What Is Revenue Cycle Management? The Complete 2026 Guide for Healthcare Practices
Every dollar your practice earns starts with a patient walking through the door.
But getting that dollar from the moment of care to your bank account is not a straight line. It travels through insurance verification, clinical documentation, charge capture, claim coding, submission, payer adjudication, payment posting, denial management, and patient collections — and it can fall off the track at any one of those points.
The system that manages all of that movement is called revenue cycle management. And in 2026, it is not just a back-office function. It is the financial backbone of your entire practice.
Billing is no longer a quiet task in the back office — it has become the heart of a practice. Today, it drives cash flow, patient trust, and long-term success.
This guide explains exactly what revenue cycle management is, how each step of the cycle works, where practices lose the most money, and what the difference looks like between an RCM process that performs well and one that quietly bleeds revenue every month.
Whether you are a physician trying to understand why your collections do not match your patient volume, a practice manager building a billing workflow from scratch, or an administrator evaluating whether to outsource — this is the guide you need.
What Is Revenue Cycle Management — The Simple Definition
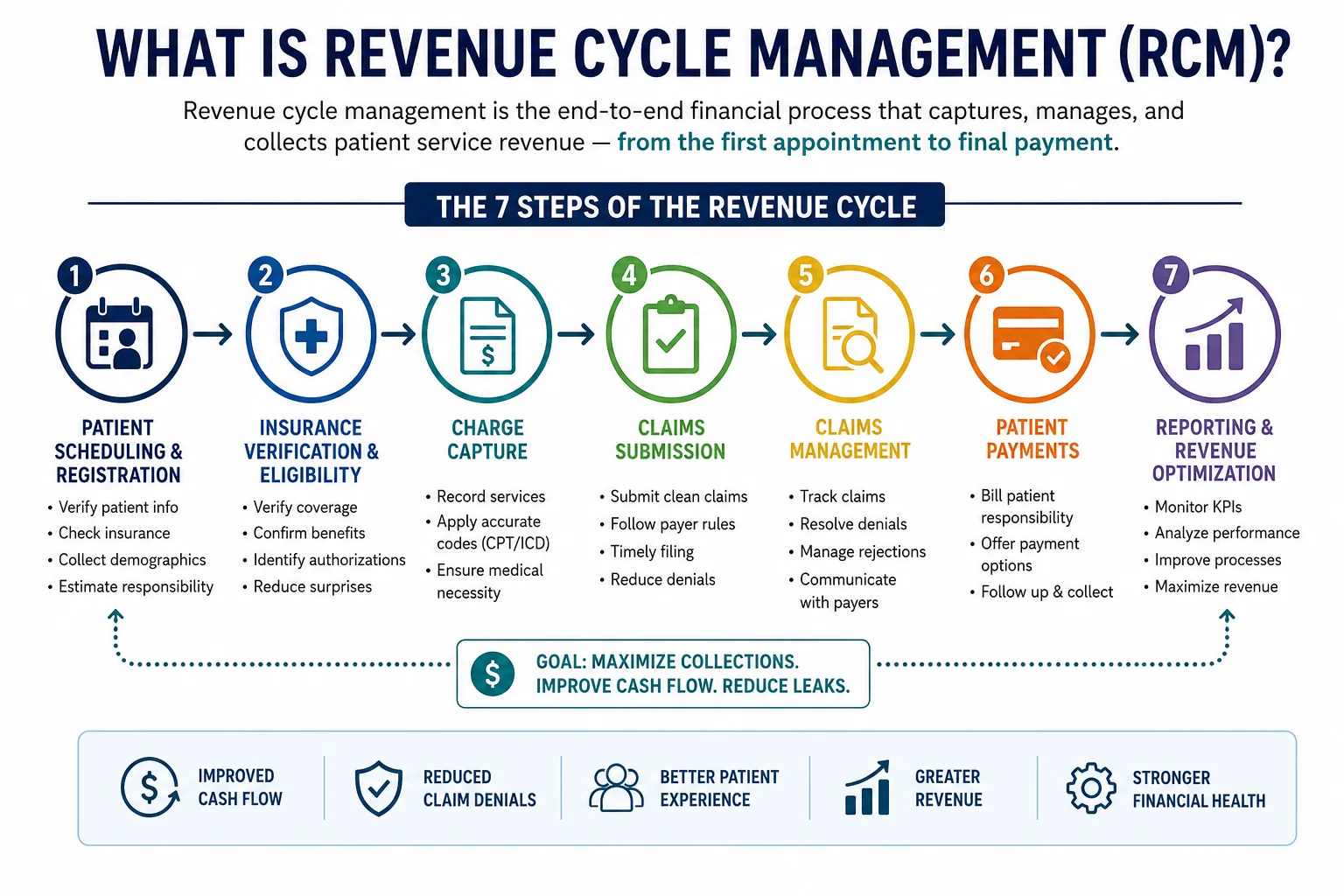
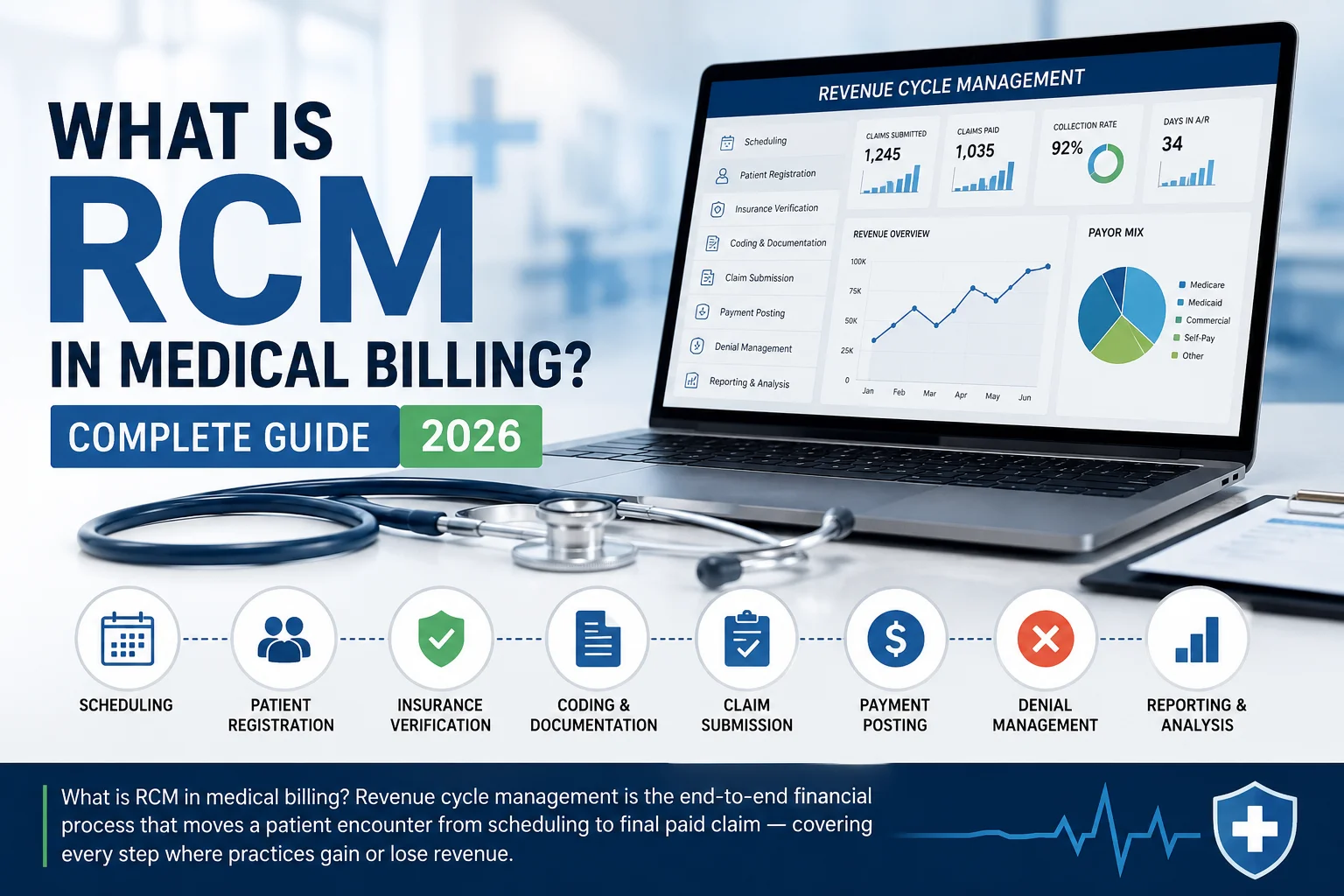
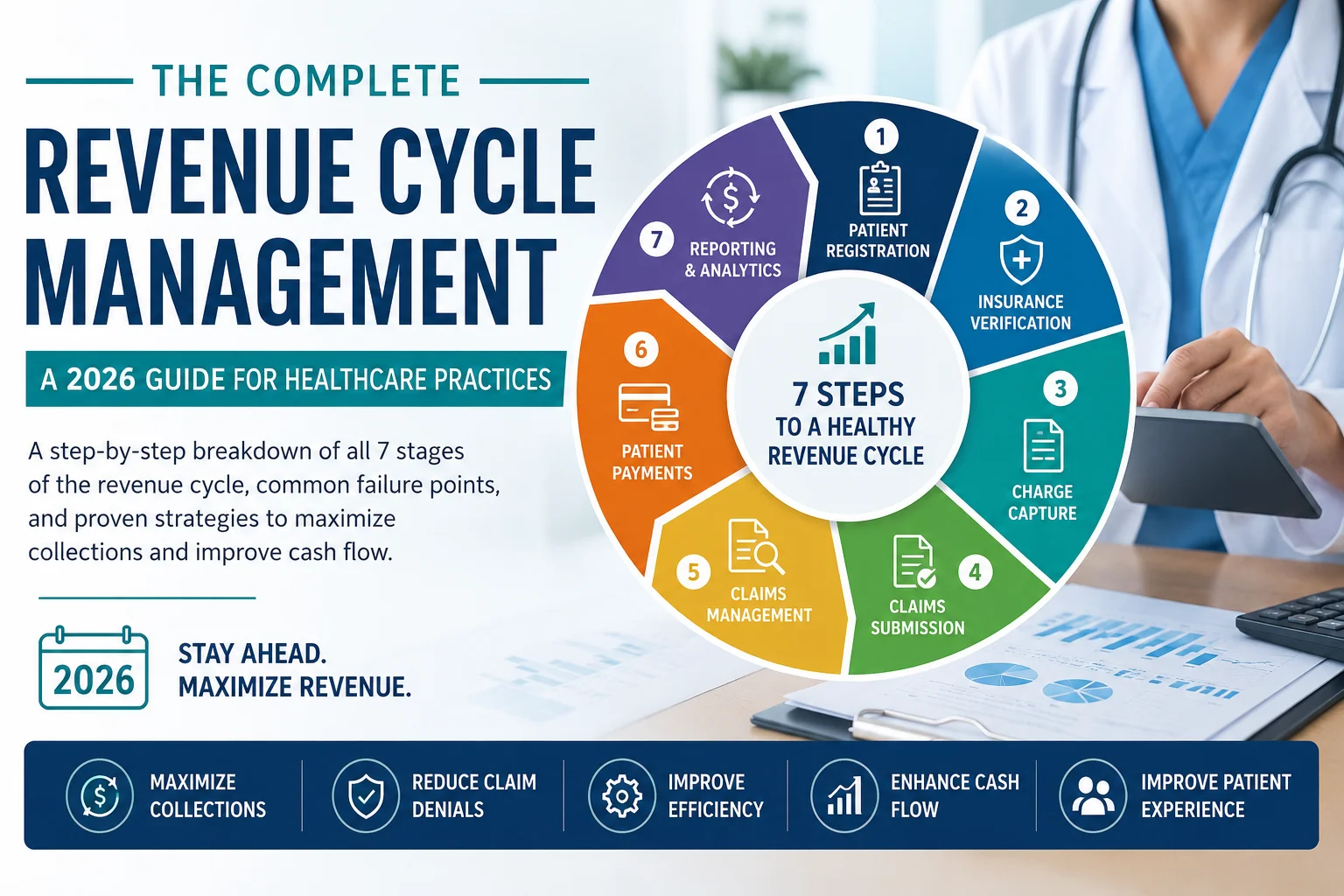
Revenue cycle management (RCM) is the end-to-end financial process that healthcare organizations use to track patient care from the initial appointment through to final payment — including every administrative and clinical function that affects revenue generation along the way.
The word “cycle” is important. This is not a linear process that starts and ends. It is a continuous loop that repeats for every patient, every visit, every service, every claim. A practice seeing 50 patients a day is running 50 simultaneous revenue cycles — each at a different stage, each with its own payer, its own authorization requirements, its own documentation, its own appeal status.
Revenue cycle management includes seven key steps: preregistration, registration, charge capture, claim submission, remittance processing, insurance follow-up, and patient collections. Each step plays a role in getting providers paid accurately and on time. Medical billing is just one part of the revenue cycle — it is mostly focused on submitting claims and posting payments.
That last point is worth emphasizing. Medical billing is a component of revenue cycle management — not the whole thing. Practices that think they have an RCM process because they have a biller are often missing five of the seven steps entirely. And the steps they are missing are usually the ones where the most money is lost.
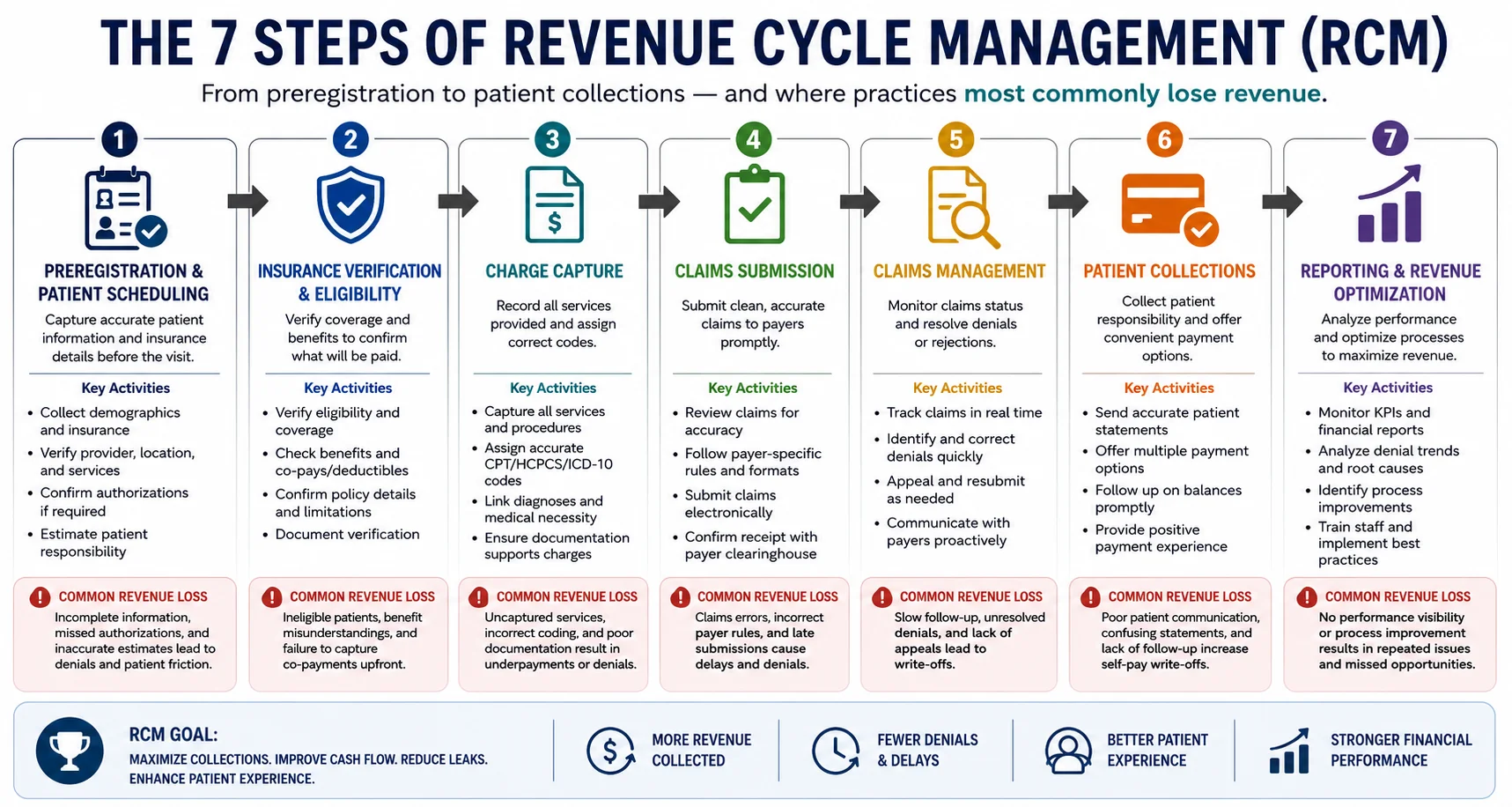
The 7 Steps of Revenue Cycle Management — Explained
Step 1 — Preregistration
Everything in the revenue cycle starts before the patient arrives. Preregistration is the process of collecting the patient’s insurance information, verifying their eligibility, identifying their benefits, and estimating their financial responsibility — all before the appointment takes place.
This step is the most undervalued in most practices — and the most expensive to get wrong. Every eligibility error that is not caught at preregistration will eventually become a denied claim. Every coverage gap that is not identified before the visit will become a patient balance dispute after the fact. Every authorization that is not obtained before a procedure will become a CO-15 denial.
What good preregistration looks like: Real-time eligibility verification — not just checking whether a patient has insurance, but confirming their specific benefits, deductible status, coinsurance, copay, and whether the service they are coming in for is covered. This happens before every appointment, every time — not just at registration for new patients.
What it costs when preregistration fails: According to CMS administrative burden research, eligibility and authorization failures at the front end of the revenue cycle account for a disproportionate share of total claim denials. Practices that run systematic preregistration catch these issues before they generate denials. Practices that skip or rush it absorb those denials downstream.
Step 2 — Registration
Registration is the formal collection and recording of patient demographic, insurance, and financial information at or before the point of service. This is where the data that will travel through the entire revenue cycle is entered — and where small errors create expensive downstream problems.
A transposed digit in a date of birth. An insurance ID entered incorrectly. A group number pulled from an expired card. Any of these generates a CO-16 denial — claim contains incorrect or missing information — when the claim hits the payer. And CO-16 is consistently the most common denial code in medical billing.
What good registration looks like: Photo ID and insurance card collected and scanned at every visit — not just at the first appointment. Insurance information verified against real-time payer records, not just what the patient reports verbally. All demographic fields confirmed and updated at each encounter.
What it costs when registration fails: CO-16 denials generated by registration errors are correctable — but they require staff time to identify, correct, and resubmit. Practices generating high volumes of CO-16 denials are paying their billing team to fix mistakes their registration team made. The fix is upstream, not in denial management.
Step 3 — Charge Capture
Charge capture is the process of translating the clinical services a provider delivered into the billable charges that will appear on the claim. It connects what happened in the exam room to what gets submitted to the payer.
This step is where undercoding most commonly occurs. A provider documents a level 3 office visit when the clinical work and documentation support a level 4 or 5. A procedure is delivered but not entered into the practice management system. A modifier that should be appended is missed. Each of these is a charge capture failure — and unlike denials, which are visible in your AR report, undercoding is invisible. The claim gets paid. Just for less than you were entitled to.
What good charge capture looks like: A structured process that connects provider documentation to charge entry with a verification step — either automated through your EHR or reviewed by a certified coder before submission. Our CodeMAXX services specifically address the charge capture and coding accuracy layer that prevents systematic undercoding.
What it costs when charge capture fails: Research cited through AHIMA consistently identifies undercoding as costing practices 6 to 9 percent of net collections. On a practice collecting $150,000 per month, that is $9,000 to $13,500 in monthly revenue loss — invisible, month after month, because the claims are getting paid.
Step 4 — Claim Submission
Claim submission is the process of transmitting a clean, correctly coded, complete claim to the appropriate payer through an electronic clearinghouse or direct payer connection. This is what most people think of when they think of “medical billing” — but it is step four of seven, not the whole picture.
A clean claim is one that passes all edits — demographic, clinical, and technical — and reaches the payer with no errors that would prevent adjudication. The percentage of claims that achieve clean submission on the first pass is your clean claim rate — the single most important performance metric in medical billing.
What good claim submission looks like: Pre-submission claim scrubbing that catches demographic errors, coding conflicts, bundling violations, missing modifiers, and authorization gaps before the claim leaves your system. Our medical billing and practice management service maintains a 98.5 percent clean claim rate — meaning 98.5 percent of claims are accepted on the first submission.
What it costs when claim submission fails: The national average clean claim rate is approximately 95 percent. The difference between 95 percent and 98.5 percent on a practice submitting $200,000 in claims monthly is $7,000 in additional clean submissions — every month — that either get paid on first pass or go into a denial queue that costs staff time and risks write-off.
Step 5 — Remittance Processing
Remittance processing is the review and posting of payments, denials, and adjustments received from payers — translating the Explanation of Benefits (EOB) or Electronic Remittance Advice (ERA) into properly balanced patient accounts.
This step is where denial codes get categorized, payment amounts get verified against contracted rates, and secondary claims get prepared. It is also where underpayments can go undetected — a payer reimbursing below the contracted rate, a payment posted to the wrong patient account, or an adjustment applied incorrectly.
What good remittance processing looks like: Every payment verified against contracted fee schedules before posting. Every denial code logged by CARC and group code. Every secondary billing trigger identified. Every underpayment flagged for follow-up. For a complete breakdown of denial codes and what they mean, see our medical billing denial codes guide.
What it costs when remittance processing fails: Underpayments that are not identified and disputed are permanent revenue losses. Denials that are not categorized correctly generate incorrect follow-up actions — billing patients for CO denials, or appealing PR denials to payers who will never change the outcome. These are costly errors that compound over time.
Step 6 — Insurance Follow-Up and Denial Management
Insurance follow-up is the proactive monitoring of outstanding claims — ensuring that every submitted claim reaches resolution within the payer’s processing timeframe, and that denied claims are appealed before their appeal windows close.
This is the step where most practices’ revenue cycles break down. Reactive denial management — waiting for a denial to arrive and then deciding whether to appeal it — is not a process. It is hope. And it consistently results in claims aging past appeal windows, high-value denials being worked while low-value denials are written off, and systematic patterns repeating month after month because nobody is feeding denial data back upstream.
The trend among top-performing practices is shifting from denial management to denial prevention. Instead of focusing on an appeals process, they are identifying issues upfront — checking eligibility in real-time, verifying code prior to submission, and analyzing claims data to determine which claim types are most likely to be denied by certain payers.
What good insurance follow-up looks like: Proactive AR aging reports that flag unpaid claims before they reach 30 days outstanding. Denial categorization by CARC and group code within 24 hours of receipt. Priority-based appeal workflows that track deadlines and dollar values simultaneously. Pattern analysis that connects denial data to upstream process failures. Our creative collection solutions are built around exactly this kind of structured denial management.
What it costs when insurance follow-up fails: About 4 in 5 medical bills contain errors costing practices billions in lost revenue annually. Practices without structured denial management write off recoverable revenue every month — not because the claims were invalid, but because nobody worked them before the appeal window closed.
Step 7 — Patient Collections
Patient collections is the final step — the process of billing, communicating with, and collecting balances owed directly by patients after insurance adjudication is complete.
In 2026, this step has grown more important than at any previous point in medical billing history. High-deductible health plans remain popular among employers, meaning more patients face significant out-of-pocket costs before insurance coverage kicks in. Point-of-service collections are becoming standard practice. Rather than sending bills after the visit, practices are collecting co-pays, deductibles, and estimated patient responsibility at check-in or check-out.
The US Consumer Financial Protection Bureau reports that approximately 100 million Americans owe a combined $220 billion in medical debt — and almost half of insured Americans report receiving unexpected medical bills.
What good patient collections looks like: Patient financial responsibility communicated before the visit — not after the bill arrives. Copays and estimated deductibles collected at time of service. Multiple payment methods available — online portal, payment plans, text-to-pay. Structured follow-up for outstanding patient balances that is firm but respectful. Our creative collection solutions address both insurance and patient balance recovery under one systematic workflow.
What it costs when patient collections fail: Patient balance write-offs have become the fastest-growing revenue leak in most practices. A practice that collects 95 percent of insurance-paid claims but only 60 percent of patient balances is losing a growing share of total revenue as HDHP enrollment continues to climb.
Why Revenue Cycle Management Fails — The 7 Most Common Breakdowns
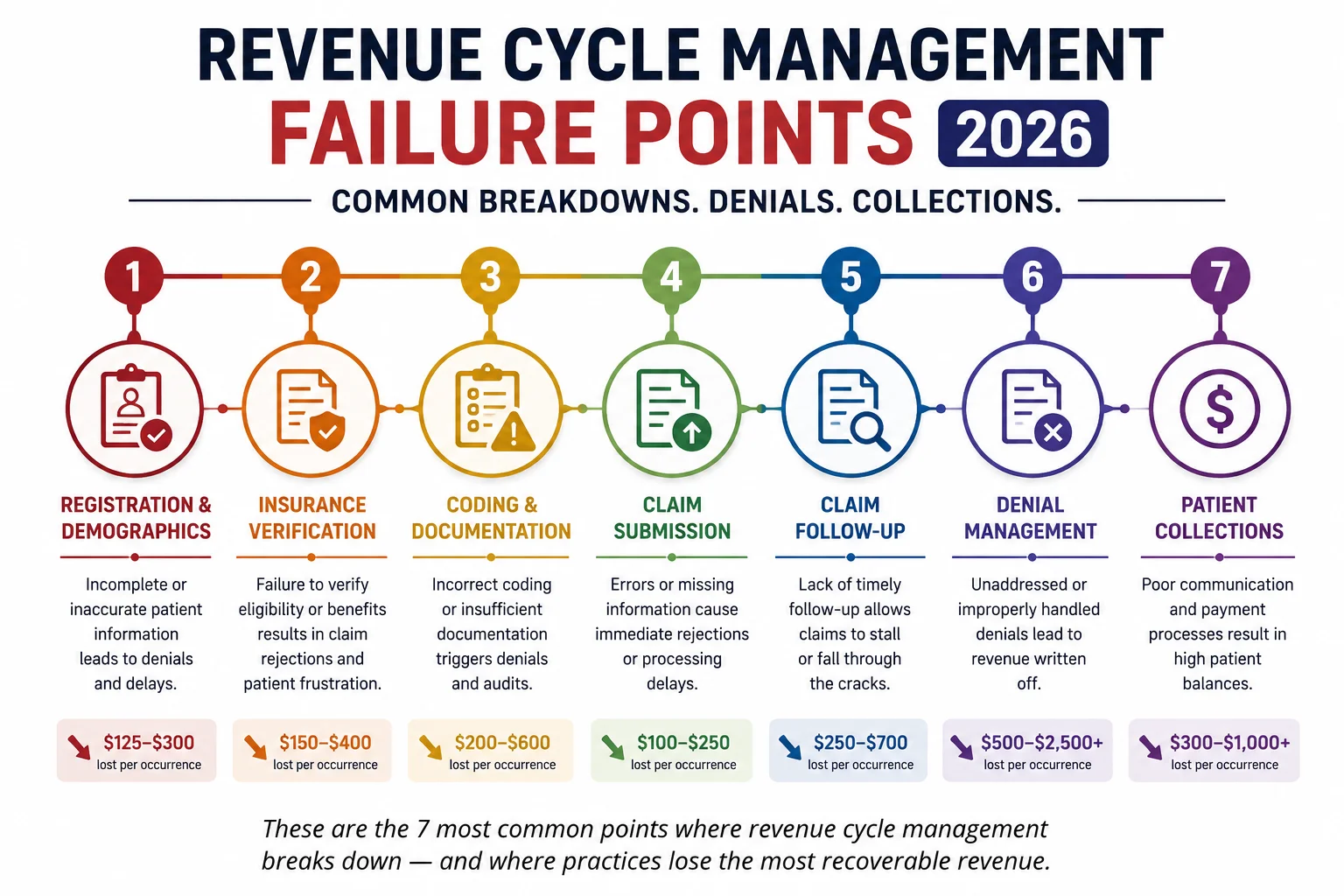
Understanding the seven steps is half the picture. Understanding where they fail — and why — is what actually protects your revenue. Here are the most common RCM breakdowns in 2026:
1. No real-time eligibility verification. Storing insurance information from the last visit and assuming it is still current is one of the most expensive habits in medical billing. Insurance changes — mid-year, mid-treatment, mid-week. Real-time verification before every appointment is the only protection.
2. Incomplete prior authorization tracking. <cite index=”66-1″>Electronic prior authorization systems are finally reaching critical mass in 2026 — but practices without systematic PA workflows are still generating CO-15 denials on services that were rendered without valid authorization.</cite> Once the service is delivered without authorization, the denial is almost always unwinnable.
3. Charge capture errors and undercoding. Undercoding is invisible until someone audits it. Most practices never do. The result is a systematic 6 to 9 percent suppression of net collections that has been running, undetected, for years.
4. No pre-submission claim scrubbing. Submitting claims without a scrubbing step is the equivalent of sending important correspondence without proofreading it. Every error that passes through becomes a denial that has to be worked downstream.
5. Reactive denial management. Working denials as they arrive, without categorization, prioritization, or pattern analysis, means the same denial types recur every month. Denial management without upstream feedback is not management — it is damage control.
6. No fee schedule auditing. Payers paying below contracted rates is more common than most practices realize — and it goes undetected when remittance processing does not include rate verification against current contracts.
7. Patient balance avoidance. Collecting patient balances after the visit is exponentially harder than collecting at the time of service. Practices that do not have point-of-service collection workflows are writing off an increasing share of patient responsibility as HDHP enrollment grows.
What Excellent Revenue Cycle Management Looks Like — The Numbers
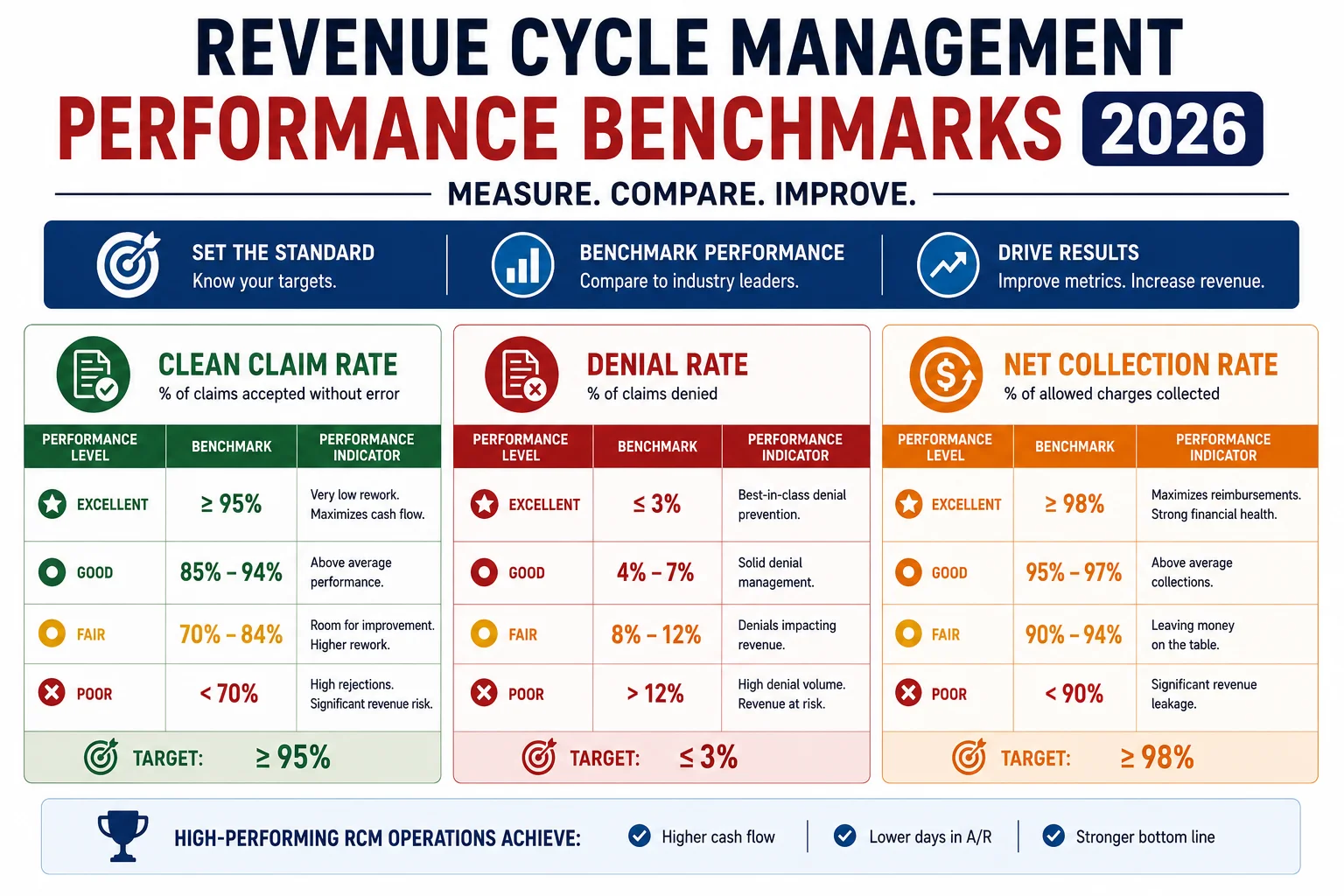
Revenue cycle management performance is measurable. Here are the benchmarks that separate high-performing RCM operations from average ones in 2026:
| Metric | Industry Average | High Performer |
|---|---|---|
| Clean Claim Rate | 85–92% | 98%+ |
| Net Collection Rate | 85–90% | 93–97% |
| Denial Rate | 11–13% | Under 3% |
| Days in AR | 40–55 days | Under 30 days |
| First Pass Resolution Rate | 70–80% | 90%+ |
| Denial Overturn Rate | 50–60% | 75%+ |
| Patient Collection Rate | 55–65% | 80%+ |
If you do not know where your practice currently sits on these metrics — that is itself a revenue cycle management problem. You cannot improve what you cannot measure. And most practices are flying blind on at least three or four of these numbers.
In-House vs Outsourced Revenue Cycle Management — What the Data Says
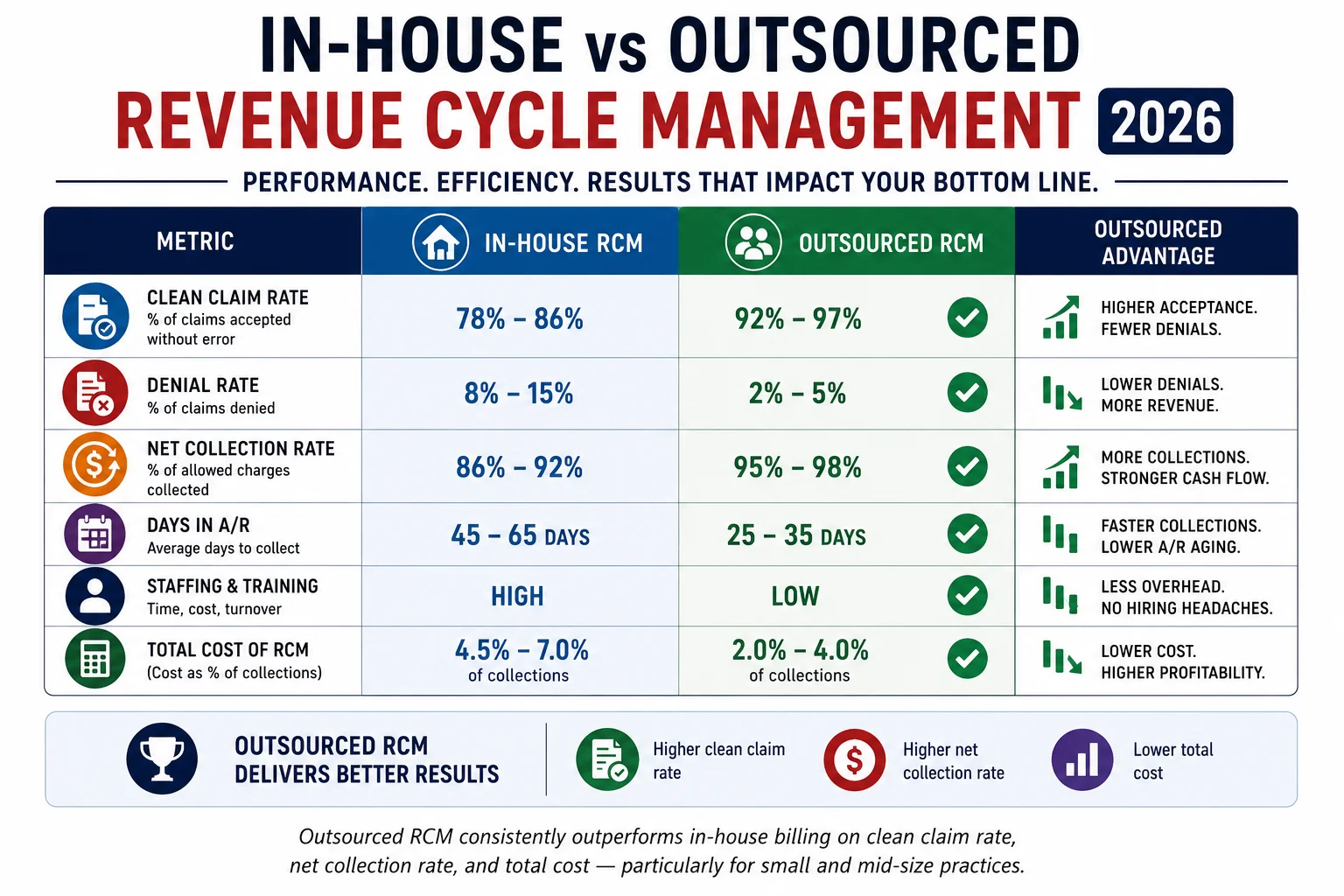
One of the most important decisions any practice makes about its revenue cycle is whether to manage it in-house or outsource it to a specialist.
More providers are choosing to outsource their billing solutions than ever before. Modern medical billing companies act as strategic partners — analyzing your performance, finding hidden revenue gaps, and addressing those gaps to target optimized revenue outcomes.
Fortune Business Insights shows that front-end billing services alone account for nearly 43.8 percent of outsourced billing demand — underscoring the growing focus on accuracy from the very start of the medical billing process.
The performance gap is real and measurable. The average in-house billing operation collects 85 to 90 percent of allowable charges. A specialist outsourced RCM partner with active denial management typically collects 93 to 97 percent. On a practice with $200,000 in monthly claims, that difference is $6,000 to $14,000 in additional revenue every month.
Many healthcare providers are adopting hybrid billing models — combining in-house teams with specialized billing partners. Outsourcing allows access to advanced technology and expertise without heavy infrastructure investment.
For a complete, honest analysis of both models — including the true cost of in-house billing that most practices underestimate — read our full guide: In-House vs Outsourced Medical Billing — Which One Makes Your Practice More Money.
Revenue Cycle Management in 2026 — What Has Changed and Why It Matters
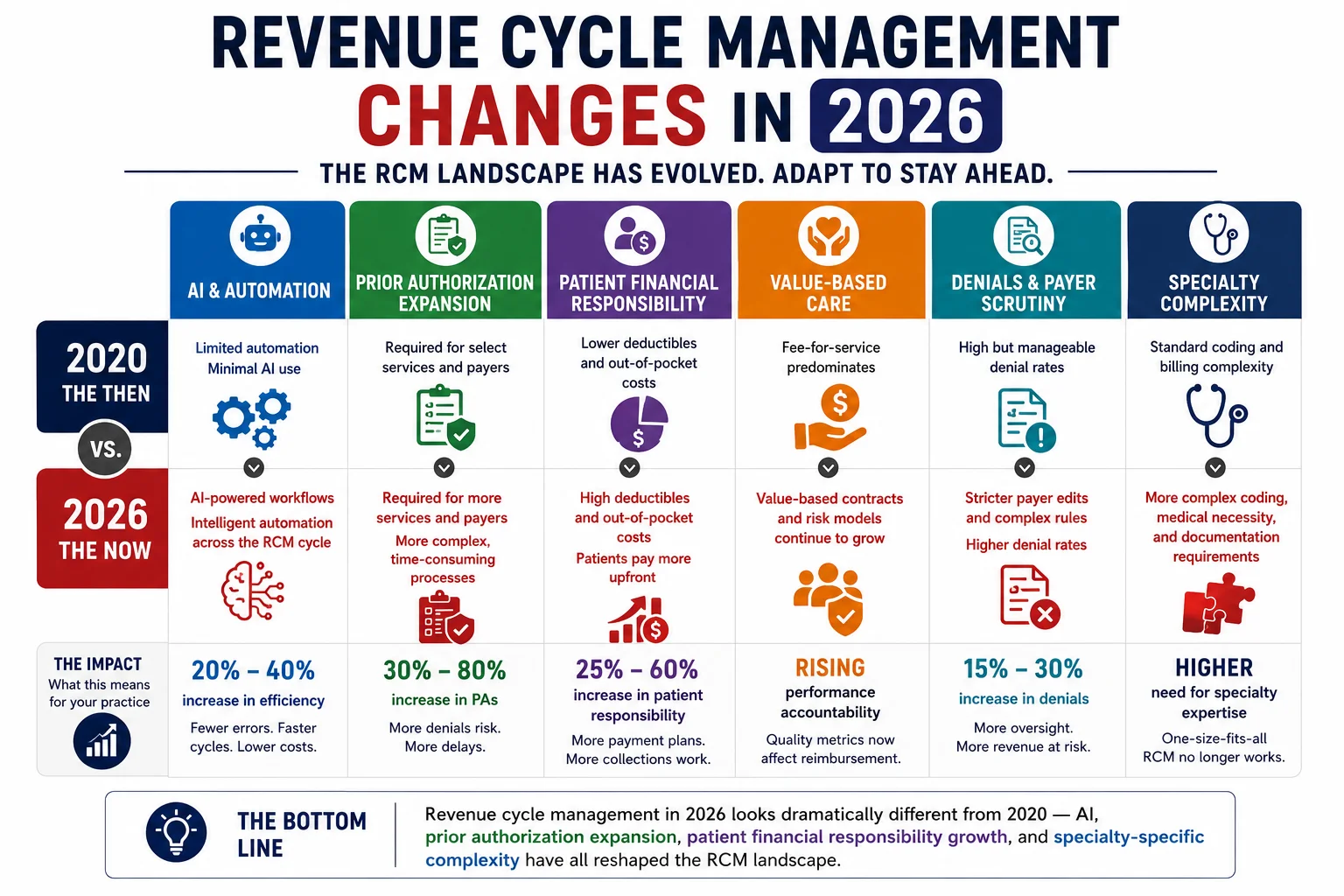
Revenue cycle management in 2026 is not the same process it was five years ago. Several forces have fundamentally changed what effective RCM requires:
AI and Automation. AI-powered RCM platforms now use predictive analytics to forecast denials, optimize coding accuracy, and recommend the best claim submission timing for faster payments. Denial prediction algorithms analyze historical claim data and payer feedback to flag high-risk claims before submission.
Prior Authorization Expansion. Physicians now spend 14.5 hours per week on prior authorization — and every practice’s RCM process must include systematic PA tracking or it will generate CO-15 denials that drain revenue continuously. For more on this, see our medical billing trends 2026 guide.
Value-Based Care Complexity. The shift from fee-for-service to value-based care continues to gain momentum. More payer contracts now include quality metrics, patient outcomes, and cost efficiency targets. Reimbursement depends not just on what services you provide, but on how well your patients do. Practices participating in value-based programs need billing partners who understand these arrangements.
CPT Code Complexity. The 2026 CPT update included 418 total changes — 288 new codes, 84 deletions, and 46 revisions. Revenue cycle management operations that do not maintain current code tables are generating automatic rejections. For full details, see our CPT code changes 2026 guide.
Cybersecurity as RCM Risk. Ransomware attacks on healthcare organizations have made cybersecurity inseparable from revenue cycle operations. A cyber attack that leads to system failure can stop claim filing and delay payments for weeks. Our HIPAA compliance services build security resilience into the billing process itself.
How Pro Health Care Advisors Manages the Full Revenue Cycle

Pro Health Care Advisors provides end-to-end, HIPAA-compliant revenue cycle management for healthcare practices across the United States. Here is exactly how we manage each step of the revenue cycle for our clients:
Preregistration and Eligibility — Real-time insurance eligibility verification before every appointment. Benefit-level checks that identify deductibles, coinsurance, copays, and coverage limitations before the patient arrives. Prior authorization tracking that confirms authorization status for every procedure that requires it.
Registration Support — Demographic verification workflows that catch the registration errors that generate CO-16 denials before they reach the claim submission stage.
Charge Capture and Coding — AAPC-certified coders review every claim for coding accuracy, diagnosis-procedure alignment, modifier use, and bundling edits before submission. Our CodeMAXX services add a dedicated coding accuracy layer that catches undercoding patterns that suppress net collections.
Clean Claim Submission — Pre-submission claim scrubbing that maintains a 98.5 percent clean claim rate — well above the 85 to 92 percent industry average.
Remittance Processing — Every payment verified against contracted fee schedules before posting. Every denial logged by CARC and group code. Underpayments flagged for contract dispute.
Denial Management and Insurance Follow-Up — Structured denial management with categorization, prioritization, and appeal workflows that maintain a denial rate under 2 percent — compared to the national average of 11 to 13 percent. Our creative collection solutions recover denied and aged claims with systematic follow-up that in-house teams cannot sustain.
Patient Collections — Structured patient billing workflows that include point-of-service collection guidance, patient balance follow-up, and payment plan management.
Physician Credentialing — Our physician credentialing service handles payer enrollment, CAQH verification, and re-credentialing management — eliminating the credentialing gaps that create billing voids for new providers.
Audit Protection — Our MD Audit Shield RAC service provides documentation review, compliance monitoring, and audit response preparation that protects your practice from RAC audit findings.
Specialties Served — We manage revenue cycles for more than 30 specialties including cardiology, family practice, mental health, wound care, and more. See our full specialties list.
For more billing education and RCM resources, visit our articles and resources library.
Frequently Asked Questions — Revenue Cycle Management 2026
Q: What is the difference between medical billing and revenue cycle management? Medical billing is one component of revenue cycle management — primarily focused on claim submission and payment posting. Revenue cycle management is the full end-to-end process covering seven steps: preregistration, registration, charge capture, claim submission, remittance processing, insurance follow-up and denial management, and patient collections. Practices that only manage the billing step are typically missing the upstream and downstream steps where the most revenue is lost.
Q: What are the 7 steps of the revenue cycle? Preregistration (eligibility verification and authorization), registration (demographic and insurance data collection), charge capture (translating services into billable charges), claim submission (transmitting clean claims to payers), remittance processing (posting payments and identifying denials), insurance follow-up and denial management (pursuing unpaid and denied claims), and patient collections (billing and collecting patient balances).
Q: What is a good clean claim rate for revenue cycle management? The industry benchmark is approximately 95 percent. The best RCM operations in 2026 operate at 98 percent or higher. Pro Health Care Advisors maintains a 98.5 percent clean claim rate. Every percentage point below 98 represents claims going into a denial queue that costs staff time, appeal resources, and write-off risk.
Q: What is a good denial rate for a medical practice? The national average initial denial rate is 11 to 13 percent. A well-performing revenue cycle should maintain a denial rate below 5 percent. The best-performing outsourced RCM operations operate below 2 percent. Pro Health Care Advisors maintains a denial rate under 2 percent.
Q: How does revenue cycle management affect patient experience? Directly and significantly. Patients who receive unexpected bills, incorrect billing statements, or confusing EOBs have worse experiences with their provider — regardless of the quality of clinical care they received. Patients today expect the same level of clarity in healthcare billing that they get from online retail or banking. A clean, transparent billing process is now part of the patient experience — and practices that do not deliver it see it reflected in reviews, referrals, and retention.
Q: How do I know if my practice’s revenue cycle management is underperforming? Start with five numbers: clean claim rate, denial rate, net collection rate, days in AR, and patient collection rate. If you do not know any of these numbers, your RCM visibility is insufficient. If your clean claim rate is below 95 percent, your denial rate is above 8 percent, your days in AR is above 40, or your net collection rate is below 90 percent — your revenue cycle has measurable performance gaps that are costing your practice money every month.
Q: Should I outsource revenue cycle management in 2026? For most small and mid-size practices — yes. The true cost of in-house RCM (including benefits, software, turnover, undercoding losses, and uncollected denials) typically runs $70,000 to $120,000 per year for a small practice. An outsourced RCM partner at 5 to 7 percent of collections with a higher clean claim rate and lower denial rate almost always generates more net revenue at lower total cost. Read our complete comparison: In-House vs Outsourced Medical Billing.
The Bottom Line — Revenue Cycle Management Is Your Practice’s Financial Engine

Here is the clearest way to think about revenue cycle management: every dollar your practice earns has to travel a seven-step journey to reach your bank account. At every step, there is a chance it falls off the track — through an eligibility error, a coding mistake, a missed authorization, a denied claim that nobody appealed, a patient balance that nobody followed up on.
The practices collecting the most revenue in 2026 are not necessarily seeing the most patients. They are simply losing fewer dollars along that seven-step journey — because their revenue cycle management process is built to catch problems at each step, not react to them after they become denials and write-offs.
That is what Pro Health Care Advisors builds for every practice we serve. A complete, HIPAA-compliant, AAPC-certified revenue cycle operation — covering all seven steps — with a 98.5 percent clean claim rate and a denial rate under 2 percent.
If you want to know where your practice’s revenue cycle stands right now — and what it would take to bring it to that performance level — the first step is a free conversation.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pressure. No pitch. Just a real look at your revenue cycle numbers and an honest conversation about what better looks like for your specific practice.