Medicare Advantage Denials Up 56% — What Private Practices Must Do Right Now 2026
There is a number that has been circulating in healthcare revenue cycle circles for the past year. That number is 56.
A 56 percent increase in Medicare Advantage prior authorization denials. Measured by Syntellis Performance Solutions and the American Hospital Association across data from more than 1,300 hospitals and health systems. Confirmed by OIG investigations. Validated by what private practices across the country are experiencing every single week in 2026.
If your practice has been seeing more Medicare Advantage denials lately, you are not doing anything wrong. You are caught in a system that has fundamentally changed how it handles claims — and changed it fast.
This guide explains exactly what is driving the denial surge, which services are getting hit hardest, why 2026 is uniquely difficult compared to previous years, and the specific steps private practices can take right now to stop the revenue bleed.
From the ProHealth Care Advisors team: We work with private practices daily on Medicare Advantage billing and denial management. Everything here reflects current 2026 data and operational realities. Visit ProHealth Care Advisors for hands-on support with your MA revenue cycle.
The Numbers Behind the 56% Denial Surge
Let us start with the actual data — because understanding the scale of this problem is what makes the solutions feel urgent rather than optional.
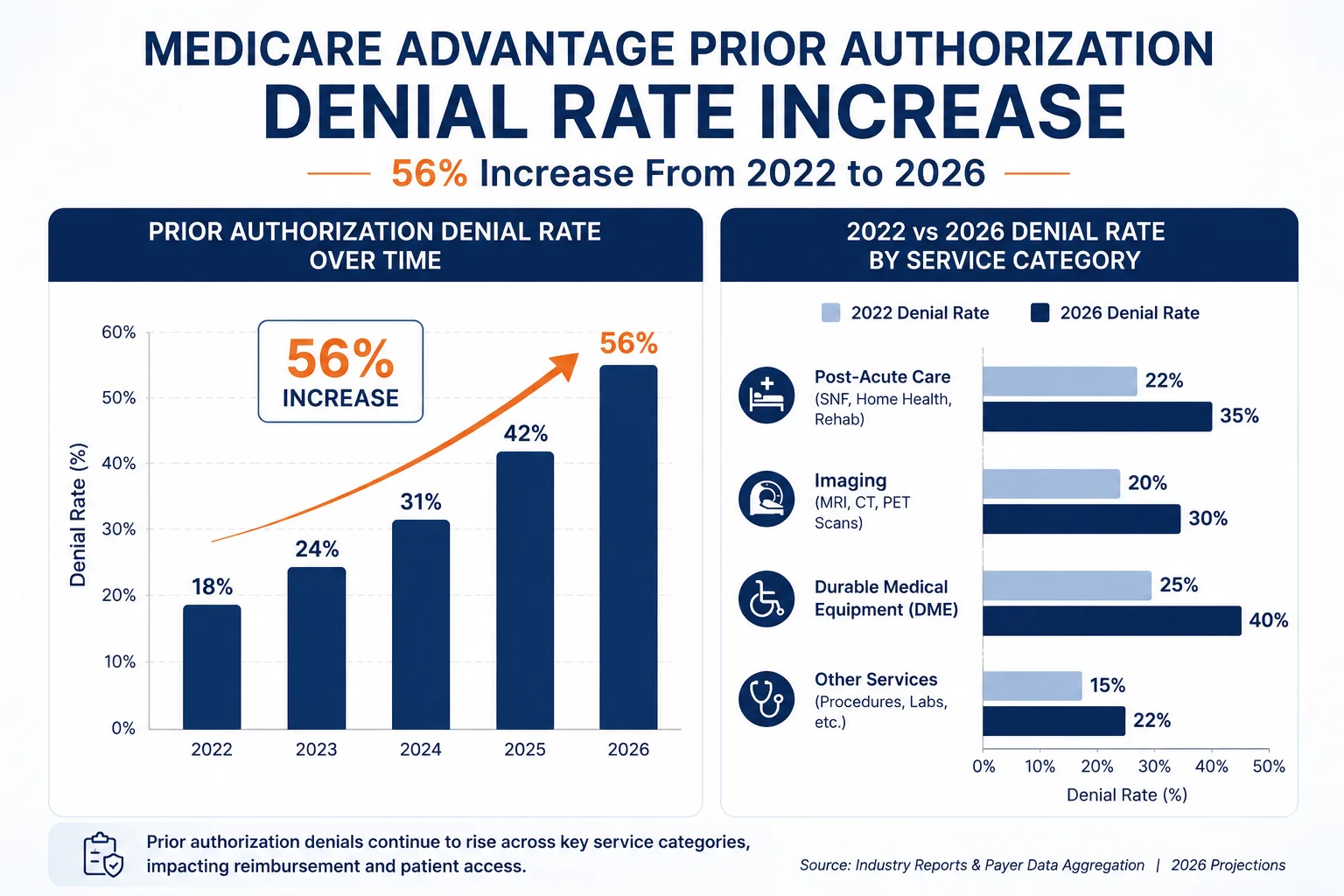
The 56% figure: Analysis from Syntellis Performance Solutions and the American Hospital Association found a nearly 56 percent increase in Medicare Advantage prior authorization denials between January 2022 and July 2023. That trend has not reversed. It has accelerated.
The initial denial rate: Research published in Health Affairs found that 17.7 percent of Medicare Advantage claims are denied on initial submission. That means nearly one in five claims your practice submits to an MA plan gets rejected the first time it is reviewed.
The appeal overturn rate: Here is the number that tells you how wrong those initial denials are. Approximately 57 percent of all denied MA claims are overturned on appeal — meaning more than half of the claims that get rejected should have been paid in the first place. One analysis of 2026 denial data puts the appeal overturn rate even higher, at 80.7 percent for certain service categories. Practices that do not appeal are leaving enormous recoverable revenue on the table.
The net revenue impact: Despite high overturn rates, Health Affairs research found that MA denials produce a 7 percent net reduction in provider revenue — because a significant portion of denied claims are never appealed at all. Staff capacity, time pressure, and the complexity of the appeals process all contribute to claims dying in the denial queue rather than getting worked.
The 2026 specific spike: Medicare Advantage plans saw a 4.8 percent spike in overall denial rates from 2023 to 2024, and that pace continued into 2026 as AI-powered review algorithms became standard across major MA plans. In 2024 alone, MA plans processed nearly 53 million prior authorization determinations — and the denial rate on those requests kept climbing.
Why 2026 Is Uniquely Dangerous for Private Practice MA Billing
The 56 percent denial increase did not happen in a vacuum. And 2026 has added new layers of difficulty on top of an already-difficult situation. Here are the specific forces making this year particularly hard.
1 — 2.9 Million Patients Are in Plans They Did Not Choose
This is the defining story of Medicare Advantage in 2026, and it has direct billing consequences for every private practice.
According to Johns Hopkins Bloomberg School of Public Health research published in February 2026, approximately 2.9 million Medicare Advantage enrollees were forced into new plans for 2026 after a historic wave of insurer exits and service area reductions. UnitedHealthcare and Humana alone exited more than 300 counties. KFF data confirmed that 15 percent of local PPO Medicare Advantage plans were canceled for 2026.
What does that mean at the practice level? It means your long-term Medicare Advantage patients — the ones whose coverage you knew, whose authorization requirements you understood, whose plans you had built billing workflows around — are now on different plans. Plans they were automatically enrolled in. Plans they often do not fully understand themselves. Plans your billing team may not have seen before.
The prior authorizations you held for those patients? Invalidated when the plan changed. The eligibility data in your system? Potentially wrong as of January 1, 2026. The documentation standards you built for their old plan? Not necessarily applicable to the new one.
This enrollment disruption created what revenue cycle analysts are calling a “perfect storm” for preventable denials in 2026 — and most of those denials hit practices that had no idea their patients had switched plans.
The billing fix: Real-time eligibility verification at the time of scheduling and again on the date of service is no longer optional. It is a necessary part of every patient encounter involving a Medicare Advantage beneficiary in 2026.
2 — AI Is Reviewing Claims Before Any Human Sees Them
The major Medicare Advantage plans have deployed AI-powered claim review algorithms that process prior authorization requests in seconds — often without meaningful clinical review by a human being. These algorithms are designed to identify patterns associated with overutilization and flag or deny requests that fall outside expected parameters.
The problem is that these algorithms are not always right. An OIG investigation found that MA organizations were denying prior authorization requests that actually met Medicare coverage criteria — meaning the algorithm rejected care that the patient was legally entitled to receive. The OIG raised serious concerns about whether cost containment had crossed the line into access restriction.
For private practices, this means documentation written for a human reviewer does not always work with an algorithmic reviewer. Your clinical notes need to be structured with the specific indicators these algorithms look for — not just thorough in a general clinical sense, but targeted in the specific terminology and code combinations the AI is programmed to recognize as valid.
3 — HMO Plans Now Cover More Patients Than Before
The 2026 enrollment disruption pushed many patients from flexible PPO plans into more restrictive HMO plans — often because HMOs had lower premiums and broker agents moved patients into them without fully explaining the referral and authorization requirements.
HMO plans require a valid referral from a primary care physician before a specialist visit. If your specialist practice sees an HMO patient without a valid referral on file, that claim will be denied — and no amount of appealing will change the outcome. The claim stays denied because the referral requirement is a contractual access rule, not a clinical judgment call.
With an estimated 57 percent of all Medicare Advantage plans now being HMO plans in 2026, the likelihood of your practice encountering an HMO patient who does not know their own plan type has increased significantly. The billing risk is real and specific.
4 — Chronic Condition Special Needs Plans Are Expanding Fast
C-SNPs — Chronic Condition Special Needs Plans — grew by an estimated 42 percent in 2026. These plans cover patients with specific chronic conditions like diabetes, heart failure, or end-stage renal disease, and they receive higher reimbursement rates from CMS in exchange for serving this population.
The billing complexity: C-SNPs often require diagnosis coding to be specific to the condition that qualifies the patient for the plan. If your coding team uses a general ICD-10 code instead of the specific code the C-SNP plan requires, the claim may deny — not because the service was not medically necessary, but because the code did not match the plan’s eligibility criteria.
As more of your Medicare Advantage patients shift into C-SNPs, your coding team needs to know which patients are on these plans and what specific coding requirements apply.
Which Services Are Getting Denied the Most
Not every service is equally at risk. Here is where the 2026 denial data is showing the highest rates:
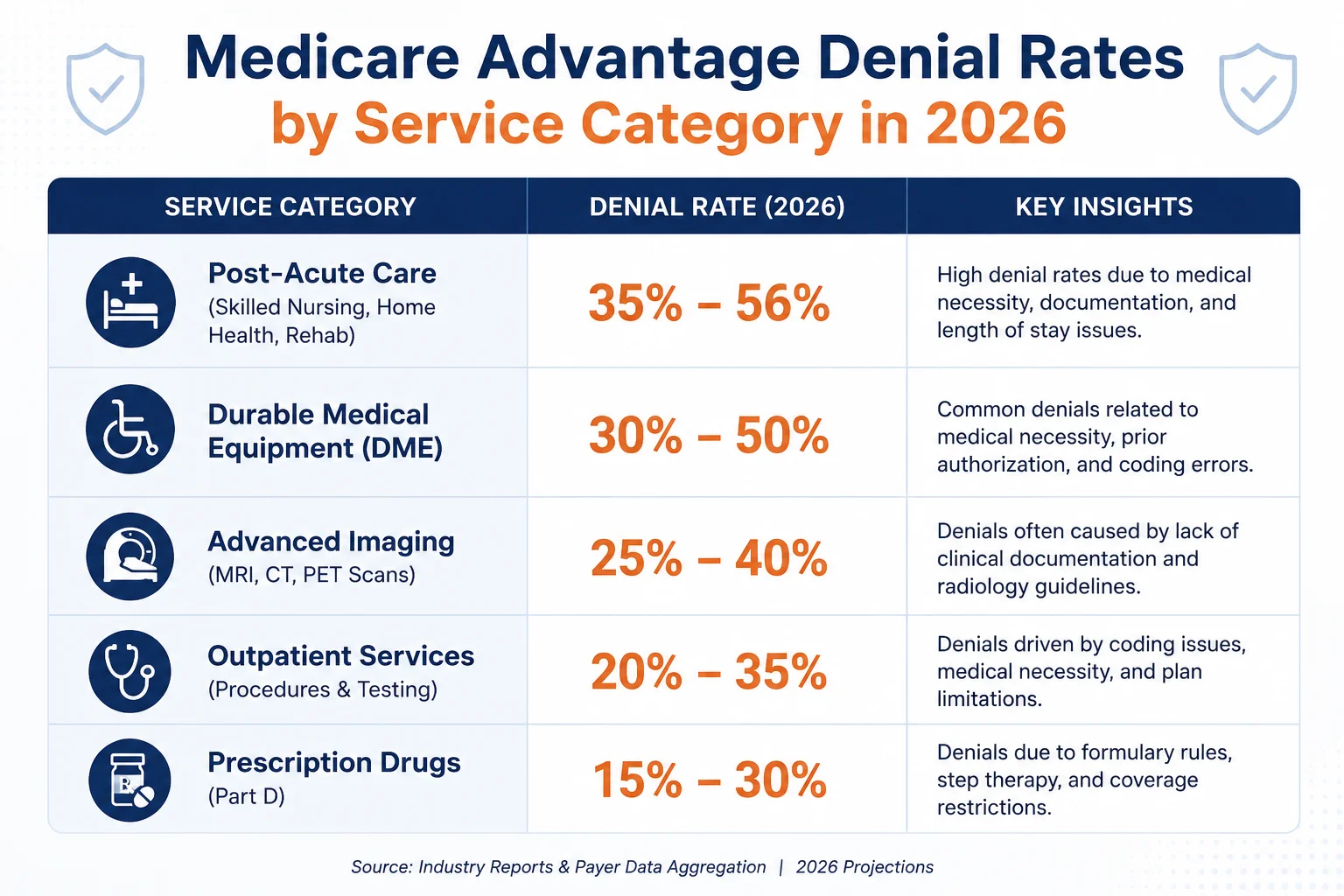
Post-acute care (skilled nursing, home health, wound care): Denial rates of 35 to 56 percent. These services face the highest scrutiny because MA plans view them as high-cost and discretionary.
Durable medical equipment: Denial rates of 30 to 50 percent. Documentation requirements are specific and frequently incomplete on initial submission.
Advanced imaging (MRI, CT, PET): Denial rates of 25 to 40 percent. AI-based medical necessity review is especially active for imaging authorizations. MRI denials increased significantly in 2026 as MA plans tightened necessity criteria beyond what traditional Medicare requires.
Injectable medications: Denial rates of 20 to 35 percent, with particularly high denial rates for specialty biologics and infusion therapies where the medical benefit drug prior authorization rules are still in flux.
Specialist visits without referrals (HMO plans): Near 100 percent denial rate when the referral requirement is missed. These are mostly preventable with proper eligibility checks.
Pain management and orthopedic procedures: Specifically affected in the six WISeR states — see our Prior Authorization Rules Changed 2026 guide for the WISeR service list.
What the CMS 2026 Rules Changed for MA Denials
The 2026 CMS interoperability rules — specifically CMS-0057-F — did bring some important protections that private practices can use to their advantage.
Shorter decision windows — now enforceable. Under the new rules, MA plans must issue standard prior authorization decisions within 72 hours and expedited decisions within 24 hours. Before this rule, payers had significantly more time. If a plan is exceeding these windows, you now have grounds to escalate.
Specific denial reasons are now required. MA plans can no longer issue vague denials like “not medically necessary” without further explanation. Every denial must include a specific clinical reason tied to coverage criteria. This matters enormously for appeals — a specific reason is something your team can argue against with documentation.
Public reporting is now mandatory. MA plans must publicly report their approval rates, denial rates, and appeal outcomes. This data is beginning to surface, and it gives practices intelligence about which plans have unusually high denial rates on specific service types — information you can use to build stronger first submissions.
External resource: CMS — CMS Interoperability and Prior Authorization Final Rule CMS-0057-F for the full rule text.
6 Steps Private Practices Must Take Right Now
These are not general suggestions. These are the specific workflow changes that the 2026 denial data tells us matter most.
Step 1 — Run real-time eligibility verification at scheduling and on the date of service. With 2.9 million patients in new MA plans for 2026, your records from last year may be wrong today. Check eligibility at scheduling. Check again on the day of the appointment. For patients in plans that changed January 1, treat their coverage as unverified until confirmed.
Step 2 — Verify the plan type — HMO versus PPO — for every Medicare Advantage patient. This takes 60 seconds and prevents the most common and most irreversible denial category. HMO patients need a valid referral on file before the visit. If there is no referral, do not proceed until one is obtained. The claim will not survive an appeal without it.
Step 3 — Build your clinical documentation for algorithmic review, not just human review. Your notes need to include specific clinical indicators, the exact diagnosis codes relevant to the plan, functional limitation language, and medical necessity statements that match the terminology the payer’s review system looks for. Generic clinical language that a human reviewer would accept often fails automated screening.
Step 4 — Establish a same-day denial routing process. Every MA denial should be routed the same day it is received to a designated team member responsible for triage. First, determine whether the denial reason is something your practice can address — incomplete documentation, wrong code, missing referral — or whether it requires a clinical appeal. Urgency matters because timely filing windows for MA appeals are specific and shorter than many practices realize.
Step 5 — Appeal every denial that has clinical merit. The 57 to 80 percent overturn rate on MA appeals means that most denials worth appealing get overturned. The practices leaving the most money on the table are the ones that write off denials as lost rather than working them. Build an appeal into your workflow as a default response to any denial where the service was medically necessary.
Step 6 — Track denial patterns by MA plan and by service type. Monthly data on which plans are denying most frequently, and for which services, tells you where to focus documentation improvements. If one plan denies your imaging orders at three times the rate of another, that is a signal to investigate their specific criteria and adjust your first-submission documentation accordingly.
For a complete audit of your current MA denial rate and recovery process, our Revenue Cycle Health Check covers the full benchmark analysis.
The Financial Reality — What Unworked MA Denials Cost Your Practice
Let us put a number to this. A private practice billing $2 million annually in Medicare Advantage revenue with a 17 percent initial denial rate and a 40 percent non-appeal rate is leaving approximately $136,000 per year in recoverable revenue unworked. That is money the practice earned for services it provided to real patients — and it is sitting in the denial queue because no one has the bandwidth to work it.
For most private practices, that is not a billing problem. It is a capacity problem. The billing team is managing front-end PA submissions, patient statements, payer credentialing renewals, and a dozen other tasks. Denial management is the thing that gets done when everything else is done — which means it frequently does not get done at all.
This is exactly the scenario where a specialized revenue cycle partner adds measurable, calculable value. A denial management process that captures 60 percent of currently unworked MA denials at the industry overturn rate of 57 percent returns meaningful dollars to a practice that would otherwise write them off.
For more on how this works in a private practice environment, see our Medical Billing and Practice Management services page.
External resource: American Medical Association — Prior Authorization Reform and Advocacy for national data on the scope of the MA denial problem.
Georgia Practices — What the MA Denial Surge Means in Your Market
For Georgia private practices, the 2026 MA denial situation carries some additional layers.
Georgia had significant Medicare Advantage plan exits and service area reductions for 2026. Practices across the state — particularly outside the Atlanta metro — are seeing patients arrive on unfamiliar MA plans with different network requirements, different prior authorization rules, and different documentation standards than what the practice previously managed.
Georgia’s MA market includes major plans from UnitedHealthcare, Humana, Aetna, Cigna, and Blue Cross Blue Shield of Georgia, each with its own prior authorization requirements layered on top of the CMS baseline rules. The increase in C-SNP enrollment is visible in Georgia practices serving patients with high rates of diabetes, heart failure, and kidney disease — conditions that are prevalent in the state’s demographic profile.
The OIG finding that MA plans were denying care that met Medicare coverage criteria applies nationally — including Georgia. Practices in this state have grounds to appeal denials aggressively when the service was medically necessary under Medicare coverage standards, regardless of what the MA plan’s internal criteria claim.
For Georgia-specific billing support and MA denial management, see our Georgia Medical Billing Guide and our Prior Authorization Support Services.
External resource: Georgia Medicaid Division — Provider Information for Georgia-specific payer compliance standards that run parallel to MA requirements.
Frequently Asked Questions — Medicare Advantage Denials Up 56%
Why are Medicare Advantage denials so much higher than traditional Medicare denials?
Traditional Medicare uses relatively straightforward fee-for-service billing with limited prior authorization requirements outside of specific DME and home health categories. Medicare Advantage plans are privately administered and allowed to set their own prior authorization requirements beyond Medicare’s baseline — meaning they can require approval for services that traditional Medicare would pay without prior review. This structural difference, combined with financial incentives to control costs, drives substantially higher denial rates in MA versus original Medicare.
What is the 80.7 percent appeal overturn rate telling us?
It tells us that the vast majority of Medicare Advantage denials issued in certain service categories are wrong — the services were medically necessary and covered, and the plan should have paid them on first submission. The high overturn rate is not a coincidence. OIG investigations have specifically found that MA organizations denied prior authorization requests that met Medicare coverage criteria. Practices that do not appeal are accepting losses they do not have to absorb.
Why are 2.9 million patients switching MA plans relevant to my billing in 2026?
Because a patient who changed plans on January 1, 2026 is now covered by a plan with different prior authorization requirements, different documentation standards, and different networks. Any authorization you obtained under their old plan is invalid. Any eligibility data in your system from 2025 may be wrong. If you bill the wrong plan or submit documentation structured for a different plan’s criteria, you will receive a denial that is preventable with proper eligibility verification.
What is a C-SNP and why does the coding matter differently?
A Chronic Condition Special Needs Plan covers patients with specific qualifying conditions. These plans receive higher federal payments for serving this population and in return apply specific coding requirements tied to the qualifying condition. If your claim does not use the exact diagnosis code the plan requires for the qualifying condition, it may deny — not because the service was inappropriate, but because the coding did not match the plan’s eligibility criteria. As C-SNPs grew by 42 percent in 2026, this coding distinction affects more patients than ever.
How do I know which Medicare Advantage plan a patient is on in 2026?
Real-time eligibility verification through your clearinghouse or EHR should return the current plan information at the time of the check. Do not rely on last year’s records. For patients who appear to be on an MA plan, confirm the plan name, plan type (HMO or PPO), effective date, and whether any prior authorization is required for the planned service before the visit occurs.
What happens if a Medicare Advantage plan misses the 72-hour decision window?
Under the 2026 CMS rules, impacted MA plans are required to issue standard prior authorization decisions within 72 hours. If a plan is consistently exceeding this window, you should document the submission date and the response date, then escalate through the payer’s formal complaint process. In some state regulatory environments, a missed timeline can result in the authorization being deemed approved. Track these patterns — repeated violations by the same payer are something your billing team and legal advisor should flag.
Is it worth appealing every Medicare Advantage denial?
Not every denial has equal appeal merit. Denials due to a missed HMO referral, for example, are structural and not typically overturnable. But denials based on medical necessity, documentation insufficiency, or prior authorization decisions on services that met Medicare coverage criteria are worth appealing in most cases. The 57 to 80 percent overturn rate tells you that the investment of time in a well-prepared appeal consistently returns more revenue than writing off the denial.