Physician Credentialing Timeline 2026 | How Long It Really Takes (And Why Delays Are Costing Practices a Fortune)
Here is a scenario that plays out in practices every single week across the United States:
A new physician joins your team. She is licensed, trained, experienced, and ready to see patients on day one. Your schedule is full. Your patients are waiting. But weeks pass — then months — and she still cannot bill a single insurance claim. Not because anything is wrong with her credentials. But because the credentialing paperwork is stuck somewhere in a payer’s queue.
Meanwhile, your practice is paying her salary. Your patients are being seen. But zero dollars are coming in for her work.
That is what an unmanaged credentialing timeline costs. And in 2026, with stricter rules, tighter windows, and more documentation requirements than ever before, the stakes have never been higher.
This guide walks you through exactly how long physician credentialing takes in 2026, what has changed this year, what causes delays, and — most importantly — how to protect your practice revenue while the process runs.
What Is Physician Credentialing and Why Does It Control Your Revenue?
Physician credentialing is the formal process by which insurance payers — Medicare, Medicaid, and commercial insurers — verify that a provider is qualified, licensed, and eligible to be reimbursed for patient care within their network.
Until that process is complete, your provider cannot bill. Until your provider cannot bill, your practice cannot collect. It is that direct.
According to healthcare industry data, nearly 40% of providers experience delayed reimbursements because of credentialing issues, and practices lose an estimated $7,000 to $12,000 per provider each month during enrollment delays. MedCare MSO
One in five hospitals that can quantify the impact report losing more than $1 million annually from credentialing delays alone. And 69% of health systems and provider groups report losing $1,000 to $5,000 per provider per day due to payer enrollment delays. OmniMD
Those numbers are not outliers. They are what happens when credentialing is treated as a back-office task instead of a revenue-critical process.
Our physician credentialing services are built around one goal: getting your providers credentialed as fast as possible, with zero gaps, and zero billing disruptions.
How Long Does Physician Credentialing Actually Take in 2026?
Provider credentialing in 2026 typically takes between 60 to 180 days, depending on the insurance payer, provider specialty, state regulations, and document accuracy. MedCare MSO
That is a wide range — and it is intentional. The honest answer is that no two credentialing timelines are identical. Here is how it breaks down by payer type:
Medicare (PECOS): 60 to 90 days when the application is complete and accurate. Errors or missing documents can push this past 120 days.
Medicaid: 45 to 90 days on average, though state-by-state variation is significant. Some state Medicaid programs run faster; others are notoriously slow.
Commercial Payers (Blue Cross, Aetna, United, Cigna): 90 to 150 days. These payers have their own internal committee review cycles — often monthly — and a missed committee meeting can add 30 days overnight.
Medicare Advantage Plans: These are credentialed separately from traditional Medicare and often take as long as commercial payers — 90 to 150 days — with each plan having its own process.
Telehealth Credentialing: Telehealth credentialing timelines usually range between 90 to 150 days, often longer because providers may require multi-state licenses and separate payer enrollments for multiple states. MedCare MSO
The practical rule: Start credentialing 120 days before a provider’s intended start date — not 60 days, not 30 days. 120 days. That buffer is not conservative; it is necessary. Medsolercm
What Has Changed in 2026? The NCQA and CMS Updates You Must Know
2026 brought the most significant credentialing rule changes in over a decade. If your practice has not updated its credentialing workflows to reflect these changes, you are already behind — and you may not know it yet.
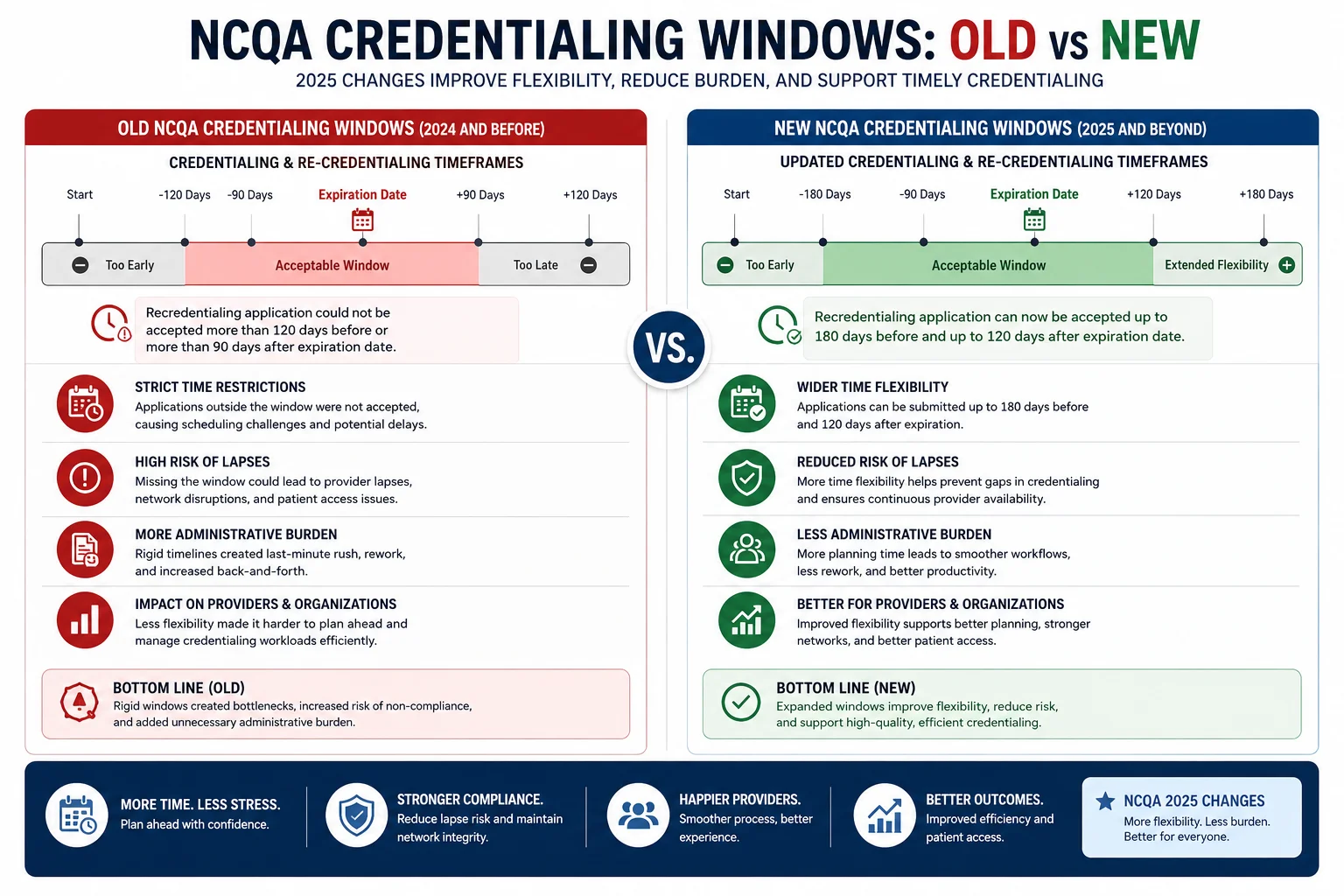
NCQA Shortened Verification Windows — Dramatically
NCQA reduced credentialing windows from 180 to 120 days for accredited organizations and from 120 to 90 days for certified organizations. That is a 33% reduction in available credentialing time, while verification requirements have actually increased. prohealthcareadvisors
Read that again: less time, more requirements. Organizations undergoing their 2026 review cycles are failing surveys due to these new requirements. This is not a theoretical risk — it is happening right now. DrCatalyst
Monthly Monitoring Is Now Mandatory
NCQA now requires healthcare organizations to verify provider credentials every 30 days instead of the previous 6-month cycle. This applies to all credentialing files processed after July 1, 2025. Missing a single monthly check can mean practicing with an expired credential — a compliance violation that creates liability and billing risk. MBW RCM
This change alone has forced many practices to completely rethink how they track and manage provider files. Manual spreadsheets cannot keep up with a 30-day monitoring cycle across multiple providers and payers.
CAQH Re-Attestation Is Now Every 120 Days
In 2026, CAQH ProView re-attestation is required every 120 days. Missing a re-attestation window causes a provider’s CAQH profile to lapse — which in turn delays or blocks any new credentialing applications that depend on it as a primary data source. BillFlash
CMS Moved to Digital-First Processes
CMS is advancing digital transformation through cloud-based credentialing systems that enable real-time data entry, automatic updates, and faster communication between providers and payers. Paper-based systems now create compliance risks. After March 1, 2026, CMS stopped mailing paper CLIA fee coupons entirely — a signal of where the entire process is heading. prohealthcareadvisors
Stricter Risk-Level Documentation for Medicare and Medicaid
Accurate risk-level documentation is now required for both Medicare and Medicaid to prevent enrollment delays. Providers classified under higher-risk screening levels face additional verification steps that can extend timelines significantly. Prgmd
The 8-Step Physician Credentialing Process in 2026
Understanding the full sequence helps you see exactly where delays happen — and how to prevent them.
Step 1 — Establish or Update the CAQH ProView Profile
Everything starts here. Over 2.5 million providers use CAQH ProView, and most major health plans accept it as their primary data source. The provider’s CAQH profile must be complete, fully attested, and authorized before any application is submitted. BillFlash
An incomplete or lapsed CAQH profile blocks everything downstream. Check it first, every time.
Step 2 — Gather the Full Documentation Package
Missing even one document creates delays that can cost providers thousands in lost revenue. The standard documentation package includes: current state medical license, DEA certificate, board certification (if applicable), malpractice insurance certificates with history of claims, NPI numbers (individual and group), hospital privileges documentation, CV with no unexplained gaps, and education and training verification. prohealthcareadvisors
Every gap in your CV — even a few weeks between positions — will be questioned by payers. Document everything in advance.
Step 3 — Submit Applications to Each Payer
Applications go to each payer separately, as each has its own enrollment process, portal, and requirements. Our team at Pro Health Care Advisors maintains direct working relationships with major payers, which allows us to submit applications correctly the first time and track them actively from day one.
Step 4 — Primary Source Verification (PSV)
Each payer independently verifies your provider’s credentials directly from the original sources — not from documents you submitted. They contact the medical school, training programs, licensing boards, and malpractice carriers directly. This step is largely outside your control — but delays happen when submitted information does not exactly match what primary sources report. Even small discrepancies, like a middle name shortened or a graduation date off by one month, create back-and-forth that adds weeks to the timeline. Medsolercm
This is why accuracy in Step 2 is so critical. Every error here costs days.
Step 5 — Payer Committee Review
The final step before a provider can bill involves internal committee review at each payer, which may only happen once a month. If your application misses this month’s committee meeting — even by one day — you wait another 30 days for the next one. Active follow-up to confirm your application is on the agenda is not optional; it is essential. Medsolercm
Step 6 — Receive the Effective Date
Upon approval, the payer issues an effective date — the date from which claims can be submitted. This date matters enormously. Claims submitted for dates of service before the effective date will be denied, even if the provider was already seeing patients.
Step 7 — Set Up EFT and ERA
Once credentialed, Electronic Fund Transfer and Electronic Remittance Advice must be set up with each payer. Our Electronic Fund Transfer services handle this automatically, ensuring the first payment hits your account without delay.
Step 8 — Begin Monthly Monitoring
NCQA now requires organizations to monitor provider credentials every 30 days for license expirations, OIG exclusions, medical board actions, and SAM.gov screening. This is not a one-time setup task — it is an ongoing operational responsibility. Our credentialing team handles monthly monitoring for all providers we credential, so nothing slips through the cracks. MBW RCM
The 9 Most Common Reasons Credentialing Gets Delayed
Most credentialing delays are preventable. Here are the ones we see most often:
- Incomplete CAQH profile — Unattempted fields or lapsed re-attestation block applications before they even start
- Gaps in the CV — Any unexplained gap in work history triggers a verification request, which can add weeks
- Malpractice history not fully documented — Incomplete claims history is one of the top reasons payers send back applications
- Wrong NPI or taxonomy code — A single digit error here creates a denial chain that is frustrating and time-consuming to unwind
- Missing hospital privileges documentation — Required by most commercial payers even if the provider never admits patients
- DEA certificate not current — An expired DEA delays credentialing across every payer simultaneously
- Starting the process too late — Beginning credentialing 30 to 60 days before a provider’s start date virtually guarantees a billing gap
- Not following up actively — Payers do not chase you when something is missing; they simply wait for you to ask
- Multi-location enrollment not updated — When a practice adds a location or telehealth as a service site, the enrollment update requirement multiplies across every payer — and the failure rate for multi-location enrollment updates is 34% higher than single-location updates. Dr. Credentialing
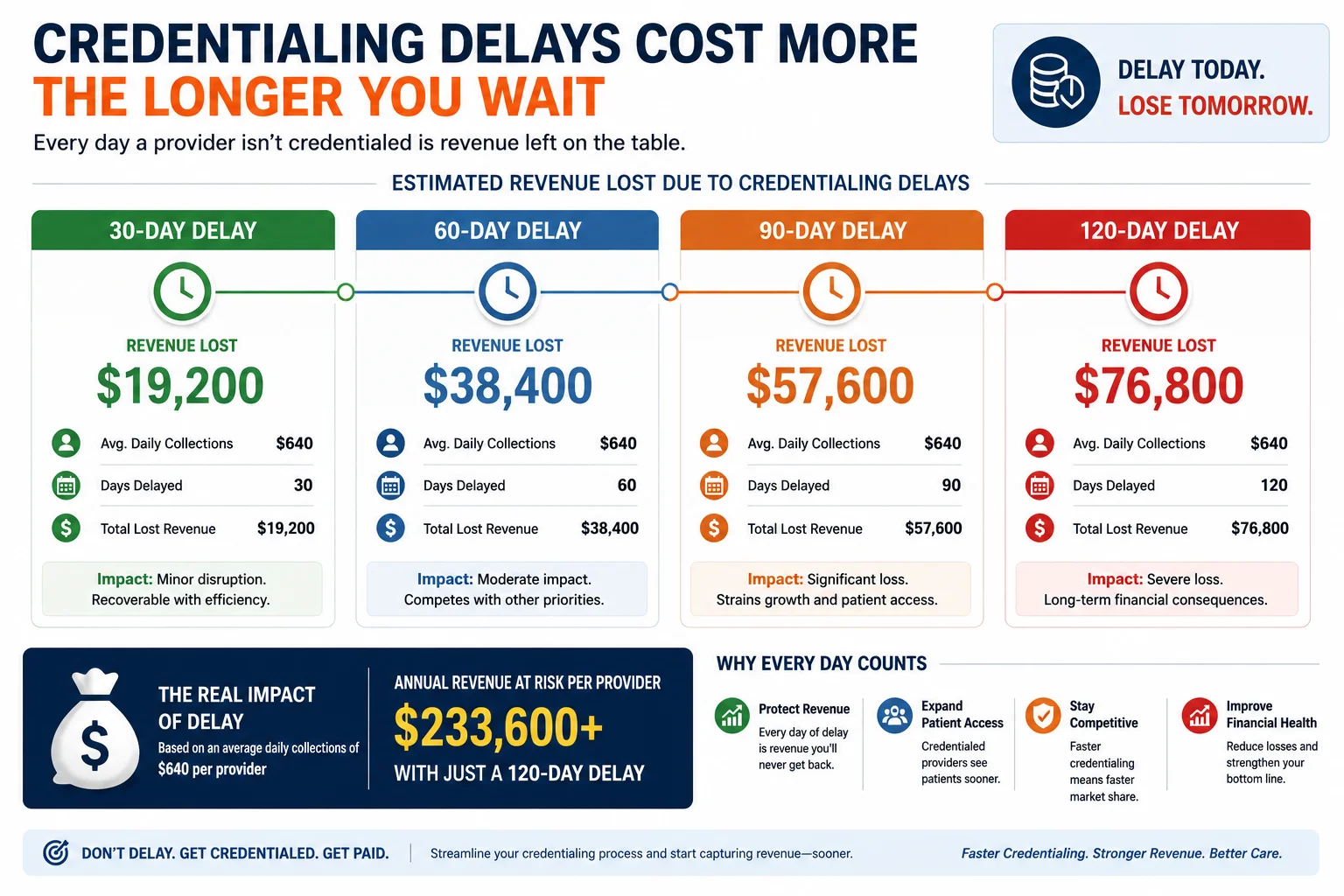
What a Credentialing Delay Actually Costs Your Practice
Let’s stop talking in abstract terms and look at real numbers.
Research from the credentialing industry shows that physicians contribute an average of $200,000 to $300,000 in revenue per month to a practice. Every month of credentialing delay is a month of that revenue either lost or delayed. For a small practice bringing on a new provider at $250,000 per month in revenue contribution, a 4-month credentialing delay instead of a 2-month delay costs approximately $500,000 in unrealized revenue. Medsolercm
A physician earning $2,000 a day in charges delayed for just two months costs the practice $120,000 in gross revenue. A practice in Florida reported a loss of $400,000 in revenues because of a five-month delay in the credentialing process for two physicians. Billmate
Delays in credentialing directly delay revenue, often creating $135,000 to $900,000 or more in deferred billings over 90 to 120 days, depending on specialty and volume. billrMD
These numbers explain why experienced practice managers treat credentialing as a revenue strategy — not a paperwork chore.
Re-Credentialing: What Happens After Initial Approval
Getting credentialed is not a one-time event. Providers must be re-credentialed every 36 months, unless the payer indicates otherwise. Re-credentialing includes verification of licensure, malpractice coverage, sanctions, and professional references. Prgmd
According to a 2026 analysis across 190 specialty practices, 61% of practices experience at least one active credentialing lapse at any given time, and 78% of those lapses go undetected for 60 or more days. Dr. Credentialing
An undetected credentialing lapse means your provider is seeing patients and submitting claims — but those claims are being silently denied because the payer’s records show an expired enrollment. By the time someone notices, there may be 60 or 90 days of claims to rework or appeal.
Credentialing lapses result in revenue losses of $18,000 to $95,000 per affected provider annually. Dr. Credentialing
Our physician credentialing team proactively tracks every re-credentialing deadline for every provider we manage — sending alerts 90, 60, and 30 days before expiration so you are never caught off guard.
Credentialing and Your Revenue Cycle: The Connection Most Practices Miss
Credentialing is not just an HR or compliance function. It is the foundation of your entire revenue cycle management operation.
A provider who is not credentialed cannot generate billable claims. A provider whose enrollment has lapsed generates claims that get denied. A provider credentialed at the wrong location generates claims that get rejected. Every credentialing gap creates a downstream billing problem.
This is why we integrate credentialing management directly with medical billing and practice management at Pro Health Care Advisors. When credentialing and billing are handled by the same team, nothing falls between the cracks. Effective dates flow directly into billing activation. Payer enrollment numbers get loaded correctly. Monthly monitoring protects the claims you are already submitting today.
For practices that also need prior authorization services, credentialing status directly affects which authorizations can be requested — another reason the two functions need to be managed together.
Common Questions About Physician Credentialing in 2026
Can a provider see patients before credentialing is complete?
Yes — but they cannot be reimbursed by insurance for those visits until they have an effective date from each payer. Some practices choose to hold claims and submit them once the effective date is received. This is allowable for most payers, but the rules vary. Talk to your billing team before making this decision.
What is the difference between credentialing and payer enrollment?
Credentialing is the verification of a provider’s qualifications. Payer enrollment is the administrative process of getting that provider added to a payer’s network. The two happen together but are technically separate steps — and both are required before billing can begin.
What happens if a provider’s license lapses during credentialing?
The entire application stops. Most payers will not continue processing until the license is renewed and verified. This is one of the most expensive and preventable delays in credentialing — and one of the main reasons monthly monitoring matters so much.
How many payers should a new provider be credentialed with?
At minimum: Medicare, Medicaid (state), and the top 3 to 5 commercial payers by patient volume in your area. Most practices credential with 8 to 15 payers per provider. Each requires a separate application and timeline.
Can credentialing be done faster?
Yes — with the right preparation. In-house credentialing requires 40 to 60 hours of administrative time per provider for 10 to 15 payers, plus expertise in each payer’s specific submission requirements and consistent weekly follow-up calls. Most practices find outsourcing more cost-effective once they calculate the true staff cost plus the revenue lost during longer timelines. OneMed Billing
How Pro Health Care Advisors Handles Credentialing Differently
Most credentialing services submit your application and wait. We do not work that way.
From the moment we take on a credentialing file, we are actively in contact with payers — tracking application status, confirming committee meeting schedules, resolving discrepancies before they cause delays, and documenting every step so there is never a question about where something stands.
Here is what our credentialing service includes:
- Complete CAQH ProView setup, completion, and re-attestation management
- Primary source verification coordination
- Applications submitted to Medicare, Medicaid, and all major commercial payers
- Active follow-up with every payer on a weekly basis
- Effective date tracking and billing team notification
- EFT and ERA setup coordination
- Monthly monitoring for license, DEA, OIG, SAM.gov, and board sanctions
- Re-credentialing management with 90-day advance alerts
We also handle HIPAA-compliant data management throughout the entire credentialing process — because the documents involved contain highly sensitive provider and patient information that must be protected at every stage.