How to Reduce Claim Denials | A Real, Step-by-Step Guide for Healthcare Practices in 2026
Picture this: your providers see patients all day. Your clinical team documents everything. Your billers submit the claims. And then — silence. The payer sends back a denial. Then another. Then five more.
Your team corrects what they can and resubmits. Some come back. Many don’t. And quietly, week after week, money your practice already earned just… disappears.
This is not a rare story. Out of $3 trillion in submitted medical claims, an average of $262 billion gets denied each year by healthcare organizations — roughly $5 million per provider. And here is the part that should really bother every practice manager: around 65% of medical claim denials are never resubmitted. MedsolercmMedsolercm
That is not a payer problem. That is a workflow problem. And workflow problems have solutions.
This guide gives you exactly that — a practical, plain-language playbook for reducing claim denials in 2026. No jargon-heavy theory. Just clear steps your team can actually use.
First, Let’s Get Honest About the Numbers
Before you can fix a denial problem, you need to understand how widespread it really is.
Claim denial rates are rising due to stricter payer requirements and more complex documentation processes, with industry averages now ranging between 8% and 12%, and over 40% of providers reporting denial rates above 10%. EDUCBA
Medicare Advantage initial denial rates averaged about 15.7%. Commercial payers’ initial denial rates have been estimated at roughly 13.9%. Dr. Credentialing
Commercial plan denials rose 1.5% from 2023 to 2024, while Medicare Advantage denials spiked 4.8% in the same period — a meaningful signal given how aggressively Medicare Advantage has expanded its share of U.S. beneficiaries. Medsolercm
Practices with poor billing automation and staff training see denial rates of 15% to 20%, compared to a benchmark of 5% to 7% for well-managed practices. Each reworked denied claim costs an average of $25 in administrative time. Thecredentialing
So if your practice is submitting 1,000 claims a month at a 12% denial rate, that is 120 denials — costing $3,000 in rework time alone, before you count the delayed or lost revenue.
Now here is the good news that most billing guides bury: between 60% and 90% of denied claims result from avoidable front-end errors, not clinical disputes. The fix is not a legal battle with an insurer — it is a workflow problem with the right processes and the right training. EDUCBA
That means the majority of your denial problem is completely within your control to fix.
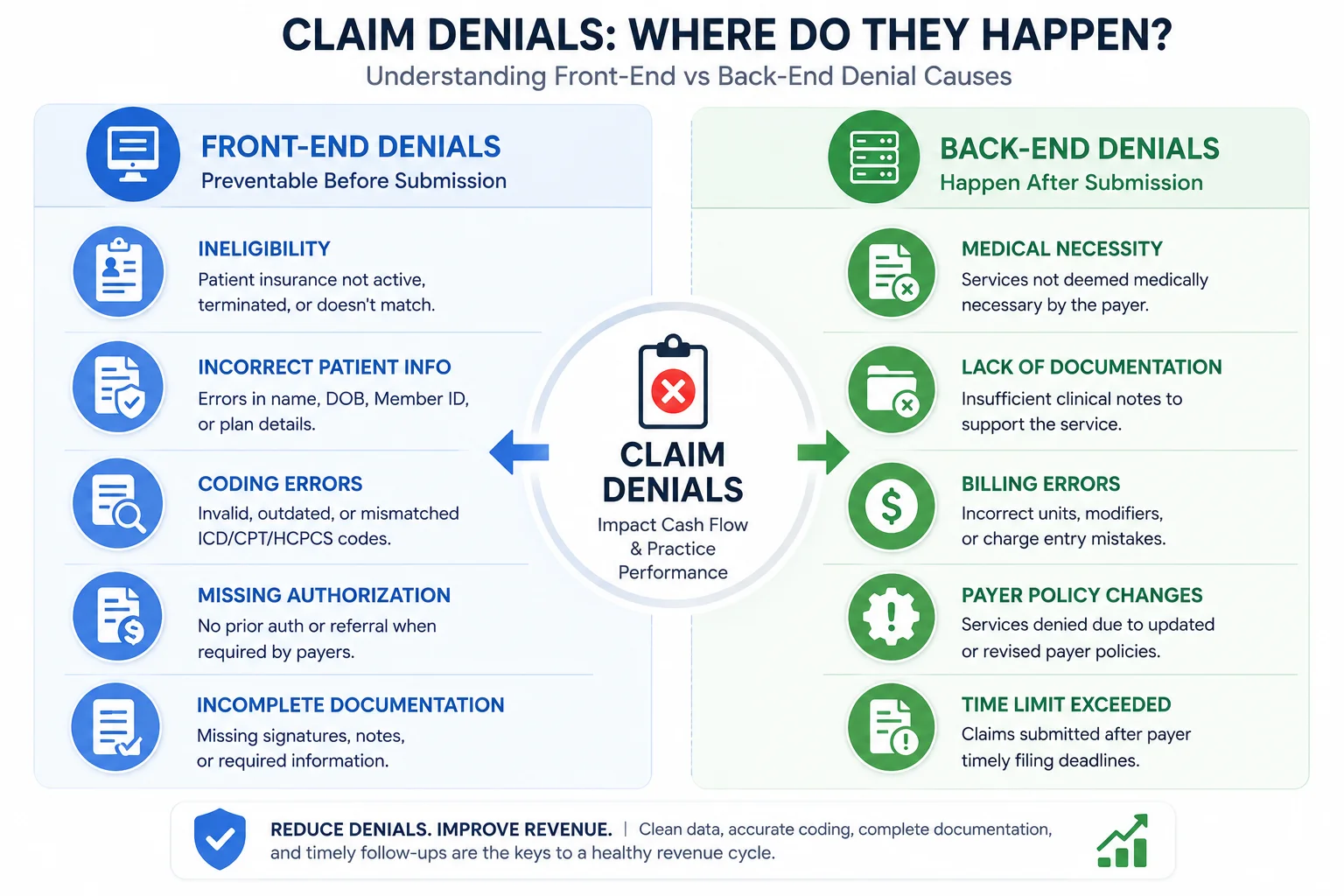
Understanding the Two Types of Claim Denials
Not all denials are the same — and treating them the same is one of the biggest mistakes practices make. Claim denials fall into two categories based on where in the revenue cycle the problem starts. Medical Billers and Coders
Front-End Denials happen before or at the time of service:
- Patient eligibility not verified before the appointment
- Insurance coverage expired or inactive on the date of service
- Prior authorization not obtained before a procedure
- Incorrect patient demographic information — wrong date of birth, misspelled name, wrong policy number
Back-End Denials happen during or after claim submission:
- Incorrect ICD-10 or CPT codes
- Missing or wrong modifiers
- Lack of medical necessity documentation
- Duplicate claim submissions
- Timely filing limit missed
- Coordination of benefits issues
Separating denials into front-end and back-end categories is the first step in building an effective denial reduction strategy. Each category requires a different fix and a different team member to own it. Medical Billers and Coders
Most practices treat all denials the same and wonder why nothing improves. The ones that fix the root cause — and assign ownership — are the ones that get results.
Strategy 1 — Verify Insurance Eligibility Before Every Single Visit
This is the single highest-impact change most practices can make — and it costs almost nothing to implement correctly.
Nearly 42% of claim denials stem from demographic or eligibility errors. And 60% of front-desk teams fail to re-verify eligibility at the point of care, despite coverage often changing between scheduling and the service date. Prohealthcareadvisors
Insurance changes constantly. Patients lose coverage. Deductibles reset. Plans switch mid-year. A patient who was fully covered at their last visit three months ago may have a completely different plan today — and if you don’t catch it before the appointment, you will find out the hard way when the claim comes back denied.
Practices that verify eligibility twice — at scheduling and on the day of service — consistently report lower front-end denial rates than those that check only once. Medical Billers and Coders
A comprehensive eligibility check must also include coordination of benefits (COB). Many COB denials occur because primary and secondary insurance information is outdated or incorrectly sequenced. Resolving these issues at the front desk prevents weeks of back-end billing follow-up and appeals. Hospitalogy
What good eligibility verification looks like in practice:
- Run automated eligibility checks 48 hours before every scheduled appointment
- Re-verify at check-in on the day of service
- Confirm copay, deductible status, and in-network status every visit — not just the first one
- Flag any discrepancies and resolve them before the patient leaves the building
Our medical billing and practice management team runs eligibility verification for every patient, every visit — automatically — so your front desk never has to choose between checking insurance and managing a waiting room.
Strategy 2 — Make Prior Authorization a Non-Negotiable Workflow Step
Prior authorization denials are among the most frustrating because they are entirely preventable — and yet they keep happening.
The reason is simple: authorization requirements vary by payer, by plan, by procedure, and sometimes even by patient. What United Healthcare approves without auth, Blue Cross might require a full medical necessity review for. What was approved last year might require auth this year because the payer quietly updated its policy.
Create a master list of procedures that require prior authorizations for each payer and each plan. Designate specific staff members to own the authorization process, and use electronic prior authorization portals that auto-populate CPT and diagnosis fields. Build automated alerts into your scheduling system that notify staff when an authorization is required before an appointment can be confirmed. Prohealthcareadvisors
The 2026 CMS Prior Authorization API Rule now requires electronic processing for many payer types — which creates both faster approvals and faster rejections for practices that submit incomplete requests.
Our prior authorization services track authorization requirements by payer and procedure, submit requests, and follow up on every pending auth before the service date — so your providers never walk into a procedure that isn’t covered.
Strategy 3 — Fix Your Coding Accuracy at the Source
The American Medical Association estimates up to 12% of medical claims are submitted with inaccurate codes. And inaccurate coding is not just a technical billing issue — it is a compliance issue. Consistent undercoding leaves money on the table. Consistent upcoding creates audit risk. And wrong codes create denials, period. Thecredentialing
Documentation and coding issues contribute significantly to denials, with front-end processes playing a critical role — accurate intake alone can reduce denials by up to 30%. EDUCBA
The most common coding errors driving denials in 2026:
- Using deleted or outdated ICD-10 codes — new codes took effect January 1, 2026; practices that haven’t updated their charge masters are submitting stale codes
- Missing or incorrect modifiers — a claim for a bilateral procedure without the correct modifier is automatically denied by most payers
- Mismatched diagnosis and procedure codes — the ICD-10 code must clinically support the CPT code billed; when they don’t align, the claim fails medical necessity review
- Unbundling — billing separately for procedures that payers require to be billed together under one code
- Using non-specific codes — ICD-10 requires the most specific code available; vague or unspecified codes often trigger additional documentation requests or outright denials
Leading billing teams adopt smarter coding strategies such as routine internal coding audits focused on denial trends, and rather than treating coding as an isolated function, they integrate coders into denial analysis discussions. P3care
Our CodeMAXX certified coding services use AAPC-certified coders who specialize by specialty — so the coder working your cardiology claims knows cardiology CPT rules cold, not just general coding principles.
Strategy 4 — Submit Clean Claims Through a Clearinghouse Scrubber
A claim scrubber is software that checks every claim for errors before it reaches the payer. Think of it as a spell-check for your billing — except instead of catching typos, it catches missing modifiers, invalid code combinations, payer-specific formatting issues, and demographic mismatches.
Practices using claim scrubbers see a 15% to 25% drop in rejections. Prohealthcareadvisors
A good clearinghouse scrub catches:
- Invalid NPI numbers
- Missing referring provider information
- Incorrect place-of-service codes
- Code combinations that violate NCCI edits
- Claims missing required attachments for specific payers
- Date of service formatting errors
Our billing team submits all claims through a clearinghouse with real-time scrubbing built in. Our current clean claim rate sits at 98.5% — meaning nearly every claim we submit passes on the first attempt. That number directly translates to faster payments and lower denial volume for the practices we serve.
Strategy 5 — Build a Denial Tracking System That Finds Patterns
Here is where most practices leave enormous money on the table. They work denials reactively — someone gets a denial, corrects it, and moves on. Nobody asks why it keeps happening.
Practices that implement formal denial tracking and root cause analysis reduce their denial rates by an average of 25% within the first year, according to the Healthcare Financial Management Association. Siriussolutionsglobal
Effective denial tracking means:
- Categorizing every denial by reason code (CARC/RARC)
- Tracking denials by payer, provider, procedure code, and date of service
- Identifying which front desk staff, which providers, or which payer rules are generating the most denials
- Running monthly denial reports and actually reviewing them in team meetings
Payers like UnitedHealthcare and Aetna frequently update their policy edits. If you are not tracking patterns, you are reacting too late. MBW RCM
Is one front desk staff member’s patients experiencing more eligibility denials? These insights guide targeted interventions that address root causes rather than just symptoms. Siriussolutionsglobal
Our creative collection solutions team tracks denial patterns across every payer and every provider for our clients — identifying the recurring issues and fixing them at the source, not just working each denial individually.
Strategy 6 — Appeal Every Recoverable Denial — Fast
When a denial does come through, speed matters.
Industry best practice is to resolve or appeal denials within 48 to 72 hours of receiving them. Delays reduce the chance of successful reimbursement and increase the risk of revenue write-offs. Psych NP Fellowship
Studies show that 57% of denied claims that are appealed are successfully overturned. That is more than half. Which means every denial your team does not appeal is money you are voluntarily leaving behind. EDUCBA
A strong denial appeal process includes:
- Logging every denial the day it is received
- Categorizing by denial type and determining if it is correctable or clinically disputable
- Pulling the original claim, clinical notes, and authorization documentation
- Submitting the corrected claim or formal appeal with supporting documentation
- Tracking the appeal status and following up before the deadline
Payer timely filing limits for appeals range from 30 to 180 days depending on the contract. Missing that window means the denial becomes permanent — no matter how valid your case.
Strategy 7 — Keep Your Provider Credentialing Current
This one surprises people. Credentialing gaps cause denials — and they are among the hardest to detect because everything looks normal on the surface. Claims go out, payers acknowledge receipt, and then a denial arrives weeks later citing provider enrollment issues.
Patient insurance may be expired, or the member ID may be incorrect — but enrollment-related denials often trace back to the practice’s own credentialing records, not the patient’s coverage. Clinicmind
A provider whose enrollment has lapsed at one payer generates denials for every claim submitted to that payer until the lapse is corrected. And if monthly monitoring is not in place, that lapse can go undetected for 60 to 90 days.
Our physician credentialing services include active monthly monitoring of every provider’s enrollment status across all payers — so credentialing lapses get caught before they become denial storms.
Strategy 8 — Train Your Front Desk Like It’s a Revenue Function (Because It Is)
Your front desk team is not just scheduling patients and collecting copays. They are the first checkpoint in your entire revenue cycle. Every piece of information they collect — or fail to collect — either protects or threatens your cash flow.
Front-end accuracy is no longer a clerical function — it is a strategic revenue protection role. Organizations that invest in training and accountability at registration see dramatic reductions in downstream denials. P3care
Front desk training that actually reduces denials covers:
- How to read an insurance card and verify network status
- What information is required at check-in versus what can wait
- How to handle patients with multiple insurance plans
- When to flag a visit for prior authorization review before it reaches the clinical team
- How to communicate billing concerns to patients professionally and clearly
The practices we work with that see the fastest denial rate improvements are almost always the ones that invested in front desk workflow — not just back-end billing fixes.
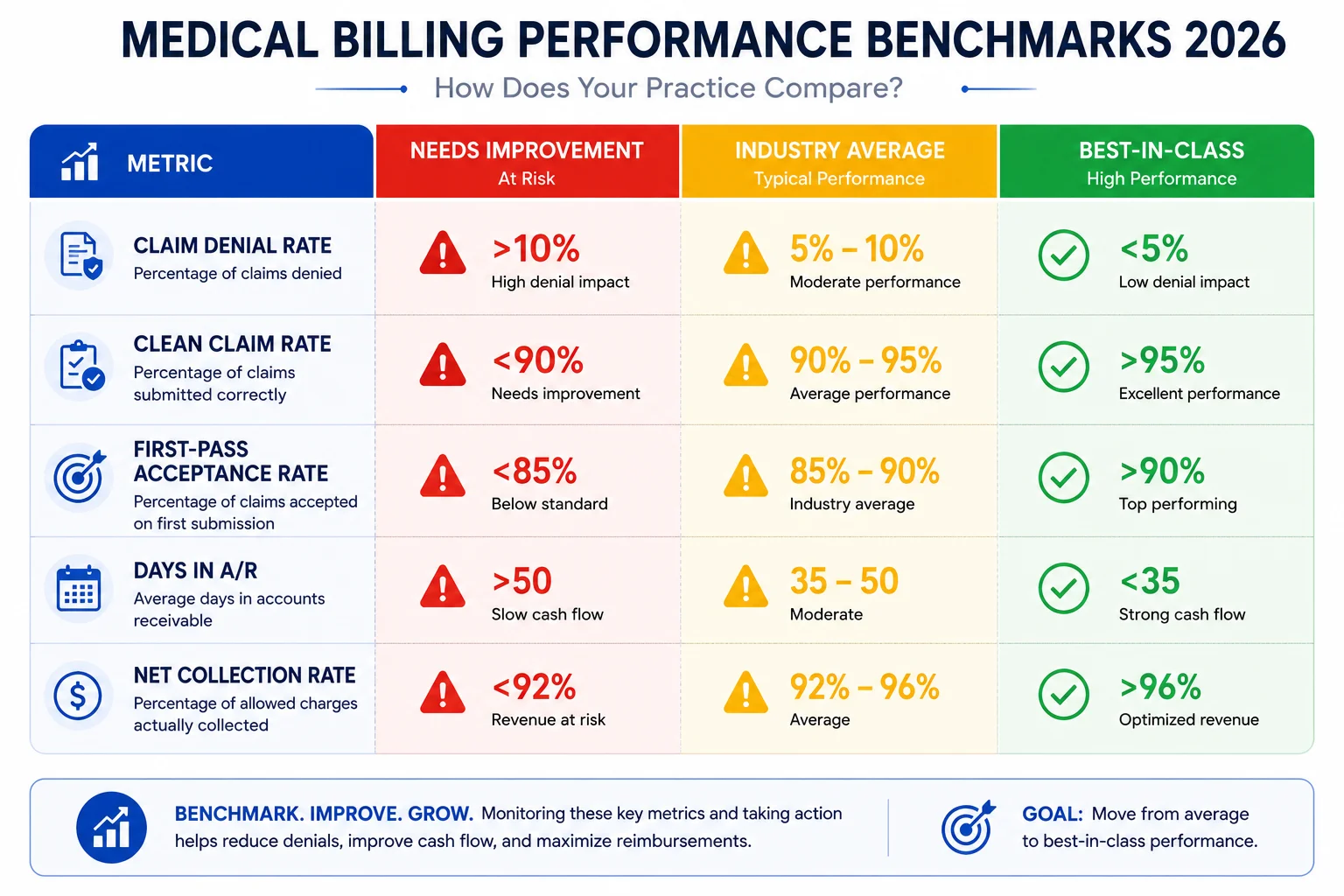
What Your Denial Rate Should Actually Be
Here are the benchmarks your practice should be measuring against:
| Metric | Industry Average | Best-in-Class Target |
|---|---|---|
| Overall denial rate | 8%–12% | Under 3% |
| Clean claim rate | 85%–90% | Above 95% |
| First-pass resolution rate | 75%–80% | Above 90% |
| Days in AR | 45–60 days | Under 35 days |
| Appeal overturn rate | 40%–50% | Above 57% |
If your numbers are outside the best-in-class column, the gap between where you are and where you should be represents real, recoverable revenue.
The Real Cost of a High Denial Rate
Let’s put concrete numbers to what denial rates actually cost at different practice sizes:
A practice billing $300,000 per month with a 10% denial rate has $30,000 in denied claims every 30 days. Even if 70% of those are eventually recovered, $9,000 per month — $108,000 per year — is written off or permanently lost.
A practice billing $800,000 per month at the same denial rate has $80,000 in denied claims monthly. At a 70% recovery rate, that is $24,000 per month — $288,000 per year — gone.
These are not hypothetical numbers. They are what we see when we do revenue audits for practices coming to us for the first time. The money is real. The leakage is real. And it stops when the right processes are in place.
Explore our full revenue cycle management services to see how we approach denial reduction across the entire billing cycle.
Common Questions About Claim Denial Reduction
What is the fastest way to reduce claim denials right now?
Start with eligibility verification — verify every patient 48 hours before the appointment and again at check-in. This single change addresses up to 42% of front-end denials and can show results within the first billing cycle.
Should we appeal every denial?
Appeal every denial that is clinically or administratively supportable and within the payer’s filing window. Do not automatically write off denials just because reworking them takes time. Given that more than half of appealed claims are overturned, the math strongly favors appealing.
How do we know which payers are causing the most denials?
Run a monthly denial report broken down by payer and denial reason code. Most practice management systems can generate this. If yours cannot, that is a problem worth solving — because without payer-level visibility, you are billing blind.
How long should the denial appeal process take?
Most correctable denials should be reworked and resubmitted within 24 to 48 hours of receipt. Formal clinical appeals may take 5 to 10 business days to build properly. The key is having a structured process so nothing sits in a queue waiting for someone to have time.
What is a good clean claim rate to aim for?
Above 95% is considered strong. Above 98% is best-in-class. Our team maintains a 98.5% clean claim rate across the practices we manage.