Prior Authorization in Medical Billing | Complete 2026 Guide for Healthcare Practices
Your provider orders an MRI. Your patient needs it. Everyone in the room knows it’s medically necessary. But before the scan happens, someone on your billing team has to stop everything, call the insurance company, fill out a form, wait days for a response, and then — more often than not — fight a denial.
This is prior authorization. And in 2026, it just got a lot more complicated.
A survey of 1,000 practicing physicians found that 95% reported prior authorization delays access to necessary care. 79% said patients had abandoned recommended treatment because of authorization challenges. And 26% reported that prior auth delays had led to a serious adverse event in their practice. Billmate
Those are not just quality-of-care numbers. Every abandoned treatment, every delayed procedure, every authorization that falls through the cracks is also a billing failure — a service your practice delivered or planned to deliver that never got paid.
The cumulative revenue loss from prior authorization inefficiencies across the US healthcare system has been estimated at $23 to $31 billion annually. DrCatalyst
The good news: 2026 brought the most significant regulatory reforms to prior authorization in over a decade. The rules changed. Payers have new obligations. And practices that understand the new landscape can use it to their advantage — getting approvals faster, appealing denials more effectively, and protecting revenue that used to quietly disappear.
This guide covers everything your practice needs to know — in plain language, with real steps your team can use starting today.
At Pro Health Care Advisors, prior authorization management is one of the core services we handle for practices nationwide. We have seen firsthand what poor PA workflows cost — and what fixing them recovers.
What Is Prior Authorization in Medical Billing?
Prior authorization — also called prior auth, PA, or pre-authorization — is the process of getting formal approval from an insurance company before providing a specific service, procedure, medication, or referral.
It is not optional. If a payer requires prior authorization for a service and you provide that service without obtaining it first, the claim will be denied. Not delayed — denied. And in most cases, that denial is not overturnable on appeal, because the issue is not clinical; it is procedural.
Prior authorization is commonly required for:
- Advanced imaging (MRI, CT scans, PET scans)
- Elective and outpatient surgeries
- Specialty referrals (cardiology, neurology, orthopedics, oncology)
- Durable Medical Equipment (DME)
- Physical, occupational, and speech therapy beyond a set number of sessions
- High-cost or brand-name medications
- Mental health and substance use disorder services beyond initial visits
- Home health services
The challenge is that what requires authorization varies by payer, by plan, by procedure code, and sometimes by patient demographics. What United Healthcare approves without auth, Aetna may require a full clinical review for. What was not on a payer’s auth list last year may have been quietly added this year.
The average medical practice now completes 39 prior authorizations per physician per week, with staff spending roughly 13 hours weekly on related paperwork. DrCatalyst
That is nearly two full working days per physician per week — spent on administrative work that generates zero patient care value and zero direct revenue.
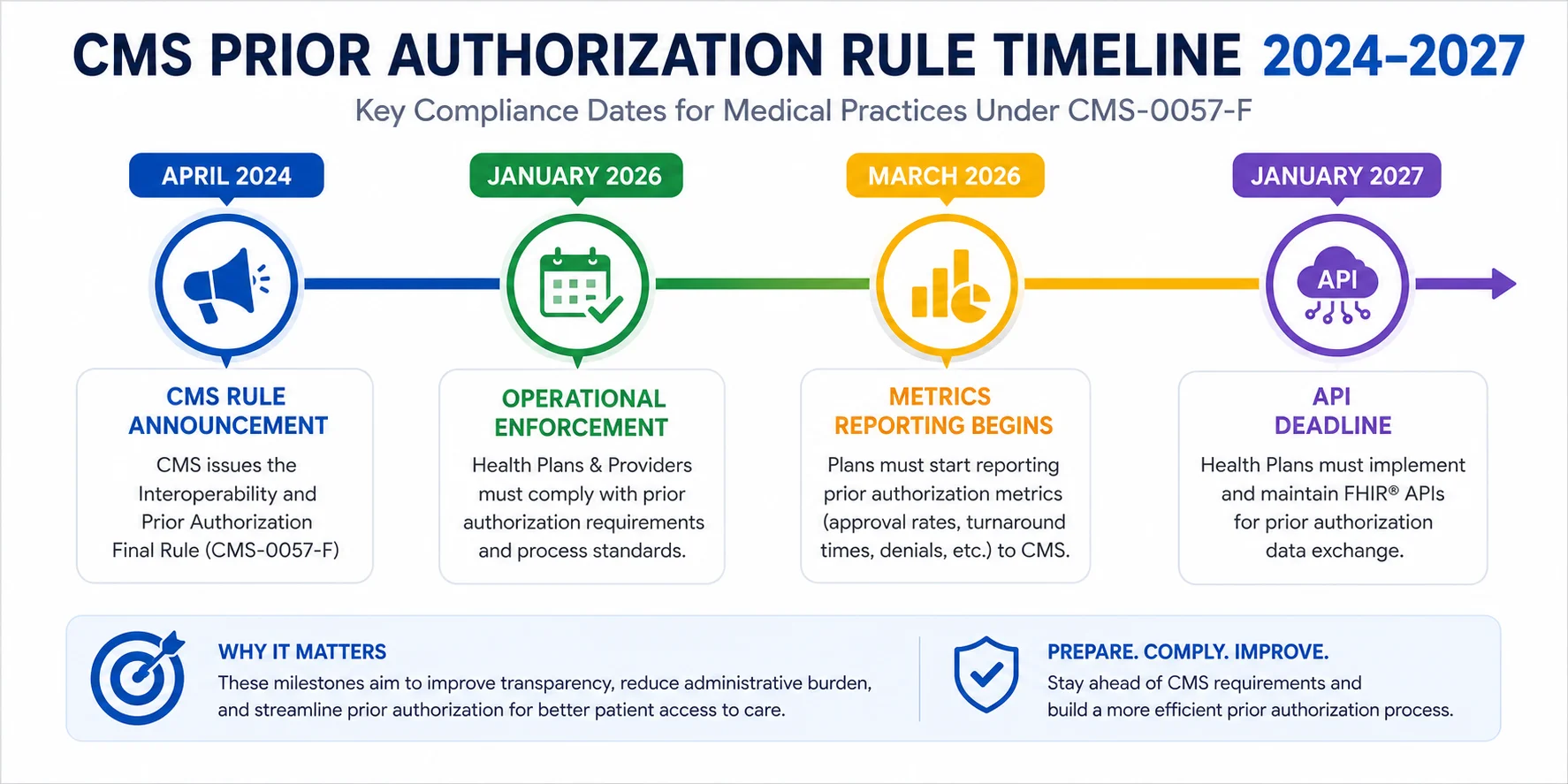
The 2026 CMS Prior Authorization Rule: What Actually Changed
This is the part most guides skip or bury. But if you bill Medicare Advantage, Medicaid managed care, CHIP, or Qualified Health Plans on the Federal Exchange, January 1, 2026 changed your prior authorization obligations in ways you cannot afford to ignore.
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) went into operational effect on January 1, 2026. Three things changed at once. billrMD
Change 1 — Decision Windows Cut in Half
Standard prior authorization decisions now have a 7 calendar day limit. Before this rule, many payers took up to 14 days. That window is cut in half. billrMD
For urgent or expedited requests — situations involving urgent medical need — payers must respond within 72 hours. Not business days. Hours.
What this means for your workflow: If your team is still building their follow-up schedule around the old 14 calendar day window, they are calling too late. Pending requests should be flagged for review at day 4, escalated at day 6, and reported as overdue at day 8. For expedited requests: flag at hour 24, escalate at hour 48, overdue at hour 72. billrMD
Build this into your practice management system as an automated rule — not a memory test that depends on which biller happens to be working that day.
Change 2 — Specific Denial Reasons Now Required
Beginning in 2026, payers must provide a specific reason for every denied prior authorization, regardless of how the request was submitted. No more vague “does not meet criteria” rejections. DrCatalyst
This is a major win for practices. Vague denial language used to make appeals nearly impossible — you did not know what to fix, so you could not correct the submission. Now payers must tell you exactly why the request was denied, which gives your team the specific information needed to appeal correctly and quickly.
Change 3 — Payers Must Now Publicly Report Their Denial Metrics
Payers must publish aggregated prior authorization metrics on their public websites annually, including approval rates, denial rates, average decision turnaround times, and appeals outcomes. The first reporting period covers calendar year 2025, with data due by March 31, 2026. DrCatalyst
This unprecedented transparency means practices can now compare payer performance and make informed contracting decisions. Medicare Advantage plans report the highest approval rates at around 95% after appeals, while ACA Marketplace plans show lower rates around 80%. DrCatalyst
Use this data. If one payer has a 20% denial rate for a procedure you commonly bill, that tells you to frontload your documentation more heavily on that payer — before you submit, not after the denial lands.
What Is NOT Live Yet in 2026 — The API Requirement
The rule also requires payers to stand up four FHIR APIs — Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization — but those compliance dates got pushed from January 2026 to January 2027. So the electronic prior authorization infrastructure is coming, just not live yet for most payers. billrMD
CMS also released a new proposed rule in April 2026 expanding prior authorization reform to drugs covered under medical benefits, with comments due June 15, 2026. This is not an incremental change — it reflects a shift in how CMS is approaching prior authorization, moving from burden reduction to system redesign. Caplinehealthcaremanagement
The direction is clear: prior authorization is moving toward fully electronic, faster, and more transparent processing. Practices that build their workflows around that future now will be ahead of every compliance deadline.
Which Services Require Prior Authorization in 2026?
Prior authorization requirements are set by each individual payer and plan — not by any single government rule. This is what makes them so difficult to manage. The list is not standardized, and it changes frequently without direct notification to providers.
The categories below represent the most commonly affected service types in 2026:
Imaging and Diagnostics MRI, CT scans, PET scans, and advanced ultrasound almost universally require prior auth from commercial payers. Even some X-rays ordered by specialists may trigger auth requirements depending on the plan.
Surgical Procedures Most elective surgeries — orthopedic, bariatric, cardiac, spinal — require prior authorization. Arthroscopic knee and shoulder procedures are among the most commonly denied in the orthopedic category.
Specialty Medications and Infusions Biologics, chemotherapy agents administered in office, and specialty infusion drugs are heavily auth-dependent. Specialty drug costs are rising fast — U.S. spending may hit $420 billion by 2025 — and to manage this, insurers now require stronger proof before approving these drugs. They might ask patients to try cheaper options first or show more clinical evidence. MedCare MSO
Mental Health and Behavioral Health Authorization for ongoing mental health services — particularly for session counts beyond initial visits — has become one of the most contested areas of prior auth in 2026. Our mental health billing services include full prior authorization support for behavioral health providers navigating payer-specific session limits.
Durable Medical Equipment CMS updated its Master List of DMEPOS items in January 2026, adding 18 HCPCS codes effective April 13, 2026. The Required Prior Authorization List also added seven HCPCS codes including certain orthoses and pneumatic compression device items — prior authorization as a condition of payment began nationwide April 13, 2026 for these newly added codes. MBW RCM
Home Health and Skilled Nursing Post-acute care authorizations are among the most complex — with payers requiring clinical documentation showing functional decline, skilled need, and homebound status, often updated every 30 to 60 days to maintain authorization.
The Step-by-Step Prior Authorization Process
Understanding the workflow end to end is the first step to making it faster and more reliable.
Step 1 — Identify at the Point of Scheduling
Authorization review should happen before the appointment is confirmed — not the morning of the procedure. When a service is scheduled, your team should immediately check whether the patient’s specific plan requires auth for that specific procedure code. Generic eligibility verification is not enough here. You need procedure-level, plan-level lookup.
Step 2 — Gather Clinical Documentation Upfront
Every prior auth request needs clinical support. Gathering this reactively — after the request is submitted and the payer asks for it — adds days to the timeline. Request the relevant clinical notes, lab results, imaging reports, and physician documentation before submitting the auth request.
Common required documents include:
- Office visit notes establishing the clinical indication
- Results of conservative treatment that has already been tried (step therapy documentation)
- Physician letter of medical necessity
- Relevant lab or imaging findings
- Patient history supporting the diagnosis
Step 3 — Submit Through the Correct Channel
Each payer has a preferred submission method — portal, fax, phone, or clearinghouse. New rules require electronic prior approvals for some insurers by 2026, and many are moving to digital systems. Providers using only fax or phone face more claim denials. MedCare MSO
Check each payer’s current submission preference before sending. A fax sent to a payer that now requires portal submission may sit unreviewed.
Step 4 — Track Every Request Actively
Submitting and waiting is not a workflow. It is a revenue leak. Under the new 7-day standard timeline, your team needs active follow-up built in — not a once-a-week check to see what came back.
Track every open auth request in a dedicated log with:
- Date submitted
- Payer and plan
- Procedure code
- Tracking or reference number
- Follow-up due date (Day 4 for standard, Hour 24 for urgent)
- Current status
Our prior authorization services maintain active tracking for every open request across every payer for the practices we manage — with escalation workflows triggered automatically when payer response windows are approaching.
Step 5 — Confirm the Authorization Before the Service Date
A verbal auth approval is not sufficient. Get the authorization number in writing — from the payer portal or via written correspondence — and document it in the patient’s chart before the service is provided. An authorization number that cannot be produced when the claim is submitted is the same as no authorization at all.
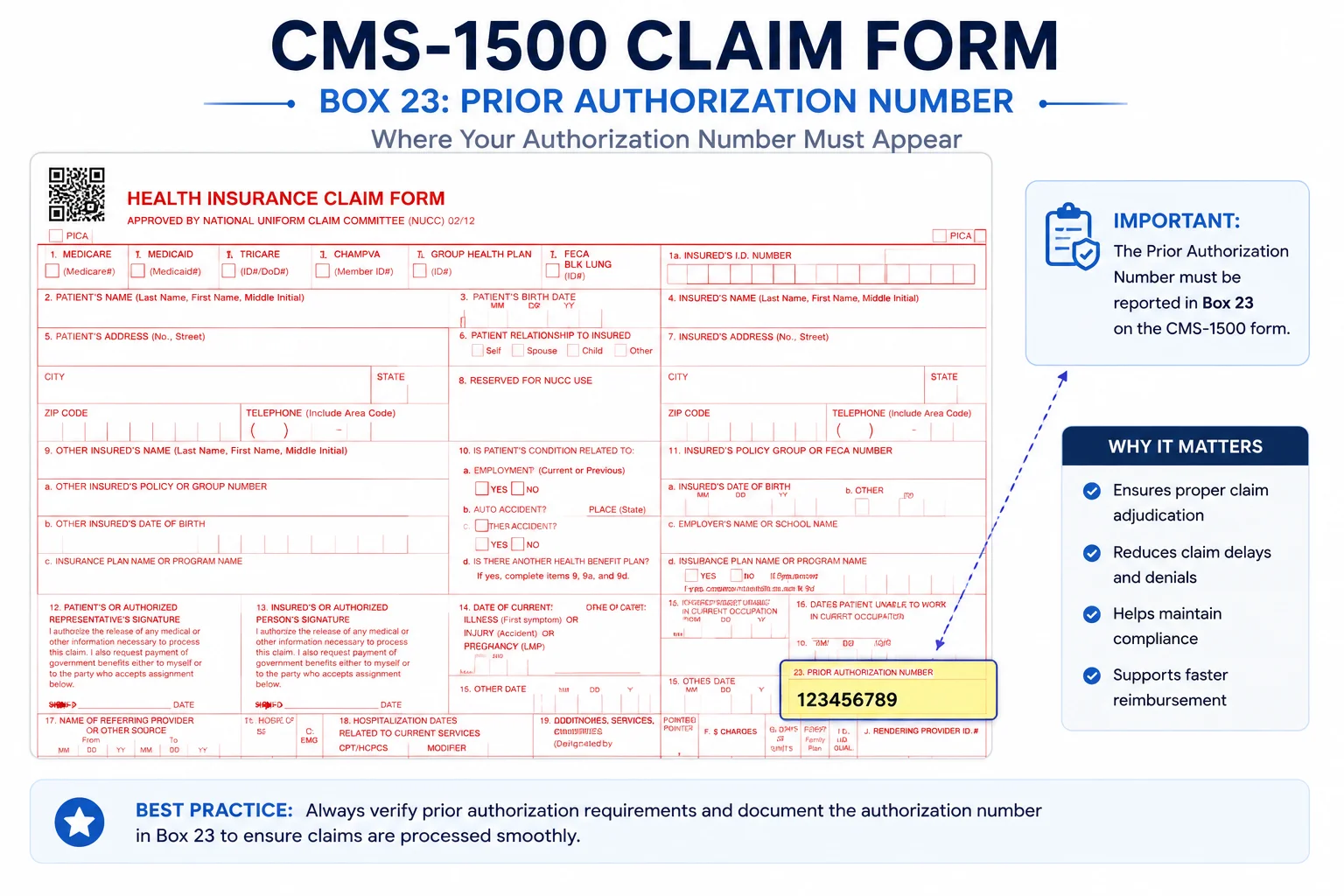
Step 6 — Link the Authorization Number to the Claim
When the claim is submitted, the authorization number must be included in the correct field (Box 23 on the CMS-1500 form). A claim submitted without the auth number — even when the auth was legitimately obtained — will be denied for missing authorization.
This is one of the most common prior auth-related denial types we see when auditing new client accounts. The auth was there. The claim submission just did not include it.
Why Prior Authorization Denials Happen — And How to Prevent Each One
KFF reported that Medicare Advantage insurers made 52.8 million prior authorization determinations in 2024, denying 4.1 million — a 7.7% denial rate that translates directly into delayed patient care and lost practice revenue. Only 11.5% of denied requests were appealed, but when appeals were filed, 80.7% were overturned. Caplinehealthcaremanagement
Read that last number carefully. When practices actually appeal a prior auth denial, they win more than 80% of the time. The problem is not that payers are right — it is that practices do not appeal.
Here are the most common denial reasons and how to prevent them:
Denial: Service not covered under the patient’s plan Prevention: Verify plan-level coverage — not just general eligibility — before scheduling. Coverage for specific services varies even within the same insurance company across different plan types.
Denial: Not medically necessary Prevention: Submit stronger clinical documentation upfront. A letter of medical necessity from the physician — specific to the diagnosis and the procedure requested — dramatically reduces medical necessity denials.
Denial: Step therapy not satisfied Prevention: Document all prior conservative treatments in the auth request. If the patient tried physical therapy for six weeks before the MRI was ordered, include that documentation. Payers deny step therapy denials when this history is not provided.
Denial: Authorization submitted after the service Prevention: Implement a scheduling checkpoint — no service is confirmed without verifying whether auth is needed. No exceptions.
Denial: Authorization number missing on the claim Prevention: Build auth number verification into your claims scrubbing checklist. Every claim for a service requiring auth must include the auth number before it goes out.
Denial: Wrong procedure code on auth vs. claim Prevention: Verify that the exact CPT code on the authorization matches the CPT code being billed. A code submitted with modifier -LT that was authorized without the modifier creates a mismatch.
Prior Authorization and Your Revenue Cycle — The Connection That Costs the Most
Prior authorization does not live in isolation. It sits at the beginning of your revenue cycle management process — and every failure in the auth workflow creates downstream billing problems that cost far more than the denied claim itself.
Consider what happens when an auth is missed:
- Service is provided
- Claim is submitted without authorization
- Payer denies — “prior authorization required”
- Biller reviews the denial — realizes auth was never obtained
- Retrospective auth request submitted — most payers deny retroactive requests
- Appeal filed — requires physician time, clinical documentation, formal letter
- Appeal outcome: 50/50 at best for a retrospective auth failure
- If denied: claim is written off — revenue permanently lost
That single missed authorization can cost your practice the entire reimbursement for the service — plus the administrative cost of multiple staff hours trying to recover it.
Now multiply that by the number of auth-required services your practice provides each week. The revenue at stake is significant.
Our creative collection solutions team handles retroactive auth appeals and denial recovery for practices that have accumulated prior auth-related denials — but our strongest recommendation is always to build a workflow that prevents them from happening in the first place.
Prior Authorization by Specialty: What Your Team Needs to Know
Prior auth burden varies significantly by specialty. Here is what the most commonly affected specialty types face in 2026:
Mental Health and Behavioral Health Session-based authorization is one of the most administratively burdensome areas of prior auth. Payers often authorize 8 to 12 sessions at a time, requiring reauthorization before sessions are exhausted. Missing the reauthorization window creates an unauthorized service gap. Our mental health billing specialists track session counts and reauthorization timelines for every active patient.
Cardiology Cardiac catheterization, stress testing, echocardiography, and device implants all carry high auth requirements. Cardiology is also one of the specialties most affected by Medicare Advantage prior auth volume. Visit our cardiology billing page to learn how we support cardiology practices with auth management.
Oncology Chemotherapy and infusion authorizations require clinical staging documentation, pathology reports, and treatment plan letters. Each cycle may require a separate authorization. Oncology billing demands dedicated prior auth specialists who understand cancer staging and treatment protocols.
Wound Care Advanced wound care treatments — negative pressure wound therapy, skin substitutes, hyperbaric oxygen — are heavily auth-dependent and frequently denied on first submission. Our wound care billing team manages auth for wound care practices with specific expertise in DMEPOS and advanced treatment codes.
Urology Surgical procedures including UroLift, laser prostate treatments, and cystoscopy often require auth from commercial payers. Diagnostic imaging ordered by urologists — pelvic MRI, renal ultrasound — frequently triggers auth requirements that vary widely by plan. See our urology billing services for specialty-specific support.
How to Appeal a Prior Authorization Denial — And Win
When appeals were filed for Medicare Advantage prior auth denials, 80.7% were overturned. That number tells you everything you need to know about whether appealing prior auth denials is worth the effort. It absolutely is. The problem is that only 11.5% of denials ever get appealed in the first place. Caplinehealthcaremanagement
A strong prior auth appeal includes:
A formal letter of medical necessity written by the ordering physician — specific to the patient’s diagnosis, condition severity, treatment history, and clinical rationale for the requested service. Generic letters that could apply to any patient are easy for payers to reject. Patient-specific clinical justification is much harder to deny.
Clinical guidelines support — cite the relevant clinical guideline, peer-reviewed evidence, or specialty society recommendation that supports the requested service. If the American College of Cardiology recommends echocardiography for a specific diagnostic indication and your patient meets that indication, cite it directly in the appeal.
Documentation of prior conservative treatment — show the payer what was tried before this service was requested. Step therapy denials fall apart when you can demonstrate the patient already failed the cheaper option.
Peer-to-peer review request — most payers allow the ordering physician to request a direct conversation with the payer’s medical reviewer. These calls are often the fastest path to overturning a medical necessity denial. Do not overlook this option.
Timely filing — appeals must be submitted within the payer’s appeal window, which typically ranges from 30 to 180 days from the denial date. Missing the window forfeits your right to appeal regardless of how strong your case is.
What Good Prior Authorization Management Looks Like in Practice
Here is the benchmark your practice should be working toward:
| Metric | Current Industry Average | Strong Practice Target |
|---|---|---|
| Auth-related denial rate | 7%–12% | Under 2% |
| First-pass auth approval rate | 70%–80% | Above 90% |
| Average auth turnaround time | 5–10 days | Under 5 days |
| Appeal overturn rate | 40%–50% | Above 75% |
| Retroactive auth denials | Common | Near zero |
If your practice is outside these targets, prior authorization is actively costing you revenue every week.
Common Questions About Prior Authorization
What happens if we provide a service without getting prior authorization?
In most cases, the claim will be denied and the denial will not be overturnable on appeal — because the issue is not clinical, it is procedural. Retrospective authorization requests are denied by most payers. The service may need to be written off entirely or billed to the patient, which creates patient satisfaction problems and potential billing compliance issues.
How do we know which services require prior authorization for each payer?
Each payer maintains an authorization requirement list on their provider portal. The problem is these lists change, often without direct notification. The most reliable approach is to run a procedure-level, plan-level check at the time of scheduling for every service — not just the ones you assume require auth. Our billing team maintains updated auth requirement lists for every payer our clients bill.
Can we bill the patient if insurance denies because authorization was not obtained?
Generally no — and attempting to do so can violate your payer contract. Most commercial payer contracts prohibit billing patients for services denied due to provider-side administrative errors, which includes failure to obtain required authorization. Check your specific payer contracts with a healthcare attorney if you are unsure.
How does the new 7-day decision window affect our scheduling?
It should tighten your scheduling window. If you are scheduling procedures 2 to 3 days out and the auth has not been confirmed, you are taking on risk. For elective procedures, build a minimum of 5 to 7 days between auth submission and procedure scheduling so you have a confirmed approval in hand before the appointment is set.
What is gold carding and does it affect our practice?
Gold carding is a program where payers waive prior authorization requirements for providers who have demonstrated a high approval rate — meaning the payer trusts that the provider’s orders are consistently medically appropriate. Several states have now passed gold carding laws requiring payers to offer this. If your practice has a strong clinical and auth approval track record, it may be worth requesting gold card status directly from payers you frequently work with.