IN-HOUSE VS OUTSOURCED MEDICAL BILLING 2026 — WHICH ONE ACTUALLY MAKES YOUR PRACTICE MORE MONEY?
Let us start with something most billing articles will not say out loud.
Most practices that think they are saving money by billing in-house are not.
They are paying a salary — maybe two — and calling it done. But they are not counting the software. They are not counting the benefits, payroll taxes, and PTO. They are not counting the training and recertification costs. They are not counting what happens when their biller takes two weeks of vacation and a backlog builds up. And they are absolutely not counting the money that quietly disappears every month through undercoded visits, missed denials, and claims that age past the point of recovery.
When you count all of that — and we will show you exactly how — the math almost always tells a different story than the one most practices are telling themselves.
This guide is a genuine, honest comparison of in-house versus outsourced medical billing in 2026. Not a sales pitch. Not a one-sided argument. A real look at what each model costs, what each one produces, and how to figure out which one is right for your specific practice.
Why This Decision Matters More Than Ever in 2026
<!– ============================================================ 🖼️ IMAGE #2 — HEALTHCARE BILLING CHALLENGE GRAPHIC / STAT INFOGRAPHIC Place: Right after this heading, before the paragraph text ALT Text: medical billing market 2026 outsourcing statistics revenue cycle management growth Caption (optional): The medical billing outsourcing market reached $19.5–$21.8 billion in 2026 — driven by rising denial rates, staffing shortages, and growing payer complexity. Size: Full width or large inline ============================================================ –>
Medical billing has never been more complicated — and the gap between practices that handle it well and practices that do not has never been wider.
Here is the current state of the industry:
The national initial claim denial rate hit 11.8 percent in 2024 and has continued rising into 2026. That means nearly 1 in 8 claims is being denied on first submission nationally — and in some states and specialties, the rate runs far higher.
The average in-house billing operation collects between 85 and 90 percent of allowable charges. A specialist outsourced billing partner with active denial management typically collects between 93 and 97 percent. On a practice collecting $200,000 per month, that difference is $6,000 to $14,000 in additional revenue — every single month — that the in-house model is leaving uncollected.
The medical billing outsourcing market reached an estimated $19.5 to $21.8 billion in 2026 and is growing at approximately 12 percent annually. That growth is not driven by marketing — it is driven by practice owners doing the actual math and realizing the outsourced model outperforms in-house billing on nearly every measurable dimension.
Staffing pressures are making it worse. The healthcare industry is experiencing significant billing staff turnover — with annual turnover rates in medical billing roles running between 33 and 40 percent. Every departure means a training investment, a productivity gap, and a period of elevated claim errors. For small and mid-size practices, that cycle is expensive and exhausting.
With all of this in the background, the in-house versus outsourced decision in 2026 is not just an operational preference — it is a strategic financial choice that directly affects your practice’s revenue, margins, and long-term viability.
The Real Cost of In-House Medical Billing — The Number Most Practices Get Wrong
<!– ============================================================ 🖼️ IMAGE #3 — IN-HOUSE BILLING TRUE COST BREAKDOWN INFOGRAPHIC Place: Right after this heading, before the cost breakdown ALT Text: true cost of in-house medical billing 2026 breakdown salary software benefits training Caption (optional): Most practices estimate in-house billing costs between $45,000–$60,000 per year. The real number is $70,000–$120,000 when all hidden costs are included. Size: Full width / infographic or comparison table style ============================================================ –>
Here is the honest truth: most practices dramatically underestimate what in-house billing actually costs. They look at the salary line item and stop there. That approach misses most of the actual cost.
Here is a realistic breakdown for a small to mid-size practice (2 to 3 providers, approximately 3,000 encounters per year):
Visible Costs — What You Know You Are Paying
Biller salary: A medical billing specialist in the US earns an average of $42,000 to $58,000 per year depending on experience, specialty knowledge, and location. Larger practices typically need two or more billers.
Benefits and payroll taxes: Employer-side benefits — health insurance, retirement contributions, payroll taxes, workers compensation — add approximately 25 to 35 percent on top of base salary. On a $50,000 salary, that is an additional $12,500 to $17,500 per year.
Practice management and billing software: Most billing software subscriptions run between $300 and $1,500 per month. Clearinghouse fees, ERA processing, and eligibility check fees add another $100 to $400 per month. Annual software costs: $4,800 to $22,800.
Training and certification: AAPC and AHIMA coding certifications cost $300 to $600 to obtain and require ongoing continuing education to maintain. Annual training budget for one certified biller: $500 to $1,500.
Hidden Costs — What Most Practices Are Not Counting
Turnover and replacement: With billing staff turnover running at 33 to 40 percent annually, the average practice replaces a biller every 2.5 to 3 years. Recruiting, onboarding, and training a replacement costs between $4,000 and $12,000 per hire — plus 60 to 90 days of reduced productivity during the transition.
Vacation, sick days, and coverage gaps: When your biller is out, claims do not stop coming in. Either they pile up — which ages your AR and creates denial risk — or you pay overtime, temp agency costs, or cross-train other staff to cover. Neither option is free.
Denied claims that never get worked: In-house billing teams operating without structured denial management workflows typically work only the high-value denials. Small and mid-value denials get deprioritized, aged, and eventually written off. For a practice collecting $150,000 per month, even a 3 percent unworked denial rate is $4,500 per month in permanent revenue loss.
Undercoded visits: Studies across Georgia, California, and nationwide consistently identify undercoding as one of the most common — and most overlooked — revenue leaks in in-house billing operations. Practices lose 6 to 9 percent of net collections to systematic undercoding that an experienced outsourced coder would catch and correct.
Manager and physician time: Every hour a physician or practice manager spends reviewing billing reports, handling billing questions, or fixing billing errors is an hour not spent on patient care or practice growth. At a physician’s billing rate, even 2 hours per week of billing oversight costs $10,000 to $30,000 per year in opportunity cost.
What the Real Number Looks Like
When you add up all of these components, the true annual cost of in-house billing for a small to mid-size practice typically runs between $70,000 and $120,000 per year — not the $45,000 to $60,000 most practices estimate when they only count salary and software.
For many practices, that number alone changes the conversation.
The Real Cost of Outsourced Medical Billing — And What You Actually Get
<!– ============================================================ 🖼️ IMAGE #4 — OUTSOURCED BILLING COST MODEL GRAPHIC Place: Right after this heading, before the pricing breakdown ALT Text: outsourced medical billing cost model 2026 percentage of collections pricing Caption (optional): Outsourced billing typically costs 4–9% of net collections — but the performance improvement in collections often more than covers the fee. Size: Medium to large / inline ============================================================ –>
Outsourced billing is typically priced as a percentage of net collections. In 2026, the standard range is 4 to 9 percent for most practice types and sizes. Here is what that looks like in real numbers:
| Monthly Net Collections | 5% Fee | 7% Fee | 9% Fee |
|---|---|---|---|
| $50,000 | $2,500 | $3,500 | $4,500 |
| $100,000 | $5,000 | $7,000 | $9,000 |
| $200,000 | $10,000 | $14,000 | $18,000 |
| $500,000 | $25,000 | $35,000 | $45,000 |
For high-complexity specialties — cardiology, oncology, orthopedic surgery — fees may reach 10 to 12 percent due to coding complexity and higher prior authorization volume.
What the Fee Covers — And Why It Often Pays for Itself
Unlike in-house billing where you pay for inputs (salaries, software, training) regardless of results, outsourced billing is performance-based. The billing company only makes more money when you collect more money. That alignment of incentives is one of the most important structural differences between the two models.
A quality outsourced billing partner includes:
- AAPC-certified coding and claim submission
- Insurance eligibility verification before every visit
- Prior authorization management
- Payment posting and ERA reconciliation
- Denial management and structured appeals
- AR follow-up and aged claim recovery
- Real-time reporting and dashboard access
- Credentialing support (at many companies including Pro Health Care Advisors)
Most of these functions would require multiple in-house staff members to replicate — and even then, the depth of expertise in payer-specific billing rules is rarely matched.
The Revenue Performance Argument
This is where the math really shifts. The average in-house billing operation collects 85 to 90 percent of allowable charges. A specialist outsourced billing partner with active denial management typically collects 93 to 97 percent.
On a practice collecting $200,000 per month, that 6 to 8 percent collection rate improvement is $12,000 to $16,000 per month in additional revenue — every month, every year — compared to what the in-house model was actually collecting (not what it was billing).
That revenue improvement almost always exceeds the outsourcing fee. Which means for most practices, outsourcing does not cost more than in-house billing — it generates more net revenue than in-house billing while costing less in total overhead.
Many growing practices report overall cost savings of 40 to 60 percent when converting from fixed in-house overhead to outsourced performance-based billing — once all true costs are properly accounted for.
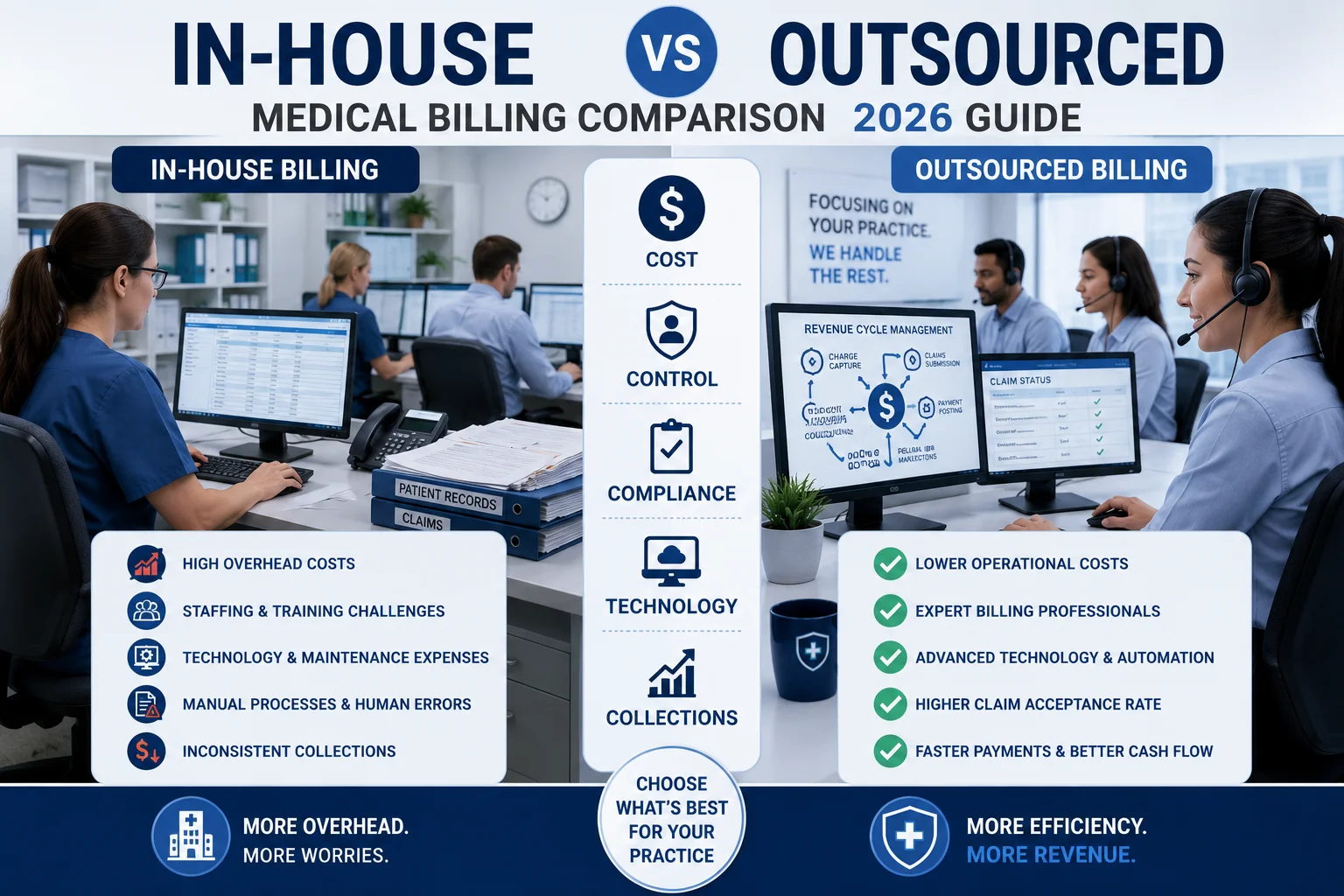
Side-by-Side Comparison — In-House vs Outsourced Medical Billing 2026
<!– ============================================================ 🖼️ IMAGE #5 — SIDE BY SIDE COMPARISON TABLE / GRAPHIC Place: Right after this heading, showing the comparison table visually ALT Text: in-house vs outsourced medical billing side by side comparison 2026 table Caption (optional): A direct comparison of in-house and outsourced medical billing across cost, performance, compliance, and flexibility in 2026. Size: Full width / table or comparison graphic ============================================================ –>
| Factor | In-House Billing | Outsourced Billing |
|---|---|---|
| True Annual Cost (small practice) | $70,000–$120,000 | 4–9% of collections |
| Clean Claim Rate | 85–92% (average) | 95–98.5% (top providers) |
| Net Collection Rate | 85–90% | 93–97% |
| Denial Management | Reactive, capacity-dependent | Structured, systematic |
| Coding Accuracy | Varies by staff training | AAPC-certified |
| Staff Turnover Risk | High (33–40% annual) | None — your problem |
| HIPAA Compliance | Your responsibility | Shared — BAA required |
| Payer Rule Updates | Depends on training budget | Ongoing — billing company’s job |
| Scalability | Hire more staff to scale | Scales with collections |
| Credentialing | Separate vendor or in-house | Often included |
| Reporting / Visibility | Depends on software | Dashboard — real-time |
| Control Over Process | High | Moderate |
| Response to Regulation Changes | Slow — training required | Fast — built-in expertise |
What In-House Does Better
Control and immediate accessibility are the genuine advantages of in-house billing. Your biller knows your practice, your providers, and your patient population. They are physically present. Questions get answered in person. Some practice owners value that deeply — and for practices with very high collections volumes (typically $1.5 million or more per year) or with in-house billing teams that are genuinely exceptional, in-house billing can be competitive.
The key qualifier is “genuinely exceptional.” That means AAPC-certified coders, structured denial management workflows, systematic prior authorization tracking, and a clean claim rate above 95 percent. Most in-house billing operations are not operating at that level — and many practice owners do not know it because they are measuring submitted claims rather than collected revenue.
What Outsourced Billing Does Better
Almost everything else. Performance-based pricing. No turnover risk. AAPC-certified coding. Structured denial management built around payer-specific rules. Real-time reporting. Scalability without hiring. Ongoing compliance with payer rule changes that most in-house teams cannot keep up with.
For practices under $1.5 million in annual collections — and honestly for many practices well above that threshold — the outsourced model produces more net revenue, at lower total cost, with less administrative risk.
The Hidden Risks of In-House Billing That Most Practices Discover Too Late
<!– ============================================================ 🖼️ IMAGE #6 — RISK / WARNING GRAPHIC Place: Right after this heading, before the risk list ALT Text: hidden risks of in-house medical billing 2026 denial management compliance staff turnover Caption (optional): These are the in-house billing risks that quietly cost practices thousands before they show up on a report. Size: Medium / inline ============================================================ –>
The financial comparison tells most of the story. But there are risks specific to in-house billing that go beyond the cost numbers.
The Single Point of Failure Problem
When your billing depends on one or two people, you are one resignation, one medical leave, or one extended vacation away from a billing crisis. Claims pile up. Denials go unworked. AR ages. By the time you hire and train a replacement, you have 60 to 90 days of billing backlog that can take months to fully recover.
This is not a theoretical risk. It happens in practices of every size, in every state, every year.
The Compliance Exposure Problem
Payer rules change constantly. CMS updates its guidelines. State Medicaid programs revise prior authorization requirements. New coding regulations take effect. Keeping one or two in-house billers current on all of these changes — across every payer your practice bills — requires a training investment most practices do not budget for.
When billing falls behind on compliance, the consequences range from avoidable denials to audit findings to HIPAA violations. None of these outcomes are free. Our HIPAA compliance services and MD Audit Shield RAC service are specifically built to prevent exactly these outcomes.
The Undercoding Invisibility Problem
Undercoded claims are harder to detect than denied claims. A denied claim shows up in your AR report. An undercoded claim gets paid — just for less than you were entitled to. Practices losing 6 to 9 percent of net collections to systematic undercoding often have no idea it is happening because the money never appears as an obvious line-item loss.
Our CodeMAXX services provide a dedicated layer of coding accuracy review designed to identify and correct the undercoding patterns that quietly reduce in-house billing revenue month after month.
The Technology Gap Problem
Medical billing software in 2026 includes AI-assisted coding, predictive denial management, real-time eligibility verification, and automated prior authorization tools. Quality outsourced billing companies invest continuously in these technologies and apply them across their entire client portfolio. Most in-house billing teams are working with practice management software that has not been significantly updated in years — and neither have their workflows.
When In-House Billing Makes Sense — Honestly
<!– ============================================================ 🖼️ IMAGE #7 — DECISION FLOWCHART GRAPHIC Place: Right after this heading, before the criteria list ALT Text: when to keep medical billing in-house vs outsource decision flowchart 2026 Caption (optional): Use this decision framework to determine whether in-house or outsourced billing is the right model for your practice size and situation. Size: Full width / flowchart or decision tree graphic ============================================================ –>
In the interest of giving you a genuinely useful guide — not just a pitch for outsourcing — here is when keeping billing in-house actually makes sense.
Your practice collects $1.5 million or more annually AND you have invested in a genuine billing team. At 16 or more providers with $8 million or more in collections, in-house billing becomes economically viable if you build the right infrastructure — AAPC-certified staff, quality software, structured denial management workflows, and active compliance monitoring. Budget $65,000 to $97,500 per billing FTE fully loaded, plus $12,000 to $60,000 per year in software.
Your billing team already performs at a certified, measurable level. If your in-house team maintains a clean claim rate above 95 percent, a net collection rate above 93 percent, and a denial rate below 5 percent — with documentation to prove it — you have a genuinely high-performing in-house operation. That is worth keeping.
You have tried outsourcing and been disappointed. Not all billing companies are equal. Some are genuinely not good. If you have had a bad outsourcing experience, the answer is not necessarily to bring billing back in-house — it may be to choose a better billing partner. But the experience is real and worth acknowledging.
Your specialty has very low billing complexity. A cash-pay or very high self-pay practice — like some cosmetic surgery or concierge medicine models — has minimal insurance billing complexity. In these cases, in-house billing may be genuinely cost-effective.
For most practices that do not meet these specific conditions — and that is the majority of small and mid-size practices in the country — the honest answer is that outsourcing will produce better financial outcomes.
How to Evaluate Any Outsourced Billing Company — What the Numbers Should Look Like
Not all outsourced billing companies perform equally. Choosing the wrong outsourced billing company is sometimes worse than in-house billing — because you have less visibility into what is going wrong. Here is what to specifically ask and verify before signing any contract.
Clean claim rate above 98 percent. The national benchmark is 95 percent. The best companies in 2026 operate at 98 percent or higher. Our medical billing and practice management team at Pro Health Care Advisors maintains a 98.5 percent clean claim rate.
Denial rate under 3 percent. The national average denial rate is 11.8 percent. A denial rate above 5 percent at a billing company means their clean claim submission is not as strong as they claim. Our denial rate is under 2 percent.
AAPC or AHIMA certified coders. Ask specifically for certification confirmation. Non-certified coding staff generate systematic undercoding and miscoding errors that cost you money.
Payer-specific experience for your state and specialty. A billing company that is genuinely experienced in your payer environment will be able to name the specific plans they have billed, the prior authorization challenges they have navigated, and the denial patterns they have encountered. Generic answers mean generic billing.
Real-time AR reporting. You should have access to your billing data at any time — not monthly summaries. Transparent reporting is not a feature — it is a basic expectation.
Credentialing included or available. Credentialing gaps are a common revenue leak for practices that manage billing and credentialing through separate vendors. A billing company that handles both eliminates that coordination failure. See our physician credentialing service for how this works in practice.
Denial management with documented appeal rates. Ask for their denial overturn rate. Ask how quickly they respond to denials. Ask whether they have a dedicated appeals team or whether denials go into the same queue as new submissions.
No flat fees — percentage of collections only. Percentage-based pricing aligns the billing company’s income with your results. Flat fees remove that incentive. Avoid billing companies that charge flat fees regardless of what they collect.
For more on what to look for in a billing partner, read our full guide on how to reduce claim denials and our breakdown of Medicare Advantage denials rising 56 percent.
What Pro Health Care Advisors Offers — And Why It Matters for This Decision
<!– ============================================================ 🖼️ IMAGE #8 — PRO HEALTH CARE ADVISORS TEAM / BRANDING Place: Right after this heading ALT Text: Pro Health Care Advisors outsourced medical billing team AAPC certified HIPAA compliant 2026 Caption (optional): Pro Health Care Advisors — AAPC-certified billers, 98.5% clean claim rate, under 2% denial rate, full RCM and credentialing services. Size: Full width or large ============================================================ –>
Pro Health Care Advisors is a HIPAA-compliant medical billing and revenue cycle management company serving healthcare practices across the United States. If you are evaluating the outsourced model, here is what our service looks like in practice.
98.5% clean claim rate. Well above the national benchmark of 95 percent — and well above what most in-house billing teams produce.
Under 2% denial rate. Compared to a national average of 11.8 percent. The difference shows up directly in your net collections every month.
Full revenue cycle management. Insurance eligibility verification. Prior authorization management. Clean claim submission. Payment posting. Denial management and appeals. AR follow-up. Collections. Everything under one roof through our medical billing and practice management services.
Physician credentialing included. Our physician credentialing service handles CAQH verification, payer enrollment, and re-credentialing management — eliminating the billing gaps that credentialing delays create.
Audit protection. Our MD Audit Shield RAC service provides documentation review and audit response support that protects your practice from RAC audit findings.
Creative collection solutions. Our creative collection solutions recover denied and aged claims with structured follow-up workflows that most in-house teams cannot sustain.
HIPAA-compliant data security. Our HIPAA compliance services include signed BAA management, risk assessment protocols, and breach response planning built into every client relationship.
30+ specialties. We serve practices across cardiology, family medicine, mental health, wound care, urology, oncology, and many more. See our full specialties list.
Transparent reporting. You have real-time access to your billing performance data — not monthly summaries delivered two weeks after the period closes.
For more education on billing and revenue cycle management topics, visit our articles and resources library.
Frequently Asked Questions — In-House vs Outsourced Medical Billing 2026
Q: How much does outsourced medical billing actually cost in 2026? Most reputable billing companies charge between 4 and 9 percent of net collections. For small to mid-size practices, most competitive quotes fall between 5 and 8 percent. High-complexity specialties like cardiology and oncology may see rates of 10 to 12 percent due to coding and prior authorization complexity.
Q: Is outsourced billing really cheaper than in-house billing? For most practices, yes — when you count all true in-house costs including benefits, software, training, turnover, and denied claim losses. The true annual cost of in-house billing for a small practice typically runs $70,000 to $120,000, compared to what many practices estimate as $45,000 to $60,000. Many practices report 40 to 60 percent cost savings after switching to outsourced billing.
Q: Will I lose control of my billing if I outsource it? You lose direct physical control — meaning you do not have a biller sitting in your office. But you should gain transparency through real-time reporting dashboards that show you more about your billing performance than most in-house teams actually report. Loss of visibility is a sign of a bad billing company, not outsourcing in general.
Q: What happens to my in-house billing staff if I outsource? This is a real human consideration. Some practices reassign billing staff to front-desk, patient communication, or other administrative roles. Others phase the transition gradually. This is a management decision that varies by practice — but it is worth planning for before making the switch.
Q: How long does it take to see results after switching to outsourced billing? Most practices see measurable improvement in clean claim rate and denial rate within 30 to 60 days of a well-managed transition. Full revenue optimization — including recovery of any AR backlog from the previous billing operation — typically takes 90 days.
Q: What if I have a billing backlog when I switch? Request a free AR analysis before starting the transition. Our creative collection solutions are specifically designed to recover denied and aged claims from previous billing operations — including claims that previous billing teams gave up on.
Q: Does Pro Health Care Advisors handle physician credentialing too? Yes. Our physician credentialing service handles the entire enrollment process — CAQH verification, payer enrollment applications, re-credentialing management, and follow-up tracking. Managing billing and credentialing through one company eliminates the coordination gaps that delay revenue for new providers.
The Bottom Line — Making the Right Decision for Your Practice
<!– ============================================================ 🖼️ IMAGE #9 — CTA / FREE CONSULTATION IMAGE Place: Right before the final CTA paragraph ALT Text: schedule free medical billing consultation Pro Health Care Advisors in-house vs outsourced 2026 Caption (optional): Not sure which billing model is right for your practice? Schedule a free consultation and we will run the real numbers with you. Size: Full width or large ============================================================ –>
Here is the honest summary of everything this guide has covered.
For most practices — particularly those collecting under $1.5 million per year, those dealing with staffing instability, those in complex payer markets, or those whose in-house billing is not performing at a certified, measurable level — outsourced billing produces better net revenue, at lower total cost, with less operational risk than in-house billing.
That is not a sales pitch. That is what the numbers say when you count everything.
But the right answer for your practice depends on your specific size, specialty, payer mix, and current billing performance. The best thing you can do right now is find out where you actually stand — not where you think you stand.
That starts with a real conversation about your current billing numbers. Clean claim rate. Denial rate. Net collection rate. AR aging. Days in AR. Those five numbers will tell you more about your billing than any amount of general advice.
Pro Health Care Advisors will review those numbers with you for free — and tell you honestly what they mean.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pressure. No generic sales pitch. Just a real look at your billing performance and an honest conversation about whether we can improve it — and by how much.