Dermatology Medical Billing | The Complete Guide for Private Practices (2026)
Dermatology Medical Billing — Why This Specialty Needs Its Own Approach
If you run a dermatology practice and your revenue never quite matches the volume of patients you are seeing, you are not imagining it.
Dermatology medical billing is genuinely different from billing in almost any other specialty. Not harder in a vague, general sense — harder in very specific, identifiable ways that compound quietly over months until the gap between what your practice earns and what it actually collects becomes too large to explain away.
The reason is structural. Dermatology is one of the few specialties where a single patient visit can involve a medical evaluation, one or more surgical procedures, a pathology specimen, a modifier, a separate diagnosis for the procedure versus the visit, and a cosmetic component that insurance will not touch — all in the same appointment. Each of those elements has its own coding rules, documentation requirements, and payer policies. When any one of them is handled incorrectly, the claim fails, silently adjusts downward, or gets denied entirely.
The billing problems costing private dermatology practices the most are not dramatic failures. They are quiet, systematic gaps that compound every month until the revenue difference becomes too large to explain away.
This guide covers everything a private dermatology practice needs to understand about billing in 2026 — the specific CPT codes, the documentation traps, the denial patterns, the 2026-specific changes that affect reimbursement, and the practical steps to close the revenue gaps that are almost certainly already open in your operation.
From the ProHealth Care Advisors team: We work with specialty practices — including dermatology — on billing, revenue cycle management, and prior authorization. Visit ProHealth Care Advisors for direct support with your dermatology billing operation.
Why Dermatology Billing Is in a Different Category of Complexity
Before getting into fixes, it helps to understand why dermatology billing is structurally more complicated than most other specialties.
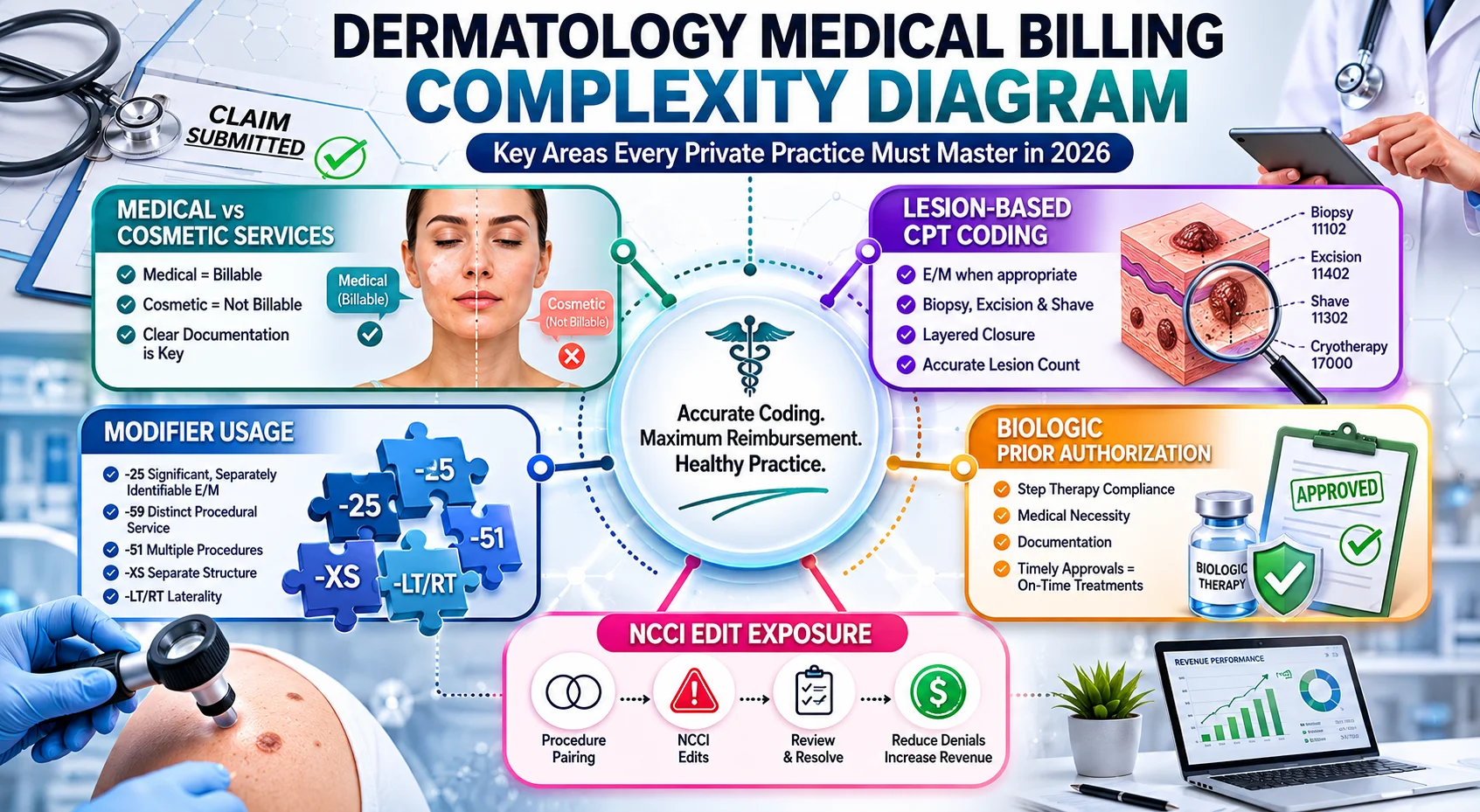
Medical versus cosmetic — the line that changes everything. Most specialties bill for medically necessary services. Dermatology spans both sides — the same physician who removes a basal cell carcinoma in one room administers Botox in the next. Insurance covers one. It does not cover the other. The documentation has to make that distinction clearly and consistently for every single service, or the medically necessary claim gets dragged into the cosmetic denial pile.
Lesion-based CPT coding demands exact measurements. Unlike most specialties where procedure codes are relatively straightforward, dermatology uses lesion size as the primary driver of which CPT code applies. The difference between a 0.5 cm excision and a 0.6 cm excision is a different code — and a different reimbursement rate. Incomplete documentation — particularly missing lesion measurements or absent pathology correlation — is among the most common causes of dermatology claim denials and audit findings.
Modifier usage is high-frequency and high-risk. Dermatology practices regularly use Modifier -25 (separate E/M service on the same day as a procedure), Modifier -59 (distinct procedural service), and Modifier -51 (multiple procedures). Dermatology combines high procedural volume, frequent modifier -25 usage, and lesion-based CPT reporting. This mix increases payer scrutiny, particularly when utilization patterns exceed peer benchmarks or when documentation lacks lesion measurement specificity.
NCCI edits create silent revenue loss. The National Correct Coding Initiative edits bundle certain code combinations that payers will not pay separately. The most common hidden revenue loss stems from excision undercoding due to incomplete lesion measurement documentation, as well as silent bundling adjustments under NCCI edits. These issues often reduce reimbursement without triggering outright denials. Silent adjustments are the worst kind — your claim gets paid, but for less than it should have been, and nobody flags it as a problem.
Biologics bring a separate billing universe. Dermatology practices prescribing dupilumab, secukinumab, ixekizumab, or other biologics for atopic dermatitis, psoriasis, or hidradenitis suppurativa are managing a billing track that runs parallel to everything else. J-code accuracy, prior authorization maintenance, buy-and-bill versus specialty pharmacy routing decisions, and Average Sales Price fluctuations all affect whether biologic billing produces the revenue it should.
The Key CPT Code Categories Every Dermatology Billing Team Must Know
Dermatology medical billing is not the same as other medical billing. It has its own set of rules, codes, and challenges that make it more complex. Dermatologists handle everything from acne treatment to skin cancer surgery, including biopsies, excisions, cryotherapy, laser therapy, and cosmetic procedures.
Here are the major CPT code categories your billing team needs to have mastered — not just generally, but with specialty-specific precision.
Evaluation and Management Codes (99202–99215)
E/M codes are used when the visit is primarily a medical evaluation — new or established patient, in-person or telehealth. In dermatology, the complexity comes when a procedure is also performed during the same visit. If the E/M is separately identifiable from the procedure — meaning the physician performed a significant, separately documented evaluation that was distinct from the pre-procedure work — Modifier -25 is appended to the E/M code. Without Modifier -25 and the documentation to support it, the E/M will be bundled into the procedure and not paid separately.
Biopsy Codes (11102–11107)
Skin biopsy codes changed significantly in 2019 and many practices are still not using them correctly in 2026. The correct code depends on the biopsy technique — tangential (shave), punch, or incisional — and whether multiple biopsies are performed. The primary biopsy uses the base code; each additional biopsy uses an add-on code. Reporting the primary code multiple times instead of the base-plus-add-on structure is a common coding error that produces claim edits or denials.
Destruction Codes (17000–17286)
Destruction codes cover cryotherapy, laser ablation, electrodessication, and chemical destruction. The correct code depends on the lesion type (benign, premalignant, or malignant), the number of lesions, and the size. Premalignant lesion destruction follows a quantity-based scale — the first lesion, the next 14, and each additional lesion all have separate code values. Malignant lesion destruction codes are size-based. Mixing these two tracks is a recurring coding error in dermatology billing.
Excision Codes (11400–11646)
Excision codes are determined by three factors: whether the lesion is benign or malignant, the anatomical location, and the excised diameter including margins. The diameter must be documented in millimeters in the clinical notes. If the measurement is missing or recorded only as an approximate estimate, the claim is vulnerable to denial or downcoding. Every excision note must contain the specific measured diameter with margins included. Pathology results should be correlated with the excision documentation.
Mohs Surgery Codes (17311–17315)
Mohs surgery billing is among the most complex in all of dermatology — and among the most audited. Each stage is billed separately. The number of tissue blocks processed per stage must be documented precisely. The pathology interpretation performed by the Mohs surgeon must be documented distinctly from the surgical excision. When a defect repair follows Mohs surgery, the repair code is billed in addition to the Mohs codes — but only if it goes beyond simple linear closure.
Biologic and Injectable Medication Codes (J-codes)
Biologic medications administered in the office are reported using J-codes — HCPCS Level II codes that correspond to specific drugs and dosing units. Common examples include J0173 for dupilumab, J3490 for unclassified biologics pending dedicated codes, and specific J-codes for each of the approved IL-17, IL-23, and JAK inhibitor therapies. J-code accuracy is critical. Biologic reimbursement risk arises when payer reimbursement tied to Average Sales Price fluctuates below acquisition cost, when J-codes are reported inaccurately, or when authorization approvals lapse before administration.
The 8 Biggest Dermatology Billing Problems in Private Practice — 2026 Data
These are the specific, recurring patterns that audit data and denial tracking consistently surface in dermatology private practices.
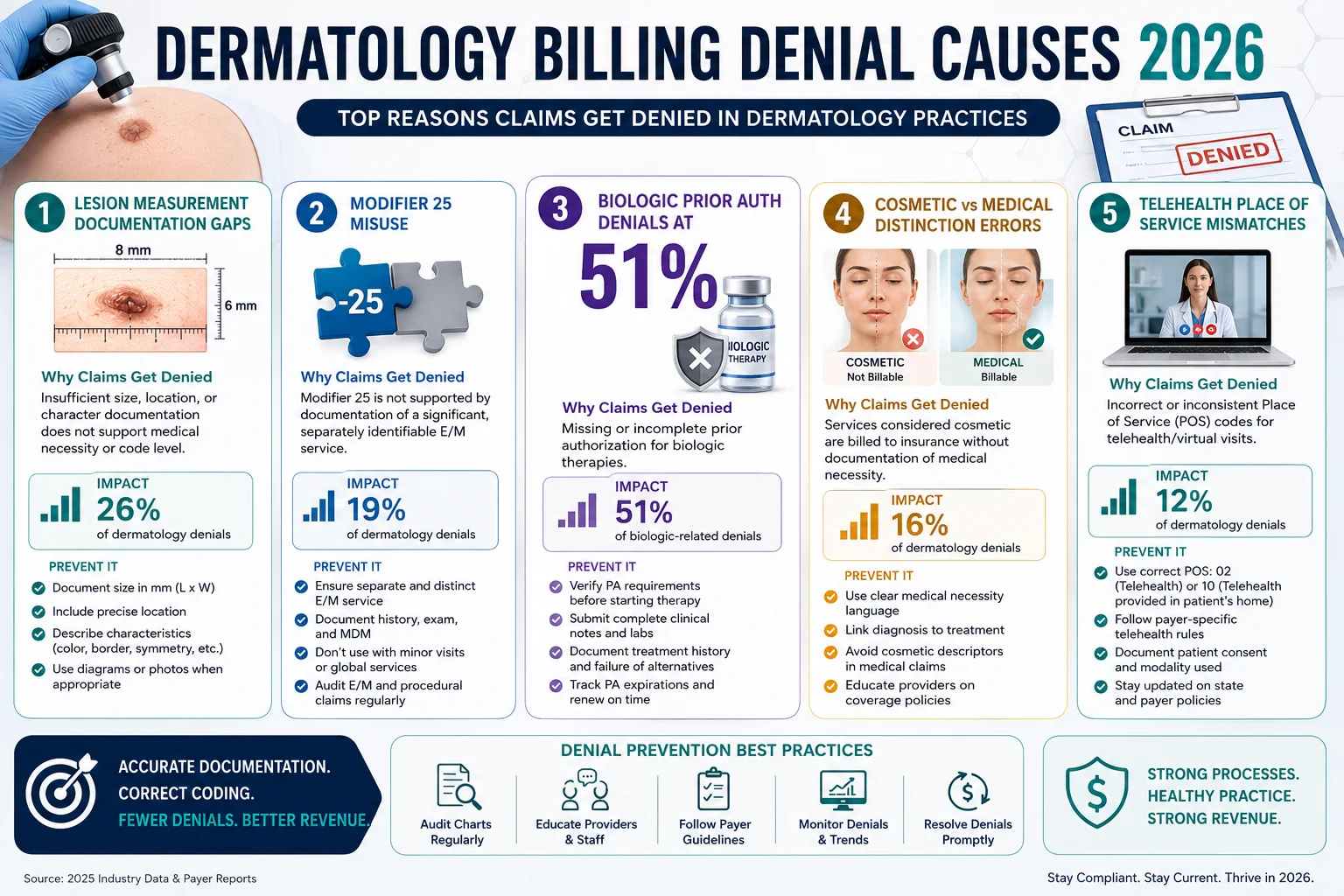
Problem 1 — Excision Undercoding Due to Missing Lesion Measurements
This is the most common source of hidden revenue loss in dermatology billing — hidden because the claim gets paid, just for less than it should. When lesion measurements are missing, incomplete, or not documented with margins included, the billing team either guesses at the code or defaults to the smallest size in the range to stay safe. The result is consistent undercoding on excisions that should be billing at higher diameter thresholds. A quarterly coding audit comparing documented measurements against submitted codes is the only reliable way to catch this pattern.
Problem 2 — Modifier -25 Denials on Same-Day E/M and Procedure Claims
Payers scrutinize Modifier -25 claims heavily in dermatology because the specialty generates a high volume of same-day E/M and procedure encounters. When the documentation does not clearly distinguish the E/M work from the pre-procedure evaluation, payers deny the E/M component. The clinical note needs to show that the physician performed a separately identifiable, medically necessary evaluation — not just a cursory pre-procedure check. Templates that combine the E/M and procedure documentation into a single note are a common source of this problem.
Problem 3 — Biologic Prior Authorization Denials at 51 Percent
Prior authorization denial rates for complex biologics and JAK inhibitors have hit a staggering 51 percent this year. This is not a minor inconvenience — it is a structural revenue problem for any dermatology practice with an active biologic program. The most common causes are insufficient step therapy documentation (showing that the patient tried and failed conventional therapies), incomplete disease severity scoring, and authorizations that lapse between renewal cycles because nobody tracks the expiration date. Biologic prior authorization needs a dedicated tracking system — not a shared spreadsheet that gets updated inconsistently.
Problem 4 — Telehealth Place of Service Errors
The risk of telehealth billing errors is significant. Medicare currently accepts POS 11 (Office) with Modifier 95, but many commercial payers have reverted to requiring POS 10 (Patient’s Home) or POS 02. Mislabeling the Place of Service is currently a top-three reason for dermatology billing rejections. A single clerical oversight applied across a high-volume week of teledermatology visits creates a significant AR backlog that is tedious and time-consuming to unwind. Your billing team needs a payer-specific telehealth matrix that is updated at the start of each year and reviewed quarterly.
Problem 5 — Cosmetic Procedure Revenue Mixed Into Insurance Claims
Some practices bill cosmetic services to insurance — either inadvertently, because the coding was not clearly separated, or because the documentation did not adequately establish medical necessity for a service that was borderline cosmetic. Payers are increasingly sophisticated at flagging these claims, and the consequences go beyond a single denial. Patterns of cosmetic claims submitted to insurance can trigger audits, recoupment demands, and compliance investigations. Every service needs a clear medical necessity rationale or a clear cosmetic designation before it is coded.
Problem 6 — Skin Substitute Reimbursement Collapsed in 2026
The most dramatic swing factor for many dermatology practices in 2026 is the treatment of skin substitutes. CMS finalized a framework that treats these products as “incident-to” supplies under the MPFS, replacing separate product payments with a single national product rate per unit. This can cut reimbursement for some office-based skin substitute products by up to roughly 90 percent compared with prior payment methodologies — particularly for advanced wound and amniotic graft products. Practices with a meaningful wound care or limb-salvage component that have not restructured their skin substitute billing model are taking a severe revenue hit in 2026 that will not self-correct.
Problem 7 — NCCI Bundling Edits Reducing Multi-Lesion Claims Silently
When multiple procedures are performed on the same date — excision and destruction on different lesions, for example — NCCI edits determine which codes can be billed separately and which must be bundled. When codes are bundled that should have been separated using Modifier -59, the practice receives one reimbursement instead of two. This happens without a denial notice. It shows up only if someone is reviewing EOBs against what was submitted and catching the payment shortfalls. Most small practices do not have a systematic process for this review.
Problem 8 — Pathology Correlation Documentation Gaps
When a biopsy or excision is sent for pathology, the results need to be correlated with the procedure documentation in the patient’s record. Missing pathology correlation — meaning the pathology result was received but never documented as reviewed and integrated into the clinical picture — creates vulnerability during audits and can contribute to medical necessity denials on subsequent treatment claims. Establish a workflow that closes the loop on every pathology result before the chart is considered complete.
Dermatology Telehealth Billing — What Changed in 2026
Teledermatology has become a standard part of dermatology practice for follow-up visits, acne management, rash evaluations, medication monitoring, and post-procedure checks. Teledermatology is uniquely well-suited for visual assessment, follow-up care, and chronic condition management.
But the billing rules for teledermatology are not uniform across payers, and 2026 brought further fragmentation. Here is the current landscape:
Medicare: Standard E/M codes (99202–99215) are accepted for synchronous audio-video telehealth visits. Place of Service 11 with Modifier 95 is the current accepted format for most Medicare teledermatology encounters. Audio-only visits have more limited coverage and require specific documentation of why video was not available or appropriate.
Commercial payers: This is where fragmentation is worst. Some commercial plans accept the same POS 11 with Modifier 95 format as Medicare. Others have reverted to requiring POS 10 (patient’s home) or POS 02. Some require GT modifier instead of 95. Some cover teledermatology visits at parity with in-person visits; others reimburse at a lower rate. Because dermatology claims have some of the highest denial rates for telehealth coding inconsistencies, verifying payer-specific telehealth rules annually — and keeping a payer matrix — is essential.
Store-and-forward teledermatology: Some payers cover asynchronous teledermatology where the patient submits photos that the dermatologist reviews without a real-time visit. Coverage is inconsistent and documentation requirements are payer-specific. Confirm coverage before building store-and-forward into your workflow for insurance patients.
The practical fix: your billing team needs a current payer-specific telehealth matrix — a document that tracks POS requirements, modifier requirements, coverage parity status, and documentation standards by payer. Update it at the start of every year and review it whenever a payer sends a policy update.
Biologic Billing in Dermatology — A Full Breakdown
Biologics are one of the fastest-growing revenue components in dermatology — and one of the most complex to bill correctly. Here is how to manage the major elements.
Buy-and-bill versus specialty pharmacy routing. For biologics administered in the office, buy-and-bill — where the practice purchases the medication and bills the payer for both the drug and its administration — generates stronger revenue per dose than specialty pharmacy routing when managed correctly. But buy-and-bill only works when J-codes are accurate, prior authorizations are maintained, and the practice is regularly verifying that Average Sales Price reimbursement exceeds acquisition cost. When ASP reimbursement falls below acquisition cost — which does happen, especially for newer biologics — the buy-and-bill model loses money per dose administered.
Step therapy documentation. Most payers require documented evidence that a patient tried and failed conventional therapies before approving a biologic. For atopic dermatitis biologics, this typically means documented failure of topical corticosteroids and/or calcineurin inhibitors. For psoriasis biologics, failure of conventional systemics like methotrexate or cyclosporine. The clinical documentation of this step therapy history must be in the chart and clearly referenced in the PA request — not just known to the treating physician.
Authorization tracking and renewal. Biologic authorizations typically run for 6 to 12 months. When they expire and the practice has not proactively renewed, the next administration is either denied entirely or paid at an out-of-network rate. Build a renewal reminder process — at minimum 60 days before expiration — for every active biologic authorization in your practice.
J-code accuracy and unit reporting. Each biologic has a specific J-code and a specific unit value tied to dose. Dupilumab (Dupixent) is reported using the dose-specific J-code with the correct number of units for the dose administered. Reporting the wrong unit count — even for the correct J-code — produces a claim that either pays at the wrong rate or denies outright. Verify J-code assignments and unit calculations quarterly against current CMS data.
For support managing prior authorizations for complex biologics, see our Prior Authorization Support Services. Also see our Prior Authorization Rules Changed 2026 guide for the CMS rule changes that directly affect biologic PA timelines.
Documentation Standards That Protect Dermatology Claims
Documentation is where most dermatology billing problems originate. The clinical note must contain specific elements for every category of service — not as a bureaucratic exercise, but because these elements are what payers and auditors look for when evaluating claims.
For every excision: Document the specific measured diameter of the lesion including surgical margins, in millimeters. Document the anatomical location precisely. Document the lesion type (benign versus malignant) with clinical justification. Document whether the specimen was sent for pathology and the result. Document separately the medical necessity reasoning if a same-day E/M is also being billed.
For every biopsy: Document the technique used — tangential, punch, or incisional. Document each lesion biopsied separately when multiple biopsies are taken. Document the clinical indication for each biopsy. Confirm pathology results are correlated and documented in the chart when received.
For every destruction procedure: Document the lesion type and the basis for that classification. For premalignant lesions, document the number of lesions destroyed. For malignant lesions, document the size. Document the destruction method.
For every E/M billed with a procedure on the same day: Document that the E/M represents a separately identifiable medical decision-making process that was distinct from the pre-procedure evaluation. The note should read as if it stands alone from the procedure documentation.
For every cosmetic service: Document that the patient was advised the service is cosmetic, that insurance does not cover it, and that payment is the patient’s responsibility. Keep cosmetic billing completely separated from medical billing at the claim level.
The Dermatology Revenue Cycle — How the Full Process Should Work
A well-run dermatology revenue cycle has specific checkpoints at every stage. Here is what that looks like from scheduling through collections.
Scheduling: Verify insurance eligibility and confirm whether the planned service requires prior authorization. For biologic administrations, confirm the authorization is current and will be valid on the date of service. Identify new Medicare Advantage patients and flag their plan type — HMO patients need referral verification before the visit.
Check-in: Re-verify eligibility on the date of service. Confirm copay and deductible status. Collect patient responsibility estimates upfront. Separate medical and cosmetic visit documentation workflows at check-in.
Clinical documentation: Physician documents each service with the specific elements required for the service type. Measurements for excisions. Technique for biopsies. Lesion count for destruction. Separate E/M documentation when applicable.
Coding and charge entry: Coding staff reviews documentation against the CPT code selected. Modifiers are applied where appropriate and documented. NCCI edit exposure is reviewed for multi-procedure visits. Cosmetic services are coded separately.
Claim scrubbing and submission: Claims are reviewed for completeness before submission. Code pairs are validated against NCCI edits. Modifier usage is checked for documentation support. Telehealth claims are reviewed for correct POS by payer.
Denial management: Denials are categorized on the day received and routed to the appropriate team member. Documentation denials go back to the clinical team for additional information. Prior authorization denials are evaluated for appeal or peer-to-peer review eligibility. Bundling adjustments are compared against submitted codes to identify missed Modifier -59 opportunities.
Patient billing: Patient statements go out promptly after insurance processing. Payment plan options are offered at the time of the first statement for balances above a set threshold. A structured follow-up process ensures patient balances do not age past 90 days without contact.
For a full audit of how your current dermatology revenue cycle is performing, see our Revenue Cycle Health Check.
External resource: CMS Local Coverage Determinations for Dermatology Procedures for current Medicare coverage criteria your billing team must follow.
Dermatology Billing in Georgia — What Makes the Local Market Specific
Georgia dermatology practices operate in a billing environment with layers that affect how the general billing principles above apply in practice.
Georgia Medicaid covers dermatology services through managed care organizations — Amerigroup, Peach State Health Management, and WellCare — each with its own prior authorization requirements for biologics, phototherapy, and certain surgical procedures. The Medicaid PA denial rate for dermatology biologics in Georgia’s CMO structure has mirrored the national 51 percent figure, meaning practices serving Medicaid patients with moderate-to-severe atopic dermatitis or psoriasis are navigating high denial rates specifically in the biologic category.
Georgia’s commercial payer market includes major plans from Blue Cross Blue Shield of Georgia, Cigna, Aetna, UnitedHealthcare, and Humana — each with different policies on teledermatology, biologic step therapy requirements, and skin substitute coverage. BCBS of Georgia, for example, has its own medical policy on biologic step therapy for atopic dermatitis that differs from the national BCBS guidelines. Billing teams that apply a single set of rules across all commercial payers miss these differences consistently.
For practices in the Atlanta metro serving a high proportion of commercially insured patients, the telehealth POS fragmentation is especially impactful — the mix of payers creates a situation where the same teledermatology visit needs to be coded differently depending on which patient’s insurance is being billed.
For more on Georgia-specific billing requirements, see our Georgia Medical Billing Guide and our Medical Billing and Practice Management services page.
External resource: Georgia Department of Community Health — Medicaid Provider Portal for current Georgia Medicaid dermatology billing requirements.
Frequently Asked Questions — Dermatology Medical Billing 2026
What makes dermatology billing different from other specialties?
Dermatology billing is more complex than most specialties for several specific reasons. It spans medically necessary and cosmetic services that must be completely separated at the claim level. CPT code selection for excisions, destructions, and biopsies depends on precise lesion measurements that must be in the clinical documentation. Modifier usage is high-frequency and heavily audited. Biologic billing adds a parallel prior authorization and J-code track. And NCCI edits create silent underpayment risks that do not trigger denial notices. Any one of these factors alone creates billing complexity. All of them together in a single practice makes dermatology billing one of the most specialist-dependent revenue cycles in healthcare.
What is the correct way to bill a same-day E/M and procedure visit in dermatology?
When an evaluation and management visit and a procedure occur on the same date of service, the E/M can be billed separately only if it represents a separately identifiable medical service — meaning the physician performed a distinct evaluation that was not simply pre-procedure assessment. Modifier -25 must be appended to the E/M code. The clinical documentation must support the Modifier -25 by clearly showing the separately identifiable evaluation work in the note. Without both the modifier and the supporting documentation, the E/M will be bundled into the procedure and denied.
Why are biologic prior authorization denials so high in dermatology?
The 51 percent prior authorization denial rate for biologics and JAK inhibitors in dermatology in 2026 reflects several compounding factors. Payers require extensive step therapy documentation showing conventional treatment failure before approving biologics. Disease severity scoring using validated tools like EASI or PASI must be documented and submitted with the PA request. When these elements are missing, incomplete, or not framed in the terminology the payer’s review system expects, the authorization is denied. Most practices that see high biologic PA denial rates have a documentation workflow problem — not a clinical problem.
How do I know which CPT code to use for a skin excision?
The correct excision CPT code depends on three things: whether the lesion is benign or malignant, the anatomical location, and the excised diameter including surgical margins measured in centimeters. For benign lesions, CPT codes 11400–11446 apply. For malignant lesions, codes 11600–11646 apply. Within each range, the code is selected based on the size range that includes the measured excised diameter. The measurement must be documented in the clinical note — if it is not there, the claim is vulnerable regardless of which code was submitted.
What is the skin substitute billing change in 2026?
CMS finalized a framework in 2026 that reclassifies many skin substitute products as “incident-to” supplies under the Medicare Physician Fee Schedule, replacing separate product payments with a single national product rate per unit. For some advanced wound care and amniotic graft products, this can reduce reimbursement by up to 90 percent compared to prior payment rates. Practices with wound care or limb-salvage programs using these products need to urgently review their skin substitute billing model and assess whether continued buy-and-bill is financially viable for specific products under the new rate structure.
What are the most common reasons dermatology claims are denied?
The most common denial reasons in 2026 dermatology billing are: missing or incomplete lesion measurement documentation, Modifier -25 claims where the documentation does not clearly support a separately identifiable E/M, biologic prior authorization denials due to incomplete step therapy documentation, telehealth place of service errors where the wrong POS code is used for a specific payer, and cosmetic services submitted to insurance without adequate medical necessity documentation. Each of these denial types has a specific documentation or workflow fix that reduces the rate significantly once identified.
Should a private dermatology practice outsource its billing?
For most private dermatology practices, outsourcing to a billing service with genuine dermatology specialty experience produces better financial outcomes than general in-house billing. The specialty-specific coding complexity — lesion-based CPT selection, biologic J-code accuracy, modifier application, NCCI edit management — is not something a generalist billing team handles well without specific training and ongoing education. The key is selecting a service with documented dermatology experience, not just one that claims to handle all specialties.
How does teledermatology billing differ from in-person billing?
Synchronous teledermatology visits use the same E/M codes as in-person visits but require specific place of service codes and modifiers that vary by payer. Medicare currently accepts POS 11 with Modifier 95 for most teledermatology encounters. Many commercial payers require POS 10 or POS 02 instead. Some require Modifier GT rather than 95. Reimbursement rates for telehealth visits vary — some payers reimburse at parity with in-person; others at lower rates. Because place of service errors are among the top three reasons for dermatology billing rejections, maintaining a payer-specific telehealth billing matrix is essential.