us.” That is not a denial you appeal — it is a patient balance you collect. If you see CO, that is where most of your appeal energy goes, because CO denials are the ones where the carrier is withholding payment that may actually be owed to you.
Billing teams that do not map each denial to its group code prefix before taking action waste enormous amounts of time appealing the wrong things and billing patients incorrectly.
There is also an important distinction between a rejection and a denial that most billing teams blur:
- A rejection happens before adjudication — the claim never entered the payer’s system due to a technical error. Fix it and resubmit.
- A denial happens after adjudication — the claim was processed but payment was withheld. This requires an appeal, not just a resubmission.
These require completely different corrective actions and are tracked separately in any serious denial management workflow.
CO Denial Codes — Contractual Obligation (The Ones That Cost You the Most)
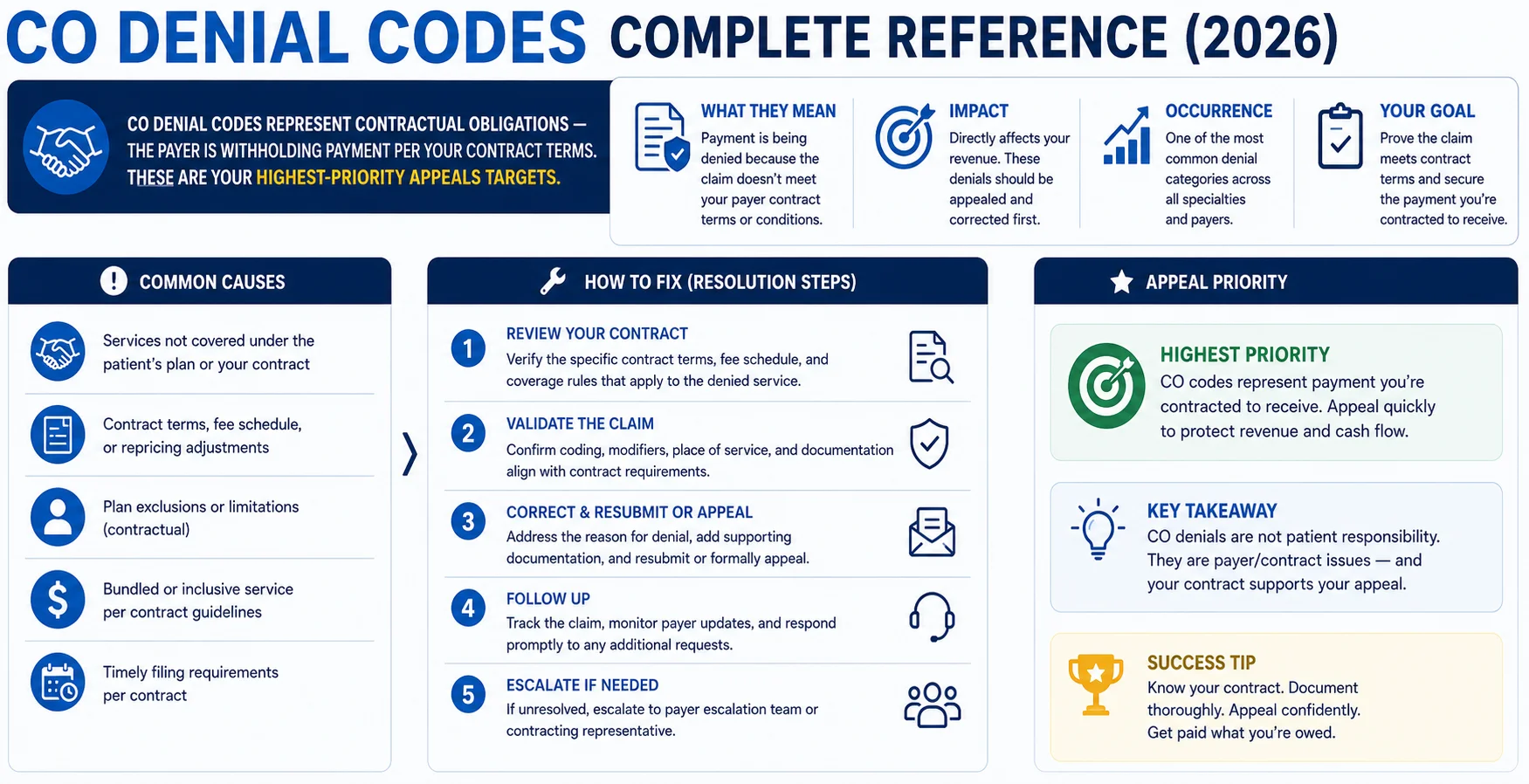
CO codes are contractual obligation adjustments — meaning the payer is reducing or withholding payment based on the terms of your provider contract. These are the codes your billing team should be most focused on, because they represent money your practice may be entitled to recover through appeals or corrective resubmission.
Here are the most common CO denial codes in 2026, what causes them, and exactly what to do:
CO-4 — Service Not Covered by This Payer or Contract
What it means: The service billed is not covered under the patient’s specific plan or your contract with that payer.
Common causes: Wrong payer billed, patient switched plans, service excluded from plan benefits, or billing a non-covered service.
What to do: Verify the patient’s active insurance coverage for the date of service. If the service is genuinely not covered, bill the patient if appropriate. If you believe coverage exists, request an explanation of benefits from the payer and cross-reference your contract.
Prevention: Run eligibility verification — including specific benefit checks — before every patient encounter, not just at check-in.
CO-11 — Diagnosis Code Does Not Support Medical Necessity
What it means: The ICD-10 diagnosis code submitted does not justify the procedure or service billed. The payer believes the treatment does not align with the documented condition.
Common causes: Diagnosis too vague or non-specific, wrong ICD-10 code selected, or mismatch between the documented diagnosis and the service provided.
What to do: Review the clinical documentation and confirm the most specific, accurate ICD-10 code for the patient’s condition. If the diagnosis genuinely supports the service, submit an appeal with supporting clinical notes. If the wrong code was selected, correct and resubmit.
Prevention: Train providers on ICD-10 code specificity. Use diagnosis-specific coding tools. Conduct quarterly coding audits. Our CodeMAXX services catch CO-11 patterns before they generate denials.
CO-15 — Authorization Number Missing, Invalid, or Does Not Apply
What it means: The claim requires a prior authorization that is either missing, incorrect, or not on file with the payer.
Common causes: Prior authorization was not obtained before the service, the authorization number was entered incorrectly on the claim, or the authorization was obtained for a different service or date.
What to do: Locate the authorization number and verify it matches the service, provider, date, and patient on the claim. If the authorization exists but was entered incorrectly, correct and resubmit. If no authorization was obtained, review whether a retroactive authorization is possible — some payers allow it in limited circumstances.
Prevention: Build a prior authorization tracking workflow that verifies authorization status before every scheduled procedure. The American Medical Association estimates prior authorization issues cost practices more than any other single denial category in terms of staff time.
CO-16 — Claim Lacks Information or Has Incorrect Information
What it means: The claim is missing required data, contains a technical error, or includes information that does not match payer records.
Common causes: Missing NPI, incorrect date of birth, absent or invalid CLIA number, mismatched place of service code, incorrect modifier, or demographic errors.
What to do: Review the claim line by line against the payer’s requirements. Identify the specific missing or incorrect field — the payer’s remittance advice often includes a Remittance Advice Remark Code (RARC) that narrows it down. Correct the error and resubmit as a corrected claim.
Prevention: CO-16 is the most common denial code in medical billing and the most correctable. <cite index=”42-1″>Most CO-16 denials trace back to missing NPI, incorrect date of birth, absent Social Security Number, invalid CLIA number, or a mismatched place of service.</cite> A pre-submission claim scrubbing process catches the majority of these before the claim ever leaves your system.
CO-18 — Duplicate Claim or Service
What it means: The payer believes this claim or service has already been submitted and processed.
Common causes: Claim submitted twice (accidentally or during a resubmission that was not flagged correctly), same service billed under two different claim numbers, or payer system error.
What to do: Pull the original claim and confirm whether it was previously processed and paid. If it was, do not resubmit. If the original was denied and you resubmitted correctly, contact the payer with both claim numbers and request a review.
Prevention: Maintain a submission log that tracks claim numbers and statuses. Never resubmit without first checking the status of the original claim.
CO-22 — This Care May Be Covered by Another Payer
What it means: The payer believes another insurance carrier has primary responsibility for this claim — a coordination of benefits issue.
Common causes: Patient has multiple insurance plans and the primary payer has not been billed first, or payer records show a different primary carrier than what your practice has on file.
What to do: Verify the patient’s complete insurance information and confirm the correct primary and secondary payer order. Bill the primary payer first, then submit the secondary claim with the primary’s explanation of benefits attached.
Prevention: Collect complete insurance information — including all secondary coverage — at registration. Update payer records any time a patient reports an insurance change.
CO-29 — Time Limit for Filing Has Expired
What it means: The claim was not submitted within the payer’s required filing deadline.
Common causes: Claim was delayed in submission, lost in a system transition, or the payer’s filing deadline was not tracked correctly.
What to do: If you have documentation proving timely filing — a submission confirmation, a clearinghouse report, or a payer acknowledgment — submit an appeal with that documentation. Without proof of timely filing, CO-29 denials are among the hardest to overturn.
Prevention: Track every payer’s filing deadline in your practice management system and build submission workflows that flag claims approaching the deadline. Common payer deadlines range from 90 days (some commercial plans) to 12 months (Medicare). Missing these is entirely preventable.
CO-45 — Charge Exceeds Fee Schedule or Maximum Allowable
What it means: The amount billed exceeds what your contract allows the payer to pay. The difference is a contractual write-off — you cannot bill the patient for it.
Common causes: This is often not a denial but a contractual adjustment — it is expected. If the amount seems unexpectedly low, your fee schedule may be outdated.
What to do: If you believe the payment is below your contracted rate, request a fee schedule from the payer and compare. If there is a discrepancy, file a contract dispute — not a standard appeal.
Prevention: Conduct annual fee schedule audits against current payer contracts. Underpayments from outdated fee schedules are one of the most invisible revenue leaks in medical billing.
CO-50 — Medical Necessity Not Established
What it means: The payer determined that the service billed was not medically necessary based on the documentation submitted.
Common causes: Insufficient clinical documentation, failure to demonstrate that the service met payer-specific medical necessity criteria, or documentation that does not align with the billed service.
What to do: Pull the complete clinical record for the date of service. Write a detailed appeal letter that specifically addresses the payer’s medical necessity criteria — cite clinical guidelines, patient history, and the medical rationale for the service. Attach all supporting documentation. <cite index=”42-1″>The average medical necessity denial amount climbed to $450 in 2025, a 70% increase year-over-year — and denied inpatient claims rose 12% from 2024 to 2025.</cite> These are worth fighting.
Prevention: Educate providers on documentation standards for medical necessity — especially for high-denial services like imaging, physical therapy, and specialist consultations. Medical necessity denials are almost always a documentation problem, not a clinical one.
CO-97 — Payment Included in Allowance for Another Service
What it means: The payer is bundling this service into the payment for another procedure already reimbursed on the same claim or a related claim.
Common causes: Billing for a service that payer policy considers part of a comprehensive procedure, or incorrect use of modifiers that should unbundle the service.
What to do: Review the payer’s bundling edits and NCCI (National Correct Coding Initiative) edits for the service combination. If the services are legitimately separate and distinct, append the appropriate modifier (most commonly modifier -59 or XU, XS, XE, XP) and resubmit.
Prevention: Review NCCI edits regularly. Our CodeMAXX services include bundling edit review before submission to prevent CO-97 denials at the source.
PR Denial Codes — Patient Responsibility (Collect From the Patient, Not the Payer)
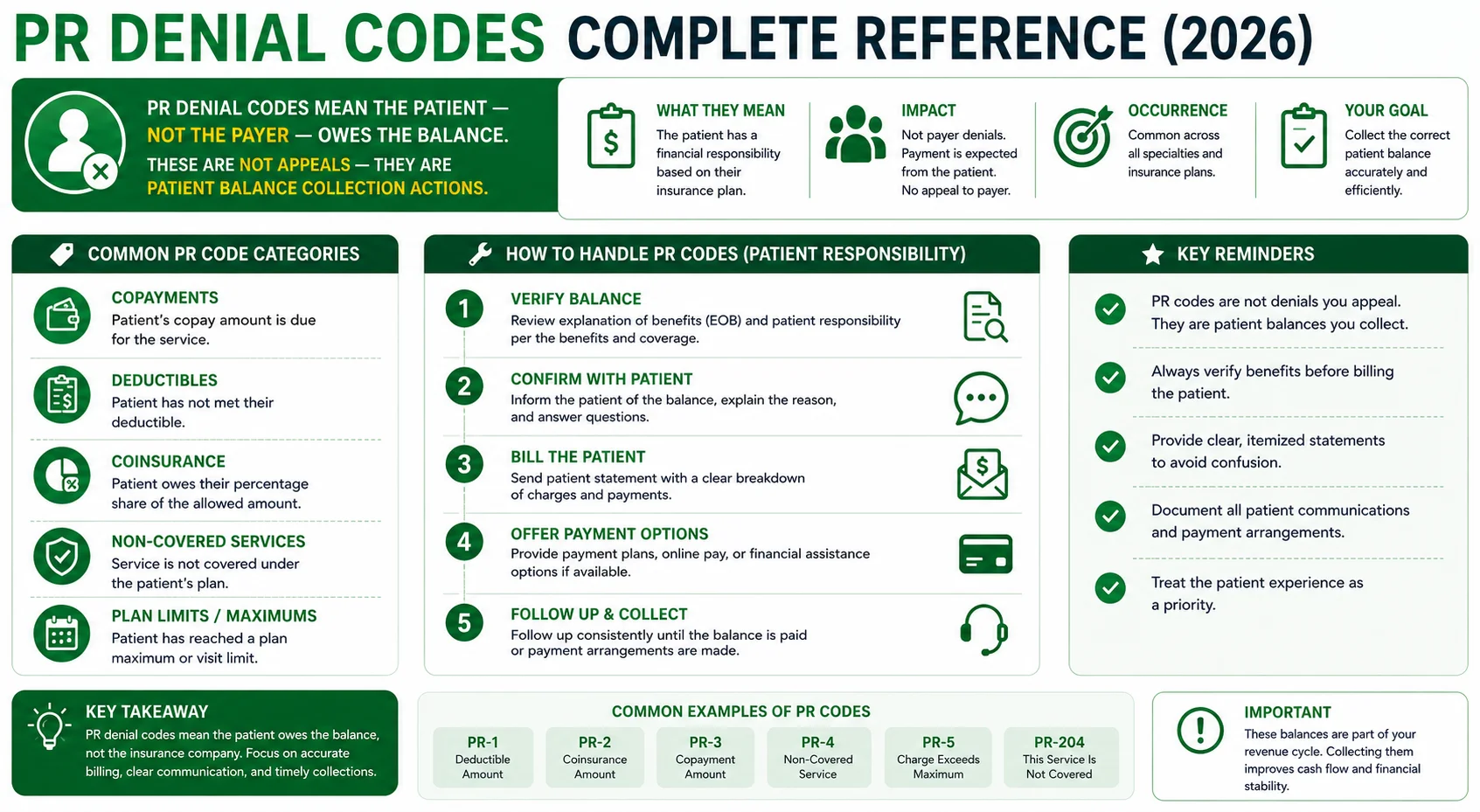
PR codes identify the portion of a charge that is the patient’s financial responsibility. These are not denials you appeal to the payer — they are balances you collect from the patient. Understanding the difference between a CO denial and a PR adjustment is essential for billing accuracy.
PR-1 — Deductible Amount
What it means: The patient has not yet met their annual deductible, and this amount applies toward it.
What to do: Bill the patient for this amount. Do not appeal to the payer — the payer has correctly applied the deductible.
Prevention: Check patient deductible status during eligibility verification before the visit. Collect estimated patient responsibility at time of service when possible.
PR-2 — Coinsurance Amount
What it means: This is the patient’s coinsurance portion — the percentage of the allowed amount the patient owes after the deductible is met.
What to do: Bill the patient for this amount. This is a standard cost-sharing determination, not an error.
Prevention: Verify coinsurance percentage during eligibility checks and communicate estimated patient cost to the patient before or at the time of service.
PR-3 — Copay Amount
What it means: This is the patient’s fixed copayment for the visit or service.
What to do: Collect the copay from the patient. If it was not collected at the time of service, bill the patient.
Prevention: Collect copays at the time of service, every time. Uncollected copays compound into significant revenue loss over time.
PR-96 — Non-Covered Charge — Patient Is Responsible
What it means: The service is not covered under the patient’s plan, and the patient is financially responsible for the full charge.
Common causes: Service explicitly excluded from the patient’s plan, patient received a non-covered elective service, or a coverage limitation applies.
What to do: Verify that the patient was informed of the non-covered status before the service was rendered — ideally through a signed Advance Beneficiary Notice (ABN) for Medicare patients or equivalent for commercial plans. Bill the patient for the non-covered amount.
Prevention: Run a benefit-level eligibility check that identifies specific exclusions before scheduling services. Use ABNs consistently for Medicare patients when a service may not be covered.
PR-204 — This Service, Equipment, or Drug is Not Covered Under the Patient’s Current Benefit Plan
What it means: Similar to PR-96 — the specific service or item is not a benefit under the patient’s current plan.
What to do: If the patient was not informed prior to service, you may face a collection challenge. Review your informed consent and financial responsibility documentation. If the patient was informed, bill them directly.
Prevention: Specialty-specific benefit verification before every encounter. Some services — particularly DME, certain injectable medications, and some behavioral health codes — are excluded from specific plan types at a surprisingly high rate.
OA Denial Codes — Other Adjustments (Neither Payer Nor Patient)
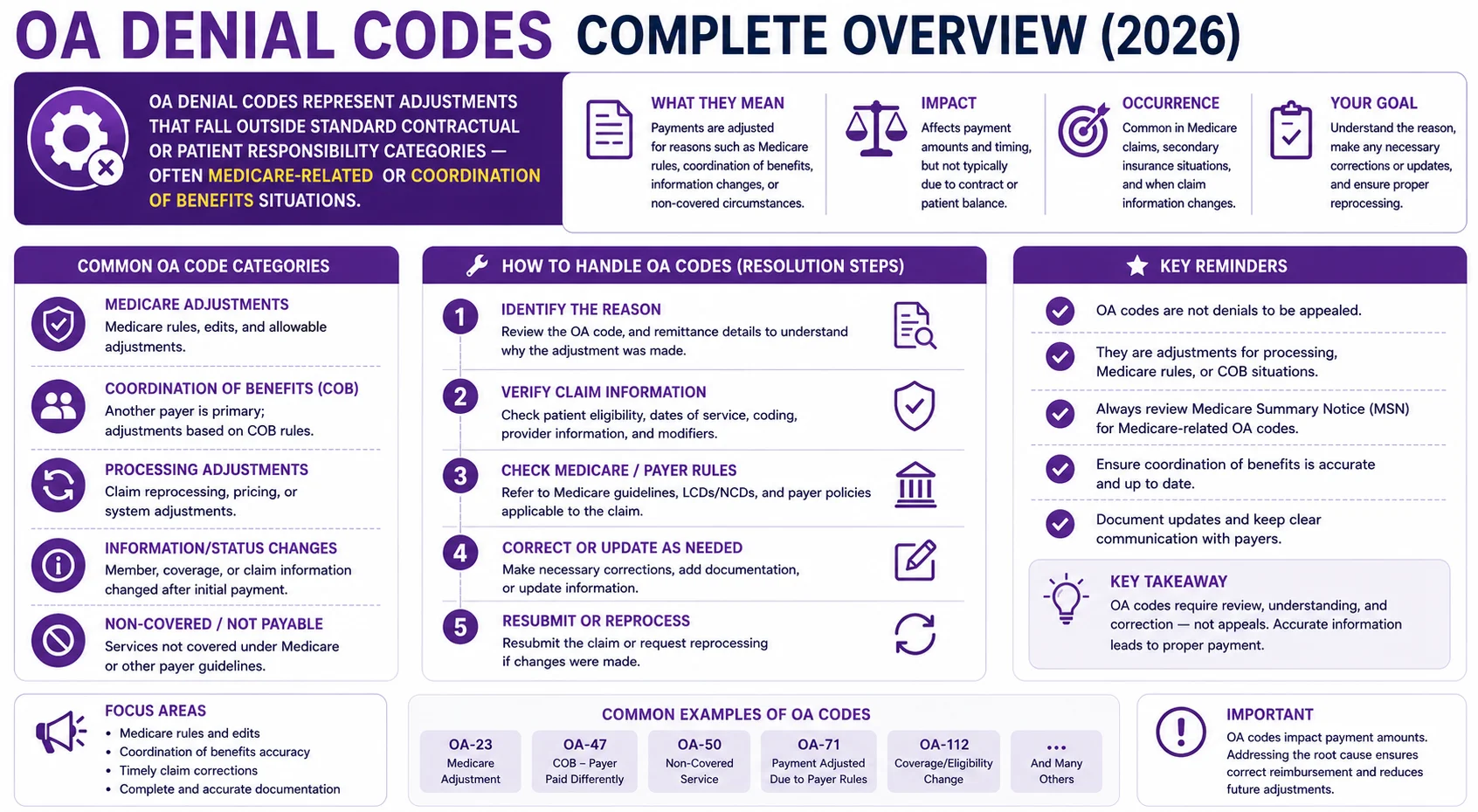
OA codes cover adjustments that do not fall neatly into contractual obligation (CO) or patient responsibility (PR) categories. They generally do not require provider action or patient billing — but understanding them prevents unnecessary appeals that waste staff time.
OA-18 — Duplicate Claim (Other Adjustment Category)
What it means: Same as CO-18 but classified differently based on payer adjudication rules. The payer considers this a duplicate submission.
What to do: Same as CO-18 — verify whether the original claim was processed and paid before taking any action.
OA-23 — Payment Adjusted Due to Enrollment or Disenrollment of Member
What it means: The patient was not enrolled in the plan on the date of service, or their enrollment status changed.
What to do: Verify the patient’s enrollment status for the exact date of service. If the patient was enrolled and the payer is in error, appeal with enrollment confirmation documentation. If the patient was not enrolled, explore other coverage or bill the patient.
Prevention: Real-time eligibility verification — not just at scheduling but at check-in on the day of service. Patient enrollment changes happen constantly and are one of the most common causes of OA-23 denials.
OA-109 — Claim Not Covered by This Payer
What it means: This payer is not responsible for the claim — either because another payer is primary or because the service falls outside this payer’s scope.
What to do: Verify which payer has primary responsibility and resubmit to the correct carrier. If this claim was sent to the wrong payer by mistake, submit to the correct one as quickly as possible to preserve your filing deadline.
OA-119 — Benefit Maximum for This Time Period Has Been Reached
What it means: The patient has exhausted a plan-specific benefit limit — such as a maximum number of physical therapy visits, mental health sessions, or chiropractic adjustments per year.
What to do: Inform the patient that their benefit has been exhausted. If appropriate, continue care as a self-pay patient. Review whether an appeal on clinical necessity grounds is viable under this specific plan.
Prevention: Track benefit limits for high-volume services during eligibility verification. For patients receiving ongoing care with visit limits, build a tracking system that flags when limits are approaching.
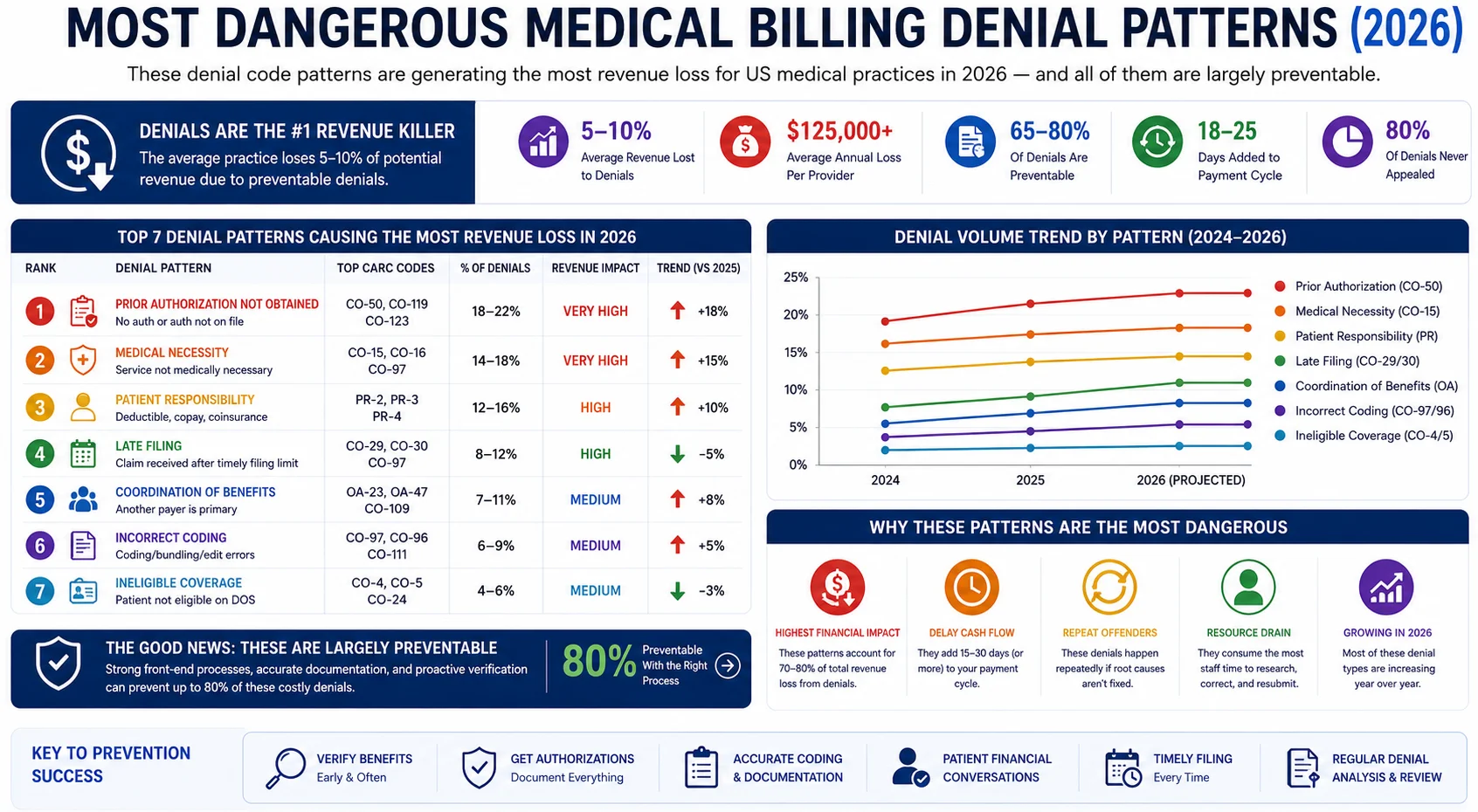
The Most Dangerous Denial Code Patterns in 2026
Individual denial codes matter. But what matters even more is recognizing denial patterns — because patterns reveal upstream problems in your billing workflow that will keep generating denials until someone fixes the root cause.
Here are the denial code patterns causing the most damage to practice revenue in 2026:
CO-15 + CO-50 combination (Prior Auth + Medical Necessity). When CO-15 and CO-50 appear together or in sequence on similar claim types, it usually means your prior authorization process is not capturing the clinical documentation the payer requires for medical necessity review. The fix is upstream — in how authorizations are requested and documented, not in how appeals are written.
CO-16 as a recurring pattern on the same provider. If CO-16 keeps appearing on claims from a specific rendering provider, the problem is usually a credentialing or enrollment issue — a missing NPI affiliation, an expired CLIA certificate, or an incorrect place of service designation in the practice management system. Fix the enrollment record, not individual claims.
CO-29 on claims over 90 days. If you are regularly seeing CO-29 denials — expired filing deadlines — you have a workflow problem, not a billing problem. Claims are not being submitted timely, and by the time denial management finds them, the appeal window is often also closed.
PR-96 without signed ABNs. If PR-96 denials are appearing on Medicare claims and you do not have signed Advance Beneficiary Notices on file, you have compliance exposure in addition to a collection problem. ABN management is a process issue that needs to be addressed practice-wide.
OA-23 in clusters. If you see a cluster of OA-23 denials — patient not enrolled on date of service — particularly at the start of a calendar year, it usually means you are not running real-time eligibility checks. January enrollment changes generate this pattern every year for practices that rely on stored eligibility data from the prior year.
How to Build a Denial Management Process That Actually Works
Most practices manage denials reactively — someone notices a claim is unpaid, looks it up, tries to figure out what happened. That approach is slow, incomplete, and systematically leaves recoverable revenue on the table.
A structured denial management process looks like this:
Step 1: Categorize every denial by CARC and group code the same day it arrives. Do not let denials sit in a queue uncategorized. Every denial should be logged with its group code (CO, PR, OA), its CARC number, the payer, the claim amount, and the date of the denial within 24 hours of receipt.
Step 2: Separate appeals from patient bills from write-offs immediately. CO denials go to your appeals workflow. PR denials go to your patient billing workflow. OA denials get reviewed and either appealed or closed. Mixing these up wastes enormous amounts of staff time.
Step 3: Set appeal priority by dollar value and appeal deadline. Not all denied claims are worth the same effort. Prioritize by dollar value — high-value denials get worked first. But always track deadlines — a $200 claim approaching its appeal window should be worked before a $2,000 claim with 60 days remaining.
Step 4: Track overturn rates by denial type and payer. If you are appealing CO-50 denials to a specific payer and winning 80 percent of them, you have a documentation process problem — those denials should not be happening in the first place. If you are winning only 10 percent, you need a different appeal strategy. Track what works.
Step 5: Feed denial data back upstream. Denial management that does not connect back to intake, scheduling, and coding is not management — it is firefighting. Every denial pattern should generate a process change upstream that prevents the same pattern next month.
If your practice does not have the bandwidth to build and maintain this workflow in-house, that is one of the strongest arguments for outsourcing billing to a company with structured denial management built into their service model. Our creative collection solutions are built around exactly this kind of systematic denial recovery and prevention.
Quick Reference: Most Common Medical Billing Denial Codes 2026
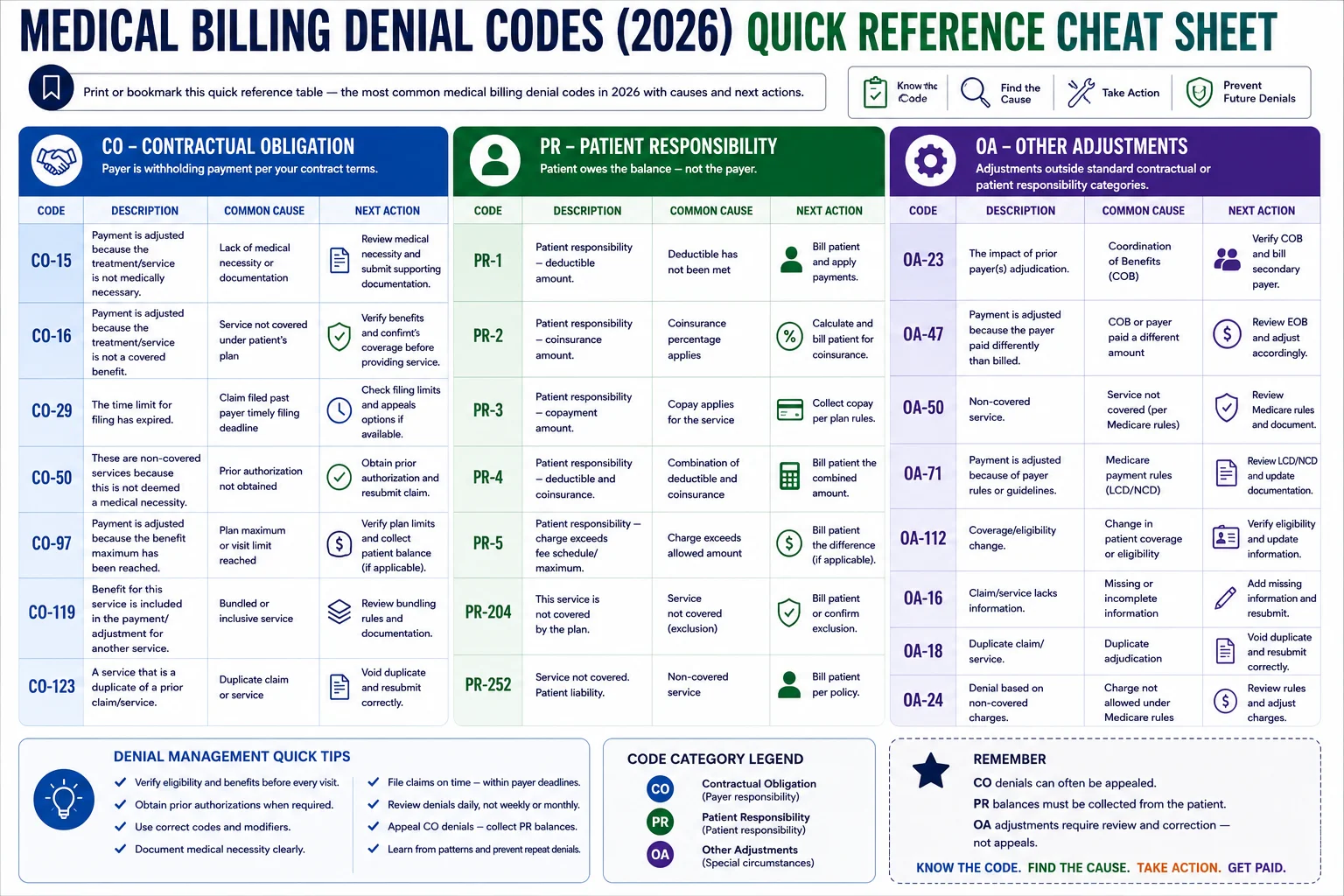
| Code | Group | Meaning | Next Action |
|---|---|---|---|
| CO-4 | CO | Service not covered | Verify coverage, bill patient if appropriate |
| CO-11 | CO | Diagnosis doesn’t support necessity | Correct ICD-10 code, resubmit or appeal |
| CO-15 | CO | Authorization missing or invalid | Locate auth number, correct and resubmit |
| CO-16 | CO | Claim missing or incorrect info | Identify specific field error, correct and resubmit |
| CO-18 | CO | Duplicate claim | Verify original claim status before acting |
| CO-22 | CO | Another payer may be primary | Verify COB order, bill correct primary first |
| CO-29 | CO | Filing deadline expired | Submit proof of timely filing if available |
| CO-45 | CO | Charge exceeds fee schedule | Review contracted rate, dispute if underpaid |
| CO-50 | CO | Medical necessity not established | Appeal with full clinical documentation |
| CO-97 | CO | Bundled into another service | Review NCCI edits, add correct modifier |
| PR-1 | PR | Deductible applies | Bill patient |
| PR-2 | PR | Coinsurance applies | Bill patient |
| PR-3 | PR | Copay applies | Collect from patient |
| PR-96 | PR | Non-covered — patient responsible | Bill patient with signed ABN if Medicare |
| PR-204 | PR | Not a covered benefit | Inform patient, bill if ABN obtained |
| OA-18 | OA | Duplicate (other adjustment) | Verify original claim before acting |
| OA-23 | OA | Enrollment/disenrollment issue | Verify eligibility for date of service |
| OA-109 | OA | Wrong payer billed | Identify correct payer, resubmit |
| OA-119 | OA | Benefit maximum reached | Inform patient, explore self-pay options |
How Pro Health Care Advisors Manages Denial Codes for Your Practice

Understanding denial codes is step one. Having the workflow infrastructure to catch, categorize, appeal, and prevent them — systematically, every month, across every payer — is the part that most in-house billing teams struggle to sustain.
At Pro Health Care Advisors, denial management is not a reactive process. It is built into every stage of the billing cycle.
Before the claim: Insurance eligibility verification catches CO-22 and OA-23 patterns before they happen. Prior authorization tracking prevents CO-15 denials at the source. Our HIPAA-compliant intake process collects the complete demographic and coverage information that prevents CO-16.
At submission: Our AAPC-certified coders review every claim for diagnosis-procedure alignment (CO-11), bundling edits (CO-97), and modifier accuracy before submission. Our CodeMAXX services add a dedicated coding accuracy layer that catches errors before they become denials.
After denial: Our creative collection solutions categorize every denial by CARC and group code on receipt, prioritize by value and appeal deadline, and maintain structured appeal workflows that recover denials other billing teams write off.
Across all specialties: From cardiology to mental health to family practice — we maintain payer-specific denial pattern knowledge across more than 30 specialties.
The result: a 98.5 percent clean claim rate and a denial rate under 2 percent — compared to the national average of 11.8 percent.
For more billing education, visit our articles and resources library. To understand how Medicare Advantage denials specifically are impacting practices, read our guide on Medicare Advantage denials rising 56 percent.
Frequently Asked Questions — Medical Billing Denial Codes 2026
Q: What is the most common medical billing denial code in 2026? CO-16 — claim missing or containing incorrect information — remains the single most frequently encountered denial code across all payer types and specialties. It is also the most correctable. Most CO-16 denials trace back to missing NPI, incorrect patient demographics, invalid CLIA numbers, or mismatched place of service codes. A pre-submission scrubbing process eliminates the majority of them.
Q: What is the difference between CO and PR denial codes? CO (Contractual Obligation) means the provider absorbs the adjustment per their payer contract — these are potential appeals targets. PR (Patient Responsibility) means the patient owes the balance — these are patient billing actions, not appeals. Mixing them up is one of the most common and costly billing team errors.
Q: Can you appeal a CO-50 medical necessity denial? Yes — and you often should, because the average medical necessity denial amount reached $450 in 2025, a 70 percent increase from the prior year. A successful CO-50 appeal requires a detailed letter citing the patient’s clinical history, the medical rationale for the service, and any applicable clinical guidelines or payer-specific medical necessity criteria. Attach all supporting documentation.
Q: What should I do if I keep getting CO-29 expired filing deadline denials? CO-29 denials are almost always a workflow problem, not a billing knowledge problem. Your claims are not being submitted within payer filing deadlines. Audit your submission process to identify where delays are occurring — common causes include unsigned encounter notes, incomplete charge capture, and claims sitting in a held status without follow-up. Build a deadline tracking system for every payer you bill.
Q: What is an OA denial code and do I need to appeal it? OA (Other Adjustments) codes represent adjustments that are neither contractual obligations nor patient responsibility. Many OA codes do not require action — they represent Medicare coordination of benefits adjustments, benefit maximum notifications, or enrollment determinations. However, OA-23 and OA-109 often indicate correctable issues worth addressing.
Q: Where can I find the complete official list of CARC codes? The complete and current list of Claim Adjustment Reason Codes is maintained by the Washington Publishing Company and updated regularly. This is the official source for all CARC codes used by Medicare, Medicaid, and commercial payers nationwide. CMS also publishes guidance on denial reason codes specific to Medicare claims.
Q: How do I reduce claim denials overall? The most effective denial reduction strategies address the upstream causes — not just the denial management response. Eligibility verification before every visit, prior authorization tracking, ICD-10 code specificity, and pre-submission claim scrubbing together address the root causes of the most common denial codes. For a deeper dive, read our complete guide on reducing claim denials.
The Bottom Line — Denial Codes Are a Symptom, Not the Problem

Every denial code on your explanation of benefits is a symptom of something that went wrong earlier in the billing cycle — at intake, at scheduling, at authorization, at coding, or at submission. The code tells you what happened. It does not fix what is broken.
That is why denial management without process improvement is just expensive firefighting. You can work every CO-16 and CO-50 and CO-29 that comes through your queue — and if the upstream problems are not fixed, the same denials will come back next month.
The practices that consistently maintain low denial rates are not staffed with superhuman billers. They have built systems that prevent denials before they happen. Pre-submission scrubbing. Real-time eligibility verification. Prior authorization tracking. Diagnosis-procedure alignment reviews. Systematic pattern analysis that feeds back into intake and scheduling.
That is what Pro Health Care Advisors builds for every practice we serve.
If your denial rate is above 5 percent — or if you are not sure what your denial rate actually is — that conversation starts with a free consultation.
Schedule Your Free Consultation with Pro Health Care Advisors →
We will review your current denial patterns, identify the upstream causes, and show you exactly what a structured denial prevention and management process looks like in practice.