How Long Does Physician Credentialing Take? State by State Guide for 2026
If you are asking how long physician credentialing takes in 2026, you have probably already realized that the standard answer — “90 to 120 days” — is not actually helpful.
Because the real answer depends on which state you are in, which payers you are enrolling with, which specialty the provider practices, and how complete and accurate your application is on the first submission.
Here is what the data actually shows: nearly 40 percent of providers experience delayed reimbursements because of credentialing issues. Practices lose an estimated $7,000 to $12,000 per provider per month during enrollment delays. And for a practice bringing on a new physician generating $250,000 per month in revenue, a four-month credentialing delay instead of a two-month delay represents $500,000 in unrealized revenue.
That is why understanding real credentialing timelines — not the optimistic estimates payers put on their websites — is one of the most financially important things a practice manager can do in 2026.
This guide covers real credentialing timelines by payer type, real timelines by state, what changed in 2026 that is affecting those timelines, the nine most common delays and how to avoid each one, and exactly when your practice needs to start the process for a new provider.
The Real Credentialing Timeline Range in 2026
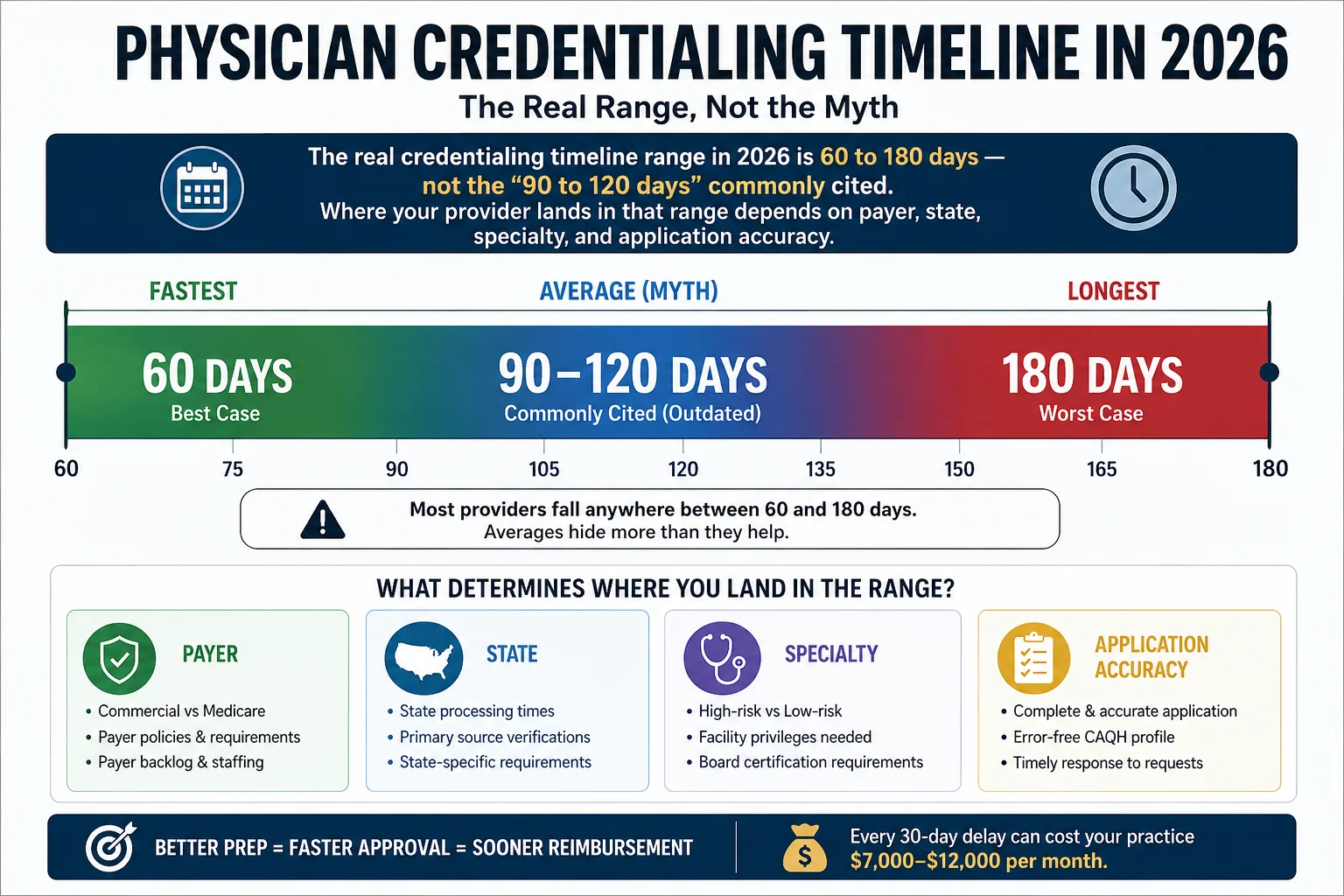
According to data from credentialing specialists and payer-reported processing times, the realistic range for physician credentialing in 2026 is 60 to 180 days — and that range has gotten wider, not narrower, as payers have added new verification requirements.
Here is why the range is so wide:
On the fast end, a primary care physician with a clean application, a complete and attested CAQH profile, no work history gaps, no malpractice history, and no prior sanctions can move through Medicare enrollment in 45 to 60 days and commercial payer credentialing in 60 to 75 days with some payers offering fast-track processing.
On the slow end, a specialist with multi-state license history, a work history gap that requires explanation, an outdated CAQH profile, and applications submitted to multiple payers sequentially rather than simultaneously can easily reach 150 to 180 days — and some states routinely exceed that.
According to Verisys’s credentialing timeline analysis, initial credentialing typically involves three phases: preparation (2 to 4 weeks), application review (60 to 120 days), and final enrollment (2 to 4 weeks). The application review phase is where most delays occur — and it is the phase most susceptible to the preventable errors covered later in this guide.
The critical implication: start credentialing 120 days before a provider’s intended start date — minimum. Starting 60 days before almost guarantees a gap where the provider is seeing patients they cannot bill for.
Physician Credentialing Timelines by Payer Type
Medicare — 30 to 90 Days (PECOS Electronic Submissions)
Medicare enrollment through PECOS — the Provider Enrollment, Chain, and Ownership System — is typically the fastest federal enrollment when done correctly.
For a clean electronic application with no errors or missing documentation, Medicare enrollment averages 30 to 60 days through PECOS. Paper applications take significantly longer — up to 120 days — and there is almost no legitimate reason to submit a paper Medicare application in 2026.
According to Medwave’s credentialing timeline guide, Medicare enrollment typically runs 60 to 90 days and requires meticulous attention to detail, as CMS rejects applications for even minor errors.
Important 2026 changes affecting Medicare timelines:
CMS updated its enrollment standards effective January 2026, adding enhanced primary source verification requirements. Enhanced fingerprint-based background checks now apply to higher-risk provider categories. And CMS reduced the revalidation cycle from five years to three years for certain specialties — meaning existing providers need to revalidate more frequently than before.
One critical detail that trips up new practices: Medicare’s effective date is the later of the date the application is filed or the date the provider meets all enrollment requirements. If documentation is submitted incomplete and corrected weeks later, the effective date shifts accordingly — affecting how far back claims can be submitted.
Medicare revalidation timeline: Providers who miss their revalidation notice face deactivation, and reactivation takes 60 to 90 days. Set calendar reminders 6 months before revalidation due dates — do not rely on CMS mail reaching the right person at your practice.
Medicaid — 45 to 150 Days (Highly Variable by State)
Medicaid credentialing is the most unpredictable part of the entire enrollment process. Federal rules require states to process applications within 45 to 90 days — but many states consistently miss that standard, and some Medicaid managed care organization enrollments run even longer.
The variability comes from three sources: state-specific documentation requirements, the presence or absence of Medicaid managed care organizations (MCOs) that require separate enrollment from the state, and the simple reality that some state Medicaid offices are significantly better resourced and more responsive than others.
For states with Medicaid MCO structures — including California (Medi-Cal managed care), Georgia (GAMMIS and CMOs), Florida (Medicaid MCOs), and Texas (Medicaid MCOs) — providers must often complete enrollment at both the state level and separately with each individual managed care organization. The state enrollment and the MCO enrollment must both be active before billing can begin, which effectively extends the total Medicaid credentialing timeline.
Key rule: Submit Medicaid applications at the same time as Medicare and commercial payers — not after. Medicaid is often the slowest part of the entire credentialing process, and sequential rather than parallel submission adds months to the total timeline.
Commercial Payers — 60 to 150 Days (By Payer)
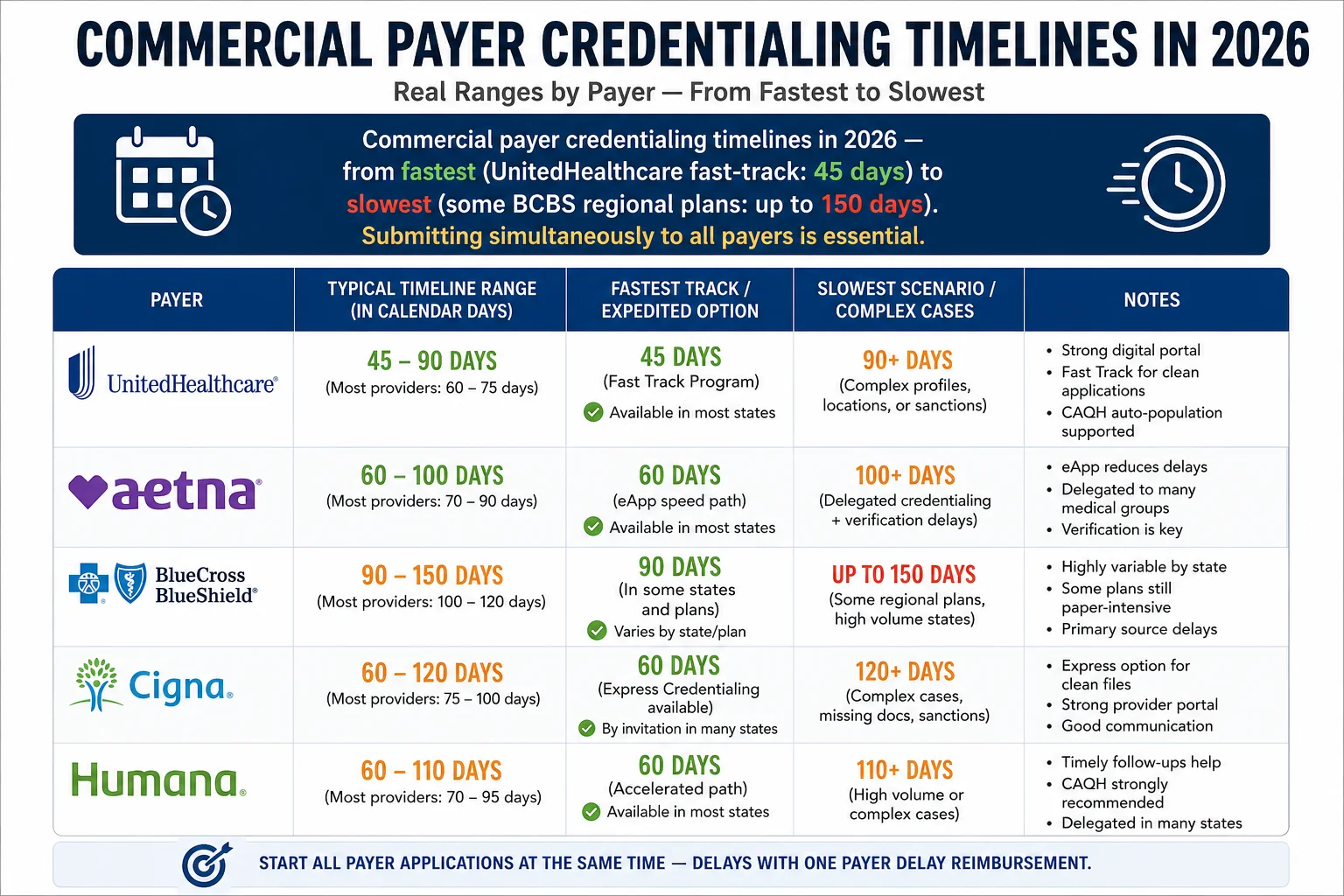
Commercial payers have their own credentialing applications, portals, document requirements, and internal review processes. Here are the realistic timelines for major commercial payers in 2026:
| Payer | Standard Timeline | Fast-Track Available? | Notes |
|---|---|---|---|
| UnitedHealthcare | 60–90 days | Yes — 45 days for PCPs in underserved areas | Fastest major commercial payer in 2026 |
| Aetna | 60–90 days | Limited | Clean applications process toward lower end |
| Cigna | 60–90 days | No | Expanded sanctions screening in 2026 |
| Humana | 60–90 days | Limited | Medicare Advantage enrollment separate |
| Blue Cross Blue Shield | 90–120 days | Yes — behavioral health fast-track in some states | Varies significantly by regional plan |
| Anthem | 90–120 days | No | New quality metric requirements added in 2026 |
| Molina Healthcare | 60–90 days | No | Medicaid MCO focus |
| Centene / WellCare | 60–90 days | No | Medicaid MCO focus |
According to MBW RCM’s credentialing analysis, some insurance companies adapted quickly to 2026 requirements and maintain 60 to 75 day timelines. Others are struggling with the additional verification workload and running 120 to 150 days. Before submitting applications, research current processing times for your priority payers.
The most important rule for commercial credentialing: Submit to all payers simultaneously — never sequentially. Every payer you submit to on the same day is 60 to 120 days closer to active enrollment than if you wait for one to finish before starting the next.
Physician Credentialing Timelines by State — 2026
This is the section most practice managers need and rarely find. Here are real credentialing timelines by state based on 2026 data:
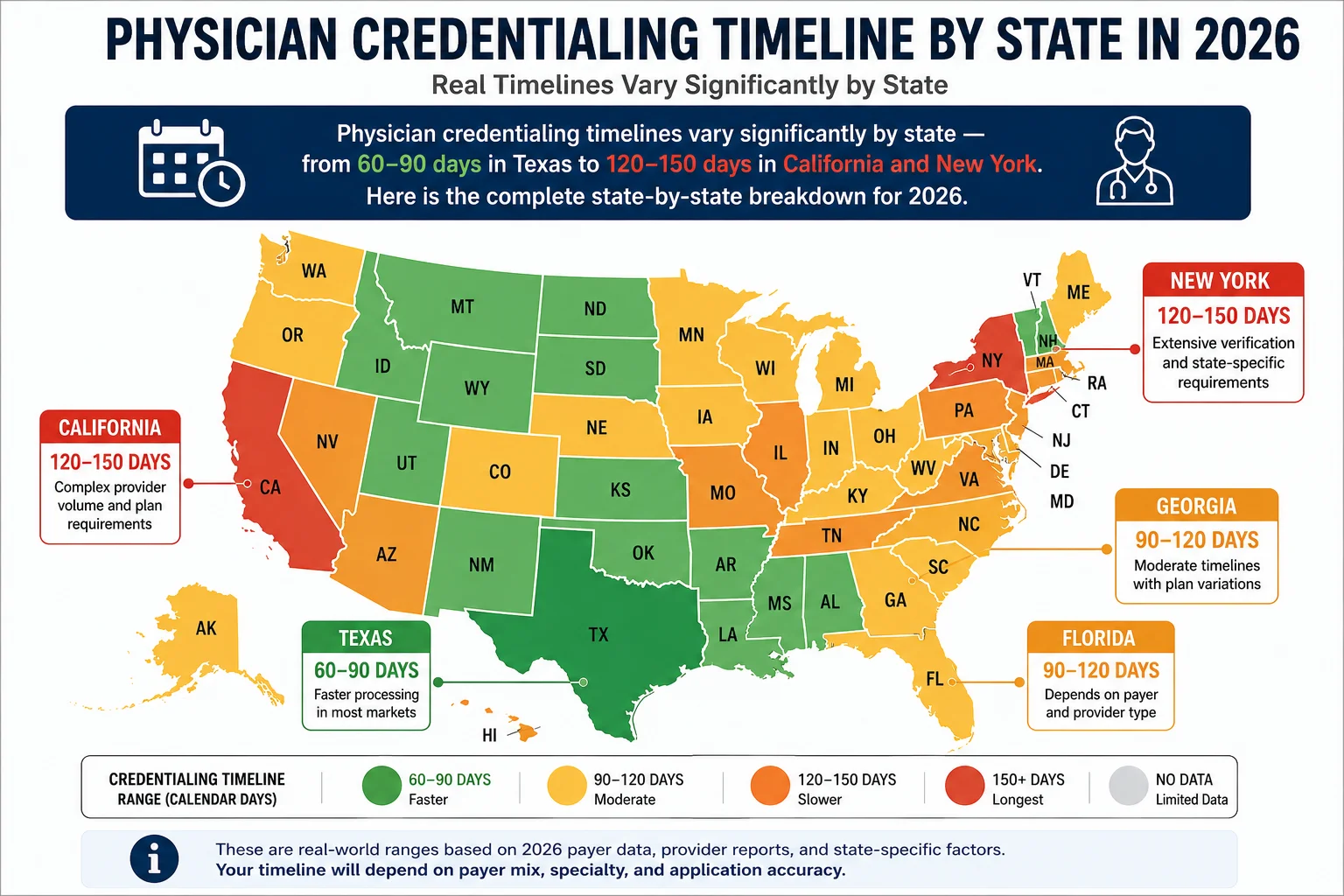
California — 120 to 150 Days
California has among the longest credentialing timelines in the country. According to data from TheCredentialing’s physician timeline analysis, the time required for physician credentialing in California is 120 to 150 days due to additional regulatory and payer-specific requirements.
California implemented real-time primary source verification for all new enrollments in 2026 — adding to an already complex process. Medi-Cal managed care enrollment adds another layer: providers must enroll with the state Medicaid program AND separately with each Medi-Cal managed care plan in their service area.
For California practices: Start credentialing at minimum 150 days before a new provider’s intended billing start date.
New York — 120 to 150 Days
New York consistently has some of the longest processing times in the country, driven by strict verification requirements, high provider volume, and a complex commercial payer landscape in the New York City metro area.
According to industry data, New York credentialing typically takes 120 to 150 days due to strict verification requirements and high provider volume. The New York Department of Health’s Medicaid enrollment process is particularly demanding, often requiring additional documentation steps not required in other states.
For New York practices: Budget 150 days minimum for new provider credentialing. For behavioral health providers, BCBS of New York offers a fast-track option due to high demand — check eligibility before standard submission.
Texas — 60 to 90 Days
Texas generally processes commercial payer credentialing faster than most states. According to credentialing timeline data, Texas often experiences shorter credentialing timelines, averaging 60 to 90 days for many commercial payers.
However, Texas Medicaid — which runs through managed care organizations including Molina Healthcare of Texas, UnitedHealthcare Community Plan, and BCBS of Texas — requires enrollment with each individual MCO in addition to state-level enrollment. This MCO enrollment layer adds 30 to 60 days to the total Medicaid credentialing timeline.
Texas also processes applications within 180 days under HMO requirements — which means while commercial credentialing moves faster, HMO-specific applications can still run long if documentation is incomplete.
For Texas practices: Commercial credentialing can complete in 60 to 90 days with complete documentation. Budget 120 days total to account for Medicaid MCO enrollment.
Florida — 90 to 120 Days
Florida credentialing typically takes 90 to 120 days, particularly for Medicaid managed care plans. Florida’s Medicaid program runs entirely through MCOs — including Sunshine Health, Molina Healthcare of Florida, Simply Healthcare, and UnitedHealthcare Community Plan — and each MCO enrollment is separate from state-level Medicaid enrollment.
Florida’s high Medicare Advantage penetration — over 57 percent of Florida Medicare beneficiaries are in MA plans — means providers must also credential separately with each Medicare Advantage plan they intend to participate in. This significantly increases the number of credentialing applications a new Florida provider must complete.
For Florida practices: Budget 120 to 150 days for new provider credentialing when accounting for both Medicaid MCO enrollment and Medicare Advantage plan credentialing.
Georgia — 90 to 120 Days
Georgia credentialing for commercial payers typically runs 90 to 120 days. Georgia Medicaid — which runs through Care Management Organizations including CareSource Georgia, Molina Healthcare, Amerigroup Georgia, and Peach State Health Management — requires both state-level GAMMIS enrollment and separate CMO enrollment.
A 2026 GAMMIS group enrollment update means practices with multiple rendering providers must also complete group-level enrollment. Practices that missed this update may be experiencing silent denials — claims processing but reimbursement going to the wrong entity.
For Georgia practices: Start credentialing 120 days before a new provider’s start date. Verify GAMMIS group enrollment status before submitting billing claims.
Illinois — 90 to 120 Days
Illinois credentialing timelines usually fall between 90 and 120 days, depending on payer verification procedures. Illinois Medicaid — managed through the Illinois Department of Healthcare and Family Services — has its own enrollment portal and documentation requirements separate from commercial payer credentialing.
For Illinois practices: 120-day lead time is the standard recommendation for new provider credentialing.
Other Key States — Quick Reference
| State | Typical Timeline | Key Notes |
|---|---|---|
| Pennsylvania | 90–120 days | Multi-state licensing needed for NJ/DE border areas |
| Ohio | 90–120 days | Medicaid MCO enrollment adds 30–60 days |
| Michigan | 90–120 days | BCBS Michigan has strong regional dominance — prioritize |
| Washington | 90–120 days | Apple Health (Medicaid) managed care enrollment required |
| Colorado | 60–90 days | Generally faster commercial credentialing |
| Arizona | 90–120 days | AHCCCS Medicaid managed care enrollment separate |
| Massachusetts | 120–150 days | Complex commercial payer landscape in Boston market |
| Virginia | 90–120 days | Medicaid Managed Care adds to timeline |
| North Carolina | 90–120 days | NC Medicaid transformation affects enrollment timelines |
| Tennessee | 90–120 days | TennCare managed care enrollment separate |
What Changed in 2026 That Is Affecting Credentialing Timelines
Several specific 2026 changes are making credentialing slower for practices that have not adapted:
CMS enhanced primary source verification (effective January 2026). CMS now directly verifies licenses, DEA registrations, and sanctions with issuing authorities rather than relying on self-reported data. This adds verification steps that can extend Medicare enrollment timelines by 2 to 3 weeks for providers with complex credential histories.
NCQA tightened PSV window from 180 to 120 days. The NCQA now requires credential verification organizations to complete primary source verification within 120 days — down from 180 days previously. If your data gathering is slow or contains errors, there is no longer a soft buffer window to fix it before verification data expires.
CMS data matching between NPPES and PECOS. According to credentialing specialists, if there is a data mismatch between the National Plan and Provider Enumeration System (NPPES) and the Provider Enrollment, Chain, and Ownership System (PECOS), claims will be instantly denied. This is a new automated check that was not applied at this scale in prior years.
Anthem added quality metric requirements. Anthem now factors patient satisfaction scores and outcome data into credentialing decisions — adding a new documentation requirement that most practices were not previously aware of.
UnitedHealthcare continuous monitoring. UnitedHealthcare now requires continuous license monitoring rather than periodic checks during revalidation — meaning a lapsed license discovered between revalidation cycles can trigger immediate suspension of billing privileges.
IMLC expanded to 40 states. The Interstate Medical Licensure Compact now covers 40 states plus Washington D.C. and Guam. Processing through the Compact typically takes 14 to 21 days once the letter of qualification is issued — significantly faster than individual state licensing for multi-state practices.
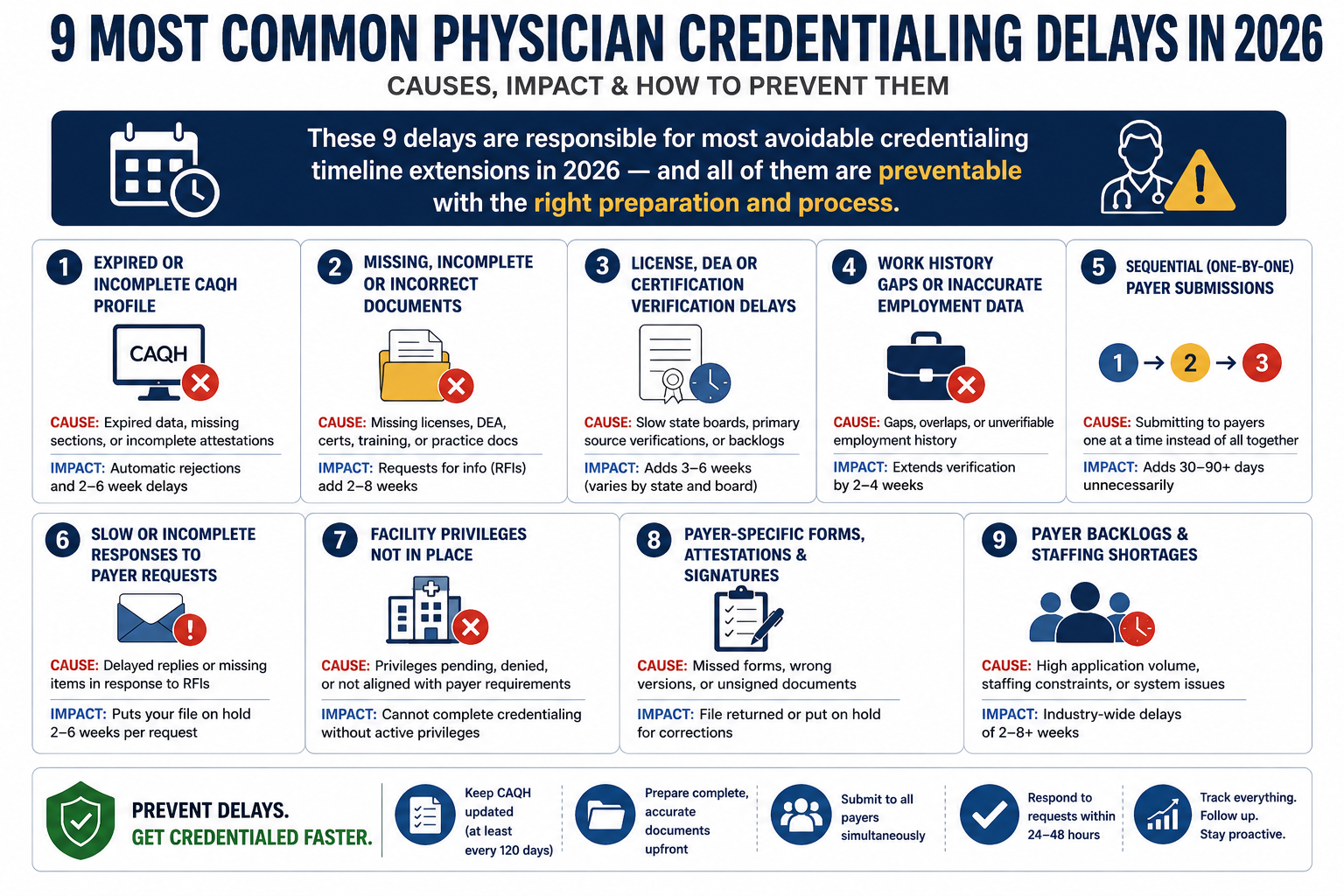
The 9 Most Common Credentialing Delays — And How to Prevent Each One
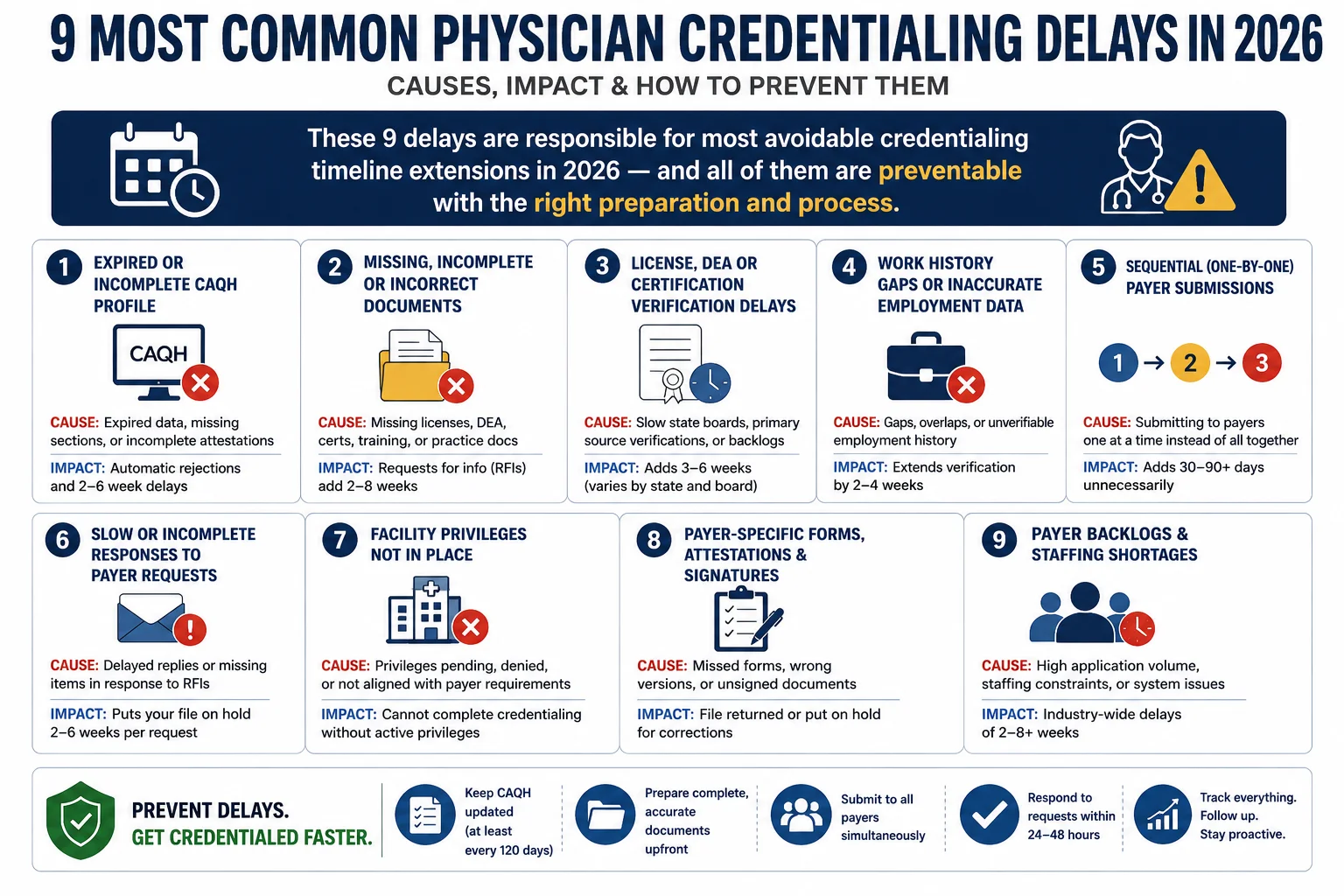
Delay 1: Starting too late. Starting credentialing 60 days before a provider’s start date almost guarantees a billing gap. The fix is simple: start 120 days before the intended start date — minimum. For California, New York, or multi-state providers, start at 150 days.
Delay 2: Expired or incomplete CAQH profile. Outdated CAQH profiles remain one of the most common credentialing problems in 2026. Incorrect provider data, outdated addresses, or missing attestations can immediately stall every payer application that draws from CAQH simultaneously. CAQH re-attestation is required every 120 days — check and attest before every credentialing cycle begins.
Delay 3: Sequential instead of simultaneous payer submissions. Waiting for Medicare approval before starting commercial applications adds months to the total timeline. Submit to Medicare, Medicaid, and all commercial payers on the same day.
Delay 4: Work history gaps. A CV with an unexplained gap greater than 30 days triggers additional payer review in 2026. Every gap in work history — including parental leave, sabbaticals, or periods between positions — must be accounted for with dates and an explanation. Prepare this documentation before submitting any application.
Delay 5: No proactive follow-up after submission. Submitting an application does not mean it is being actively processed. Payers lose documents. Applications sit in queues. Follow up with every payer every 7 to 10 business days after submission — not when you notice a problem three months later.
Delay 6: NPI and taxonomy code discrepancies. Differences in NPI details, taxonomy codes, provider names, or practice addresses across documents frequently trigger additional payer reviews. Every document in the application package must be 100 percent consistent. Industry data shows that nearly 1 in 3 credentialing applications requires corrections or resubmission — most of these trace back to data inconsistencies.
Delay 7: Submitting paper applications. Paper applications move to the back of every payer’s processing queue. In 2026, use PECOS for Medicare, CAQH for commercial payers, and each state’s online portal for Medicaid. There is almost never a legitimate reason to submit paper.
Delay 8: January and July submission timing. January and July bring the highest volume of new provider applications — hospital systems bring on residents and fellows, practices hire for the new year. Payer staff is overwhelmed and processing slows dramatically. If possible, schedule credentialing submissions for February through June or August through November.
Delay 9: Expired licenses or malpractice certificates in the application package. An expired medical license or malpractice insurance certificate submitted as current is an automatic rejection that restarts the review clock. Verify every document’s expiration date before it goes into any application.
How Much Revenue Is at Stake During Credentialing Delays
These numbers make the cost of credentialing delays concrete:
Physicians contribute an average of $200,000 to $300,000 in revenue per month to a practice. Every month of unnecessary credentialing delay is a month of that revenue either lost or postponed.
According to Medwave’s 2026 credentialing changes guide, when a provider generates $30,000 to $50,000 monthly in collections, cutting six weeks off the credentialing timeline saves $45,000 to $75,000 in opportunity cost. With enhanced 2026 requirements adding 30 to 45 days to credentialing timelines for practices doing it themselves, the revenue protected by professional credentialing support easily justifies the service cost.
For a practice bringing on two new providers simultaneously, a credentialing gap of even 6 weeks — which is easily preventable with the right process — represents $180,000 to $300,000 in delayed revenue.
The math on professional credentialing support versus in-house management is not close.
Telehealth Credentialing in 2026 — Why It Takes Longer
Telehealth credentialing consistently takes longer than in-person credentialing — and the gap widened in 2026.
The 2026 telehealth location rule strictly enforces patient-location-based licensing. A physician licensed in Georgia who provides telehealth to a patient currently located in Florida needs an active Florida license and Florida payer enrollment — not just a Georgia license. For a psychiatrist credentialing across 10 states for telehealth services, a realistic timeline looks like:
- Licensure through IMLC (parallel applications): 30 to 90 days depending on the slowest state
- CAQH profile setup and attestation: 1 to 2 weeks
- Medicare enrollment in each state: 45 to 90 days per state, run in parallel
- Commercial payer enrollment by state: 60 to 120 days per payer per state
The key word is “parallel.” Sequential multi-state credentialing — finishing one state before starting the next — extends the timeline to 6 to 12 months. Parallel submission across all target states compresses this significantly.
According to Pro Health Care Advisors’ credentialing guide, telehealth credentialing timelines in 2026 typically range between 90 and 150 days for multi-state practices — and that assumes parallel submission and complete documentation.
How Pro Health Care Advisors Manages Credentialing Timelines
Pro Health Care Advisors provides physician credentialing services for practices across the United States — handling every step of the process from CAQH setup through payer enrollment approval, with proactive follow-up that prevents the delays most practices encounter when managing credentialing internally.
Here is specifically what we do that compresses credentialing timelines:
Complete CAQH setup and maintenance. We set up new CAQH profiles, verify all documentation is current and complete before submission, and maintain 120-day attestation tracking so profiles never expire mid-enrollment.
Simultaneous multi-payer submission. We submit to Medicare, Medicaid, and all commercial payers on the same day — never sequentially. This alone can compress total credentialing timelines by 60 to 90 days compared to practices that submit one payer at a time.
Proactive follow-up every 7 to 10 business days. We track every pending application and follow up before payers ask for additional documentation — catching issues while they can still be resolved quickly rather than after weeks of inactivity.
State-specific Medicaid and MCO enrollment. We manage the state-level and MCO-level enrollment layers that practices in California, Georgia, Florida, Texas, and other managed care states must complete separately.
Re-credentialing calendar management. We track every active enrollment’s revalidation deadline and initiate re-credentialing 90 days before expiration — so billing privileges are never interrupted by a missed renewal.
Billing coordination. Because we manage both credentialing and billing for our clients, enrollment status and billing workflows stay synchronized — eliminating the coordination failures that create unbillable claim periods when credentialing and billing are handled separately.
For the complete breakdown of the 2026 credentialing process, see our physician credentialing guide.
Frequently Asked Questions — How Long Does Physician Credentialing Take
Q: How long does physician credentialing take in 2026? The realistic range is 60 to 180 days depending on payer type, state, specialty, and application accuracy. Medicare enrollment through PECOS averages 30 to 60 days for clean electronic applications. Commercial payer credentialing typically runs 60 to 120 days. Medicaid varies by state — from 45 days in faster states to 150 days in California and New York. Most practices should budget 120 days minimum when starting a new provider.
Q: Which state takes the longest for physician credentialing? California and New York consistently have the longest credentialing timelines — 120 to 150 days — due to strict verification requirements, high provider volume, and complex Medicaid managed care enrollment structures. Practices in these states should start credentialing 150 days before a new provider’s intended start date.
Q: Which payer processes credentialing the fastest? UnitedHealthcare offers the fastest standard commercial credentialing in 2026 — 60 to 90 days for standard applications, and a 45-day fast-track for primary care providers in underserved counties. Medicare PECOS is fastest for federal enrollment at 30 to 60 days for clean applications.
Q: When should I start credentialing a new physician? Start 120 days before the provider’s intended billing start date — minimum. For California, New York, or multi-state telehealth providers, start at 150 days. Starting later than 120 days before the start date almost guarantees a gap where the provider is seeing patients they cannot bill for.
Q: Can a doctor see patients before credentialing is complete? Yes — but the financial consequences are severe. Most payers do not allow retroactive billing for services rendered before credentialing approval. Once the retroactive billing window closes (typically 90 to 180 days), those services become permanently unbillable. A physician seeing patients for 90 days before credentialing approval — at $10,000 per week in collections — represents $130,000 in unrecoverable revenue.
Q: How does the IMLC help with multi-state credentialing? The Interstate Medical Licensure Compact covers 40 states plus DC and Guam as of 2026. Processing through the Compact takes 14 to 21 days after the letter of qualification is issued — significantly faster than individual state licensing applications. However, IMLC covers licensing only — payer enrollment must still be completed separately for each state.
Q: What is the most common cause of credentialing delays? According to credentialing specialists, the top causes are: starting too late (less than 90 days before start date), expired or incomplete CAQH profiles, sequential rather than simultaneous payer submissions, and undocumented work history gaps. Nearly 1 in 3 credentialing applications requires corrections or resubmission — most of these trace back to documentation inconsistencies that could have been caught before submission.
For more on how credentialing fits into your practice’s revenue cycle, see our revenue cycle management guide and our medical billing trends 2026 guide.
For more billing and credentialing resources, visit our articles and resources library.
The Bottom Line — Credentialing Timelines Are Predictable When You Plan for Them
Physician credentialing delays feel unpredictable. But they are almost always the result of predictable, preventable mistakes — starting too late, submitting incomplete applications, sequencing submissions instead of running them in parallel, and failing to follow up proactively.
The practices that credential new providers without revenue gaps are not lucky. They start 120 days before the intended start date. They submit to every payer simultaneously. They follow up every 7 to 10 business days. They keep CAQH profiles attested and current. And they track re-credentialing deadlines so billing privileges are never interrupted.
That is the process Pro Health Care Advisors builds for every credentialing client — across every state, every payer, and every specialty.
If your practice has a new provider joining — or if you are not confident that all current providers are fully enrolled and currently re-credentialed with every payer you bill — the conversation starts here.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pressure. No pitch. Just a real conversation about your credentialing timeline and exactly what it would take to protect your revenue during provider onboarding.