Mental Health Billing 2026: Complete CPT Code Guide, Real Medicare Rates & 10 Denial Fixes for Therapists
Picture this.
You just finished a really hard session with a patient who has been dealing with severe depression for months. You helped them make a real breakthrough today. You are tired but satisfied — this is why you got into this work.
Then you sit down to bill the session.
And that is where the dread kicks in.
Which CPT code? Was the session long enough for 90837? Did you write down the start and stop times? Will this payer require prior authorization? Did you use the right modifier for telehealth?
If that sounds familiar, you are not alone. Mental health billing is genuinely one of the most complicated corners of medical billing in the United States. Therapists, psychiatrists, counselors, and social workers lose thousands of dollars every year — not because they did anything wrong clinically, but because billing rules are complicated, payer requirements keep shifting, and one small documentation gap can flip an approved claim into a denial.
This guide fixes that. We are going to walk through every CPT code you need in 2026, what they mean, who can bill them, what Medicare pays, and — most importantly — the ten most common denial reasons and exactly how to avoid each one.
No fluff. No filler. Just the practical stuff you need to get paid for the work you are already doing.
What Makes Mental Health Billing Different from Every Other Specialty
Before we get into the codes, you need to understand the one thing that makes mental health billing structurally different from almost every other area of medicine.
Mental health codes are time-based. Almost all of them.
When a cardiologist bills for an echocardiogram, the code is based on the procedure — it does not matter much how long it took. When a surgeon bills for a knee replacement, same thing.
But when a therapist bills for a session, the entire claim rests on time. The difference between CPT code 90834 and 90837 is not a different treatment. It is not a different diagnosis. It is twelve minutes of documented face-to-face time.
Twelve minutes.
That is why a 50-minute session note that says “session completed, patient improving” can cost your practice real money. And a 53-minute session note that says “CBT session addressing panic disorder, patient demonstrated reduction in avoidance behaviors, total face-to-face time: 53 minutes” gets paid cleanly.
The documentation is not bureaucracy for its own sake. For mental health billing in 2026, the documentation is the claim.
The other complicating factor is that the same code — say 90837 — pays differently, requires different modifiers, and has different prior authorization rules depending on whether the payer is Medicare, Medicaid, or a commercial plan. Treating all three payers the same is one of the most expensive mistakes in behavioral health billing.
According to the American Medical Association’s behavioral health coding guide, understanding which provider type can bill which code — and pairing those codes with the correct diagnosis — is the foundation of a clean mental health claim.
Let us get into the codes themselves.
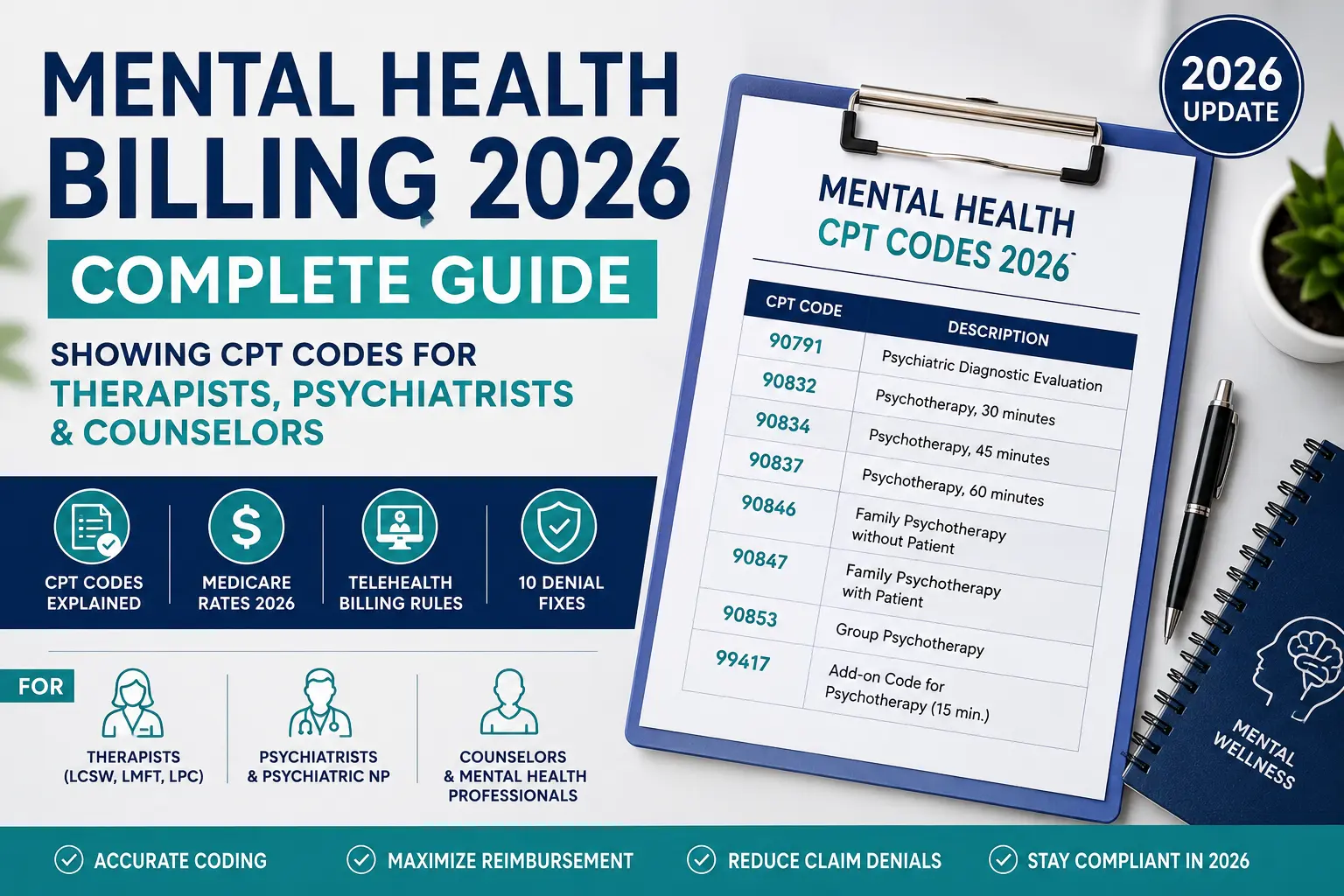
The Complete Mental Health CPT Code List for 2026
Section A — Individual Psychotherapy Codes (Time-Based)
These are the codes most therapists, counselors, psychologists, and social workers will use every single day. Every one of them is time-based, which means documented face-to-face minutes determine which code applies.
CPT 90791 — Psychiatric Diagnostic Evaluation
This is the intake code. You use it for the very first session with a new patient — the one where you are doing a full assessment, gathering history, reviewing presenting problems, and forming an initial treatment plan.
- Who can bill: Psychologists, LCSWs, LPCs, LMFTs, psychiatrists, and other licensed mental health professionals
- Time: No specific time requirement — covers a complete diagnostic evaluation
- 2026 Medicare rate: Approximately $159–$175 (varies by location)
- How often: Typically only once at the start of treatment. You can use it again if there has been a break of approximately 6 months or more, or if the patient was hospitalized for a psychiatric condition
- Documentation must include: Presenting complaint, psychiatric and medical history, mental status exam, diagnostic impressions, and initial treatment plan
CPT 90792 — Psychiatric Diagnostic Evaluation with Medical Services
Same as 90791, but this version includes medical components — physical examination, medication evaluation, prescribing, or lab orders.
- Who can bill: Psychiatrists, psychiatric nurse practitioners (PMHNPs), and other prescribers — NOT therapists or counselors who cannot prescribe
- 2026 Medicare rate: Approximately $202–$225 (varies by location)
- Important: If you are a therapist, you bill 90791. If you are a psychiatrist or PMHNP doing an intake that includes medication review, you bill 90792.
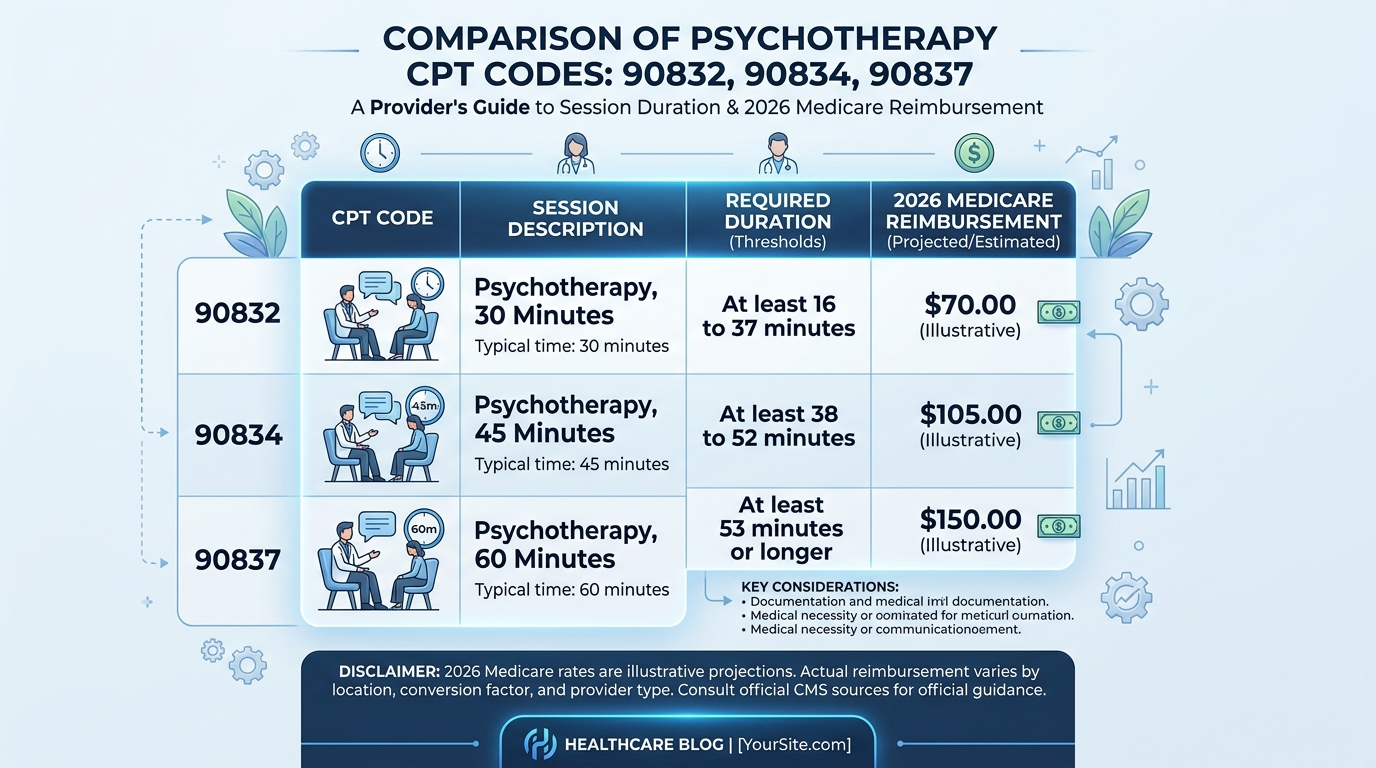
CPT 90832 — Individual Psychotherapy, 30 minutes (16–37 minutes)
The shortest standard session code. Covers sessions where the total face-to-face psychotherapy time is between 16 and 37 minutes.
- Who can bill: All licensed mental health providers
- Time range: 16–37 minutes of face-to-face therapy
- 2026 Medicare rate: Approximately $79–$81 (non-facility)
- Key rule: If your session is under 16 minutes, do not bill this code. There is no CPT code for sessions shorter than 16 minutes — those may be billed as a brief E/M service in specific circumstances, but typically should not be billed as psychotherapy
- Documentation must include: Start and stop times, specific interventions used, patient response, and progress toward treatment goals
CPT 90834 — Individual Psychotherapy, 45 minutes (38–52 minutes)
This is the most commonly billed mental health CPT code in the United States. It covers the classic 45–50 minute therapy session that most outpatient practices use as their standard appointment length.
- Who can bill: All licensed mental health providers
- Time range: 38–52 minutes of face-to-face therapy
- 2026 Medicare rate: Approximately $128–$135 (non-facility)
- Common mistake: A therapist who does 53-minute sessions and bills 90834 is actually leaving money on the table. A therapist who does 50-minute sessions and bills 90837 is upcoding — a compliance violation that RAC auditors catch
- Documentation must include: Start and stop times showing 38–52 minutes, specific therapeutic interventions, and patient progress notes
CPT 90837 — Individual Psychotherapy, 60 minutes (53+ minutes)
The code for longer, more intensive sessions. Requires documented face-to-face time of 53 minutes or more — not 52, not “about an hour.”
- Who can bill: All licensed mental health providers
- Time range: 53 minutes or more of face-to-face therapy
- 2026 Medicare rate: Approximately $176–$190 (non-facility)
- The 53-minute rule: The midpoint between 90834 (which tops out at 52 minutes) and 90837 falls at 52.5 minutes — which rounds to 53. This is not a gray area. Document exactly. If you have 52 minutes documented, you bill 90834. If you have 53 minutes, you bill 90837
- Audit risk: Consistently billing 90837 across your patient panel without corresponding documentation is one of the most flagged patterns in RAC behavioral health audits. Every 90837 claim needs airtight time documentation
Section B — Add-On Psychotherapy Codes (Used WITH Other Codes)
CPT 90833 — Psychotherapy Add-On, 30 minutes (with E/M)
This code is only for prescribers — psychiatrists, PMHNPs, and physician assistants — who conduct both medication management AND psychotherapy in the same visit.
- How it works: The prescriber bills a primary E/M code (like 99214 for the medication management portion) plus 90833 for the therapy component
- Example: A psychiatrist spends 25 minutes reviewing medications and 20 minutes doing CBT — they bill 99214 + 90833
- Critical rule: 90833 cannot be billed by therapists, LCSWs, or LPCs. It requires a primary E/M code. Billing 90833 without a primary E/M causes automatic denial
- Do not confuse with 90832: 90832 is standalone therapy. 90833 is the add-on version for prescribers in combined visits. They are never interchangeable
CPT 90836 and 90838 — Additional Add-On Codes (with E/M)
These work similarly to 90833 but cover different time ranges:
- 90836 — 45-minute psychotherapy add-on with E/M
- 90838 — 60-minute psychotherapy add-on with E/M
Same rules apply: prescribers only, always with a primary E/M code.
Section C — Group and Family Therapy Codes
CPT 90847 — Family Psychotherapy (with patient present)
Used when the therapist conducts a structured therapeutic session with the patient AND family members together.
- Time: No fixed minimum, but documentation must show a clinically meaningful session
- Patient must be present — if the family is seen without the patient, use 90846 instead
- 2026 Medicare rate: Approximately $108–$115
CPT 90846 — Family Psychotherapy (without patient present)
Same as 90847 but the patient is not in the room. Used when working with family members separately to support the patient’s treatment.
CPT 90853 — Group Psychotherapy
For structured group therapy sessions with multiple unrelated patients.
- Group size: Typically 3–12 patients. Document all participants
- Each patient is billed separately under their own claim
- 2026 Medicare rate: Approximately $31–$36 per patient
- Documentation must include: Group purpose, interventions, and each patient’s individual response and progress
Section D — Crisis Intervention Codes
CPT 90839 — Crisis Psychotherapy, first 60 minutes
Used when a patient is in acute mental health crisis — imminent risk of harm, acute suicidal ideation, psychiatric emergency requiring immediate intervention.
- Minimum time: 30 minutes to bill 90839
- Add CPT 90840 for each additional 30-minute block beyond the first hour
- 2026 Medicare rate: Approximately $205–$220 for 90839
- Audit risk: Crisis codes are among the most audited in behavioral health. Documentation must clearly show crisis-level severity, the specific interventions used, and the outcome. Routine session notes billed with crisis codes are a red flag
Section E — Telehealth Modifiers (2026 Updated Rules)
Telehealth has become a permanent part of behavioral health — and billing it correctly requires the right modifiers.
Modifier 95 — Standard telehealth modifier for real-time audio AND video sessions. Apply to any CPT code delivered via telehealth (90832–90837, 90791, 90847, 90853, etc.).
Place of Service (POS) codes for telehealth:
- POS 10 — Patient is in their private home. This reimburses at the higher non-facility rate
- POS 02 — Patient is at any other location (school, workplace, clinic). Reimburses at the lower facility rate
The $42 difference: For a 90837 session billed to Medicare in 2026, the difference between POS 10 and POS 02 is approximately $42 per session. Over a full year of sessions with multiple patients, this adds up to thousands of dollars. Document the patient’s location at the start of every telehealth session.
Audio-only sessions (phone calls): Use Modifier 93 for ongoing audio-only therapy where video is not available or appropriate. Document why video was not used and confirm patient consent to audio-only treatment is on file.
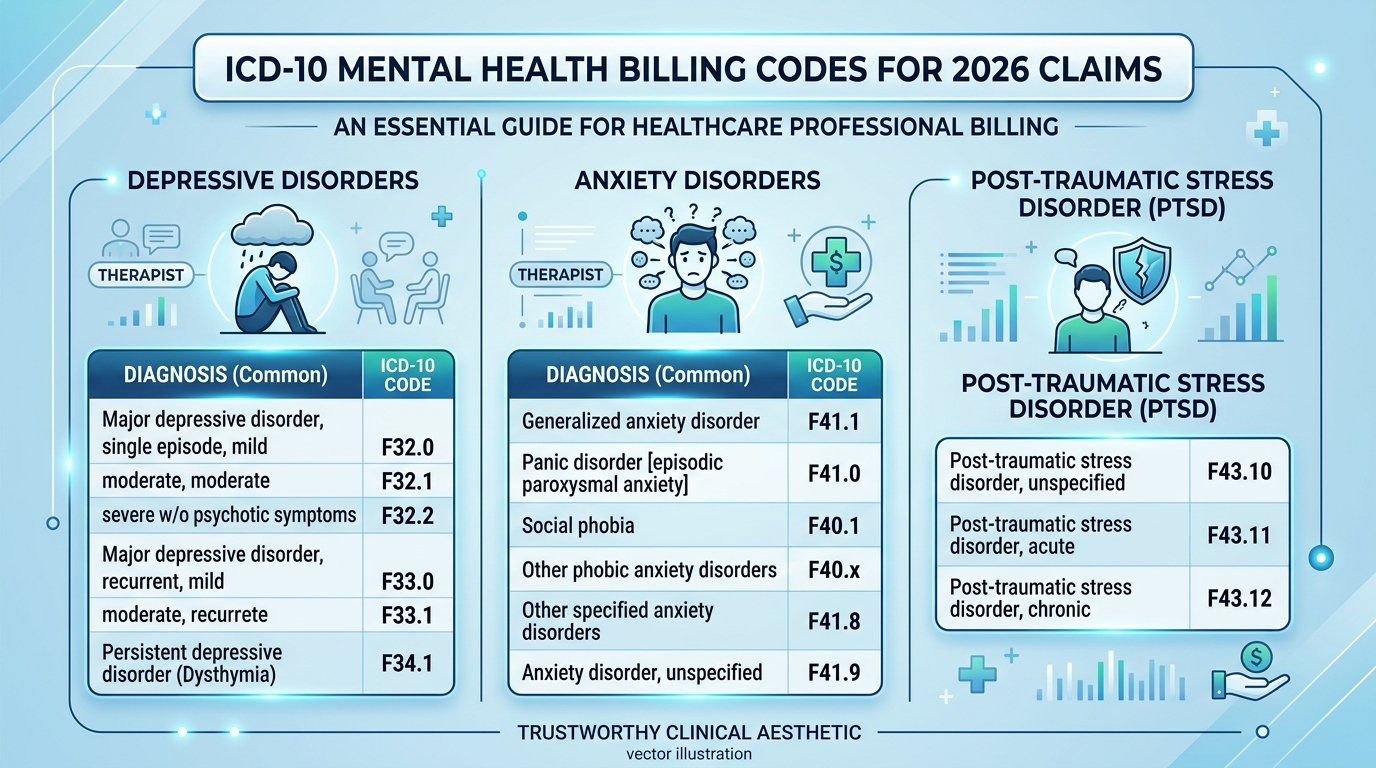
ICD-10 Diagnosis Codes — The Other Half of Every Claim
Every mental health claim needs at least one ICD-10-CM diagnosis code that establishes why the service was medically necessary. The diagnosis in the chart must match the diagnosis on the claim. If your note says “patient reports anxiety symptoms” but you code F41.1 (Generalized Anxiety Disorder), that connection must be clear and supported in your documentation.
Here are the most commonly used ICD-10 codes in mental health billing for 2026:
| ICD-10 Code | Diagnosis |
|---|---|
| F32.1 | Major Depressive Disorder, single episode, moderate |
| F33.1 | Major Depressive Disorder, recurrent, moderate |
| F41.1 | Generalized Anxiety Disorder |
| F41.0 | Panic Disorder |
| F40.10 | Social Anxiety Disorder (Social Phobia) |
| F43.10 | Post-Traumatic Stress Disorder, unspecified |
| F43.12 | PTSD, chronic |
| F90.0 | Attention-Deficit Hyperactivity Disorder, primarily inattentive |
| F84.0 | Autism Spectrum Disorder |
| F31.9 | Bipolar Disorder, unspecified |
| F20.9 | Schizophrenia, unspecified |
| F10.20 | Alcohol use disorder, moderate |
| F42.2 | Obsessive-Compulsive Disorder |
| F50.00 | Anorexia Nervosa, unspecified |
| Z03.89 | Encounter for observation — no disorder found (use for first evaluations where no diagnosis is confirmed yet) |
2026 important reminder: CMS updated ICD-10-CM codes effective October 1, 2025 — make sure your superbills and EHR system have the most current diagnosis code set. Billing with deleted or outdated codes is one of the easiest ways to generate automatic denials.
Who Can Bill Which Mental Health Codes in 2026?
This is one of the most common sources of confusion — and billing errors. Here is a clean breakdown:
| Provider Type | Can Bill These Codes |
|---|---|
| Psychologist (PhD, PsyD) | 90791, 90832, 90834, 90837, 90847, 90846, 90853, 90839 |
| Licensed Clinical Social Worker (LCSW) | 90791, 90832, 90834, 90837, 90847, 90846, 90853, 90839 |
| Licensed Professional Counselor (LPC) | 90791, 90832, 90834, 90837, 90847, 90846, 90853, 90839 |
| Licensed Marriage & Family Therapist (LMFT) | 90791, 90832, 90834, 90837, 90847, 90846, 90853, 90839 |
| Psychiatrist (MD/DO) | All of the above PLUS 90792, 90833, 90836, 90838, E/M codes |
| Psychiatric Nurse Practitioner (PMHNP) | All of the above PLUS 90792, 90833, 90836, 90838, E/M codes |
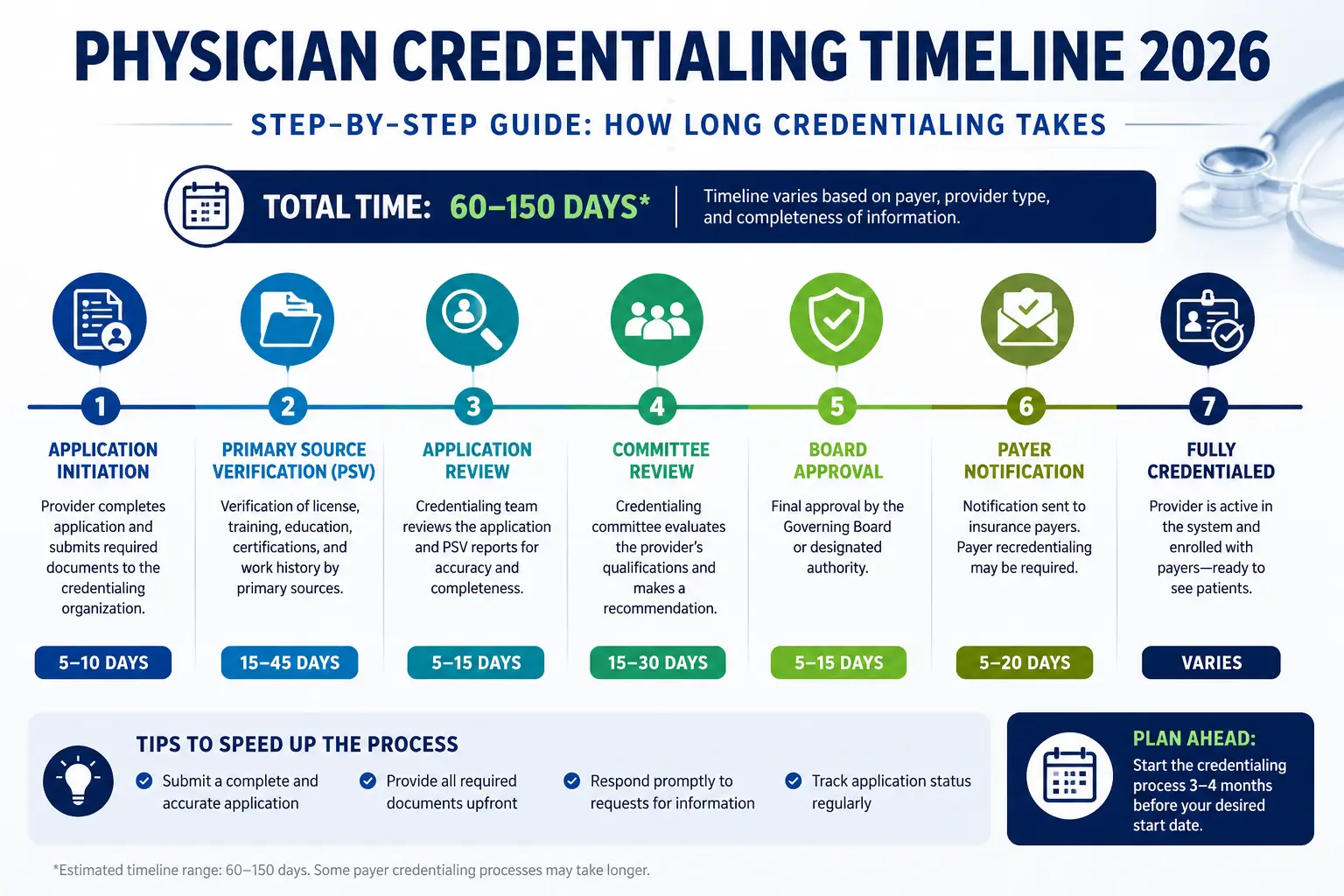
2026 update for LPCs and LMFTs: Starting January 1, 2024, Licensed Professional Counselors and Licensed Marriage and Family Therapists became recognized Medicare Part B providers. By 2026, this expansion is fully in place. If you are an LPC or LMFT who has not yet enrolled in Medicare, this is the time to do it. The process goes through CMS PECOS and typically takes 60–120 days. Our physician credentialing team handles Medicare enrollment for mental health providers across the country — contact us if you need help with the process.
Note: LPCs and LMFTs bill Medicare at 75% of the Physician Fee Schedule rate. They cannot bill E/M codes or add-on codes like 90833 that require prescribing authority.
According to the CMS Medicare coverage article for psychiatry and psychology services, each provider type has specific scope limitations that must be followed to avoid claim denials and compliance issues.
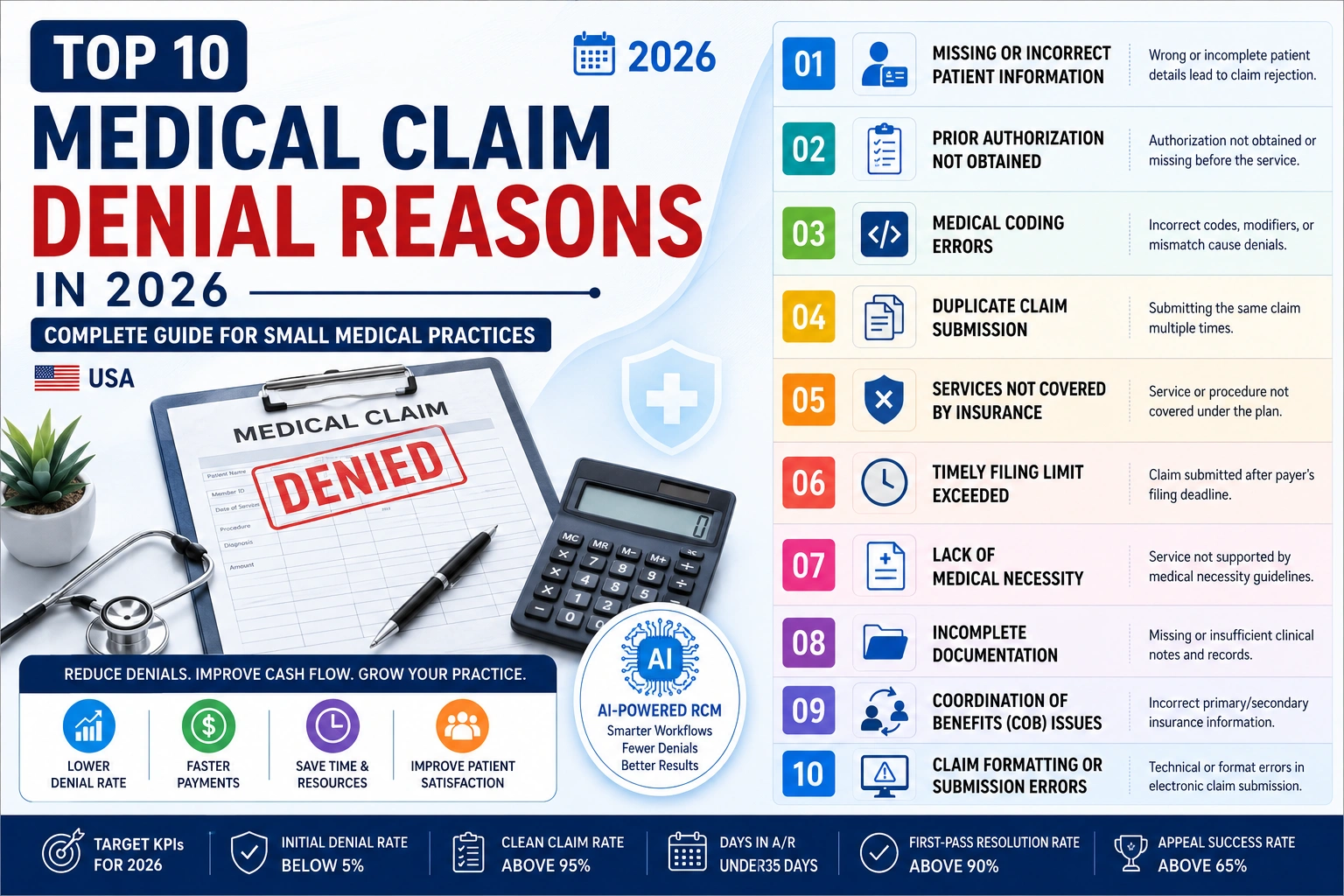
The 10 Most Common Mental Health Billing Denials — And How to Fix Each One
This is the section that will save your practice real money. These are the ten denial reasons our team sees most often when working with mental health practices across the country.
Denial #1: Missing Start and Stop Times
This is the single most common denial reason in mental health billing — and the most preventable.
Because psychotherapy codes are time-based, the documentation must show exactly when the session started and when it ended. A note that says “45-minute session” without specific clock times is not sufficient for most payers, and it is completely unacceptable for a RAC audit.
Fix: Make start and stop times the first thing you write in every session note. Literally the first line. “Session: 2:00 PM – 2:52 PM.” Everything else flows from there.
Denial #2: Upcoding — Wrong Code for Documented Session Length
Billing 90837 for a session documented as 50 minutes. Billing 90834 for a session documented as 35 minutes (that would be 90832). The code must match the documented time exactly.
Fix: Put a reference card at your desk:
- 16–37 minutes = 90832
- 38–52 minutes = 90834
- 53+ minutes = 90837
Check before you bill. Every time.
Denial #3: Incorrect Add-On Code Usage
Billing 90833 without a primary E/M code. Billing 90833 as a therapist who cannot prescribe. Billing both 90834 and 90833 in the same claim (they cannot be combined — it is one or the other).
Fix: Add-on codes (90833, 90836, 90838) are only for prescribers (psychiatrists, PMHNPs) and must always be paired with a primary E/M code. If you are a therapist, your standalone code is 90832, 90834, or 90837.
Denial #4: Diagnosis Code Does Not Support Medical Necessity
The ICD-10 code on the claim does not match what is in the clinical notes. Or the diagnosis code is too vague to establish why ongoing psychotherapy is needed.
Fix: Before billing, cross-check the ICD-10 code against the session note. The note must clearly state the diagnosis, the symptoms, and why therapy is the appropriate treatment. Codes like F41.9 (Anxiety disorder, unspecified) are technically valid but are flagged more often than specific diagnoses. Use the most specific code that is supported by your documentation.
Denial #5: Prior Authorization Not Obtained
Many commercial payers and some Medicaid plans require prior authorization for therapy beyond a certain number of sessions — sometimes as few as 8. Billing session 9 without renewing authorization results in automatic denial.
Fix: At intake, verify the patient’s mental health benefits, including whether prior auth is required and how many sessions are approved. Track authorization limits in your scheduling system and initiate renewal at least 2 sessions before the approved number runs out.
Denial #6: Billing 90791 Multiple Times Without a Break in Treatment
Using the intake/evaluation code 90791 repeatedly for established patients who have been in continuous treatment. Most payers only allow this code once at the start of treatment, or after a significant break of approximately 6 months.
Fix: Once the initial intake is done, switch to the appropriate ongoing therapy codes (90832, 90834, 90837). Reserve 90791 for new patients or patients returning after a long absence.
Denial #7: Telehealth Modifier Missing or Wrong
Billing telehealth sessions without the required Modifier 95. Using the wrong Place of Service code (which affects reimbursement rate). Not documenting the patient’s location at the time of the session.
Fix: For every telehealth session, confirm:
- Modifier 95 is on the claim
- POS code is correct (10 for home, 02 for other locations)
- Patient location is documented in the session note
- Consent for telehealth is on file
Denial #8: Group Therapy Documentation Missing Individual Progress
Billing 90853 for group therapy but only documenting the group topic — without any note of what happened specifically for each individual patient.
Fix: Group session notes need two layers: the group content (what was discussed, what interventions were used) AND an individual note for each patient (their participation, their response, their progress toward their specific treatment goals). One group note covering all patients is not sufficient for most payers.
Denial #9: Timely Filing Deadline Missed
Claims submitted after the payer’s timely filing window. Medicare requires claims within 12 months of the date of service. Most commercial payers require 90–180 days. Missing these deadlines results in denial with no right to appeal.
Fix: Bill within 30 days of every session. Do not let claims age. If you are managing a backlog, get professional billing support immediately. Aged claims are lost revenue that cannot be recovered after the filing window closes.
Denial #10: Insurance Eligibility Not Verified at Each Visit
Patient’s mental health coverage changed — they switched employers, their plan changed, their behavioral health carve-out plan is different from their medical plan. You billed the wrong payer and got denied.
Fix: Verify eligibility before every session, not just at intake. Mental health benefits are frequently carved out to separate administrators (Optum, Beacon Health, Magellan). The medical insurance card the patient shows you may not be the payer for mental health. Always call or use a verification portal to confirm behavioral health coverage specifically.
This is one area where working with a professional medical billing team makes a direct financial difference — we catch these eligibility issues before the claim is submitted, not after the denial arrives.
Mental Health Parity — Your Legal Right to Fair Reimbursement
A lot of mental health providers do not know this, but federal law is on their side.
The Mental Health Parity and Addiction Equity Act (MHPAEA), enforced by CMS, requires that insurance plans offering mental health and substance use disorder benefits cannot impose more restrictive limitations on those benefits than they apply to medical and surgical benefits.
What this means practically:
- If a plan covers unlimited physical therapy visits, it cannot cap therapy sessions at 20 per year
- If prior authorization is not required for cardiology, it cannot be required only for mental health without justification
- If a plan pays 80% for a primary care visit, it should pay the same rate for a therapy session
Parity violations are real, and they are more common than most providers realize. If you are seeing consistent denials or unusually low reimbursement rates for mental health services compared to medical services in the same plan, it may be worth investigating whether the payer is in compliance with MHPAEA.
This is also why proper HIPAA compliance and documentation practices matter — they protect you when you need to challenge payer decisions.
According to SAMHSA, nearly 1 in 5 Americans lives with a mental illness, and the demand for behavioral health services continues to grow. That demand should translate into revenue for the practices providing those services — and clean billing is how you make sure it does.

The Mental Health Billing Documentation Checklist — Print This Out
Use this checklist before submitting any mental health claim. If any item is missing, the claim is at risk.
For Every Session:
- Session start time documented (exact clock time)
- Session end time documented (exact clock time)
- Total face-to-face minutes calculated and match CPT code selected
- Patient present confirmed (required for most therapy codes)
- Specific therapeutic interventions documented (not just “therapy session”)
- Patient’s response to interventions documented
- Progress toward treatment plan goals documented
- At least one ICD-10 diagnosis code that matches the clinical note
- Provider credentials/signature present
- Consent for treatment on file
For Telehealth Sessions — Additional Requirements:
- Patient location documented (home = POS 10; other = POS 02)
- Technology platform documented (must be HIPAA-compliant)
- Consent for telehealth on file
- Modifier 95 on the claim
- Reason for audio-only documented (if video was not used)
Before Submitting Each Claim:
- Patient’s behavioral health insurance verified for this date of service
- Prior authorization confirmed and within approved session count
- CPT code matches documented session length
- ICD-10 code is current and specific
- Timely filing window is still open
How Pro Health Care Advisors Helps Mental Health Practices Get Paid
Mental health billing is our specialty — not a side service.
At Pro Health Care Advisors, we work with therapists in private practice, group practices, psychiatry offices, and behavioral health centers across the country. We understand the unique pressures mental health providers face: high session volume, complex time-based coding, payer-specific rules, frequent prior auth requirements, and the very personal nature of the work itself.
Here is what our mental health billing service includes:
Eligibility Verification Before Every Session We verify behavioral health benefits — not just medical coverage — before each appointment. We check session limits, prior auth status, copays, and whether the plan uses a carve-out administrator.
Accurate CPT Code Review Our coders review the documented session time and select the correct CPT code for every claim. No upcoding risk. No underpayment from missed add-on codes.
Prior Authorization Management We track authorization limits and initiate renewals proactively — before the approved sessions run out and before a single claim gets denied.
Denial Management and Appeals When a claim is denied, we do not just resubmit and hope. We identify the exact denial reason, fix the root cause, and build the appeal with the documentation the payer actually needs.
RAC Audit Protection Through our MD Audit Shield program, we monitor your claim patterns for audit triggers and help you maintain documentation standards that hold up to CMS scrutiny.
Provider Credentialing If you need to add a new therapist or counselor to your insurance panels — including Medicare enrollment for LPCs and LMFTs — our credentialing team handles the entire process.
You went into mental health care to help people. You should not have to spend your evenings battling billing denials. Contact our team today and let us handle the billing so you can focus on the patients who need you.
Frequently Asked Questions About Mental Health Billing in 2026
Q: What is the most commonly billed mental health CPT code?
A: CPT 90834 is the most frequently billed mental health CPT code in the United States. It covers 38 to 52 minutes of individual face-to-face psychotherapy — the standard session length for most outpatient practices. Medicare pays approximately $128–$135 for 90834 in a non-facility setting.
Q: How do I know whether to bill 90834 or 90837?
A: It comes down entirely to documented face-to-face time. If you documented 38 to 52 minutes, bill 90834. If you documented 53 minutes or more, bill 90837. If you documented 37 minutes or less, bill 90832. Always document start and stop times, not just total duration.
Q: Can LPCs and LMFTs bill Medicare in 2026?
A: Yes. Licensed Professional Counselors and Licensed Marriage and Family Therapists became eligible Medicare providers starting January 1, 2024. By 2026 this expansion is fully implemented. They bill at 75% of the Medicare Physician Fee Schedule rate and must enroll through PECOS or the CMS-855I form. They cannot bill E/M codes or prescribing add-on codes like 90833.
Q: What is a behavioral health carve-out, and how does it affect billing?
A: A carve-out means the insurance plan separates mental health and substance use benefits from the main medical benefits and administers them through a separate company — often Optum, Beacon Health Options, or Magellan Health. This means the mental health payer is different from the medical payer, even if the patient has only one insurance card. Always verify behavioral health coverage specifically before billing.
Q: How many group therapy patients can I bill for in one session?
A: CPT 90853 (group psychotherapy) is billed separately for each patient in the group. So if you have 8 patients in a group session, you submit 8 separate claims — one per patient. Each claim needs individual documentation for that patient, plus the general group session note.
Q: What modifier do I use for mental health telehealth sessions?
A: Modifier 95 is the standard telehealth modifier for 2026. Apply it to any psychotherapy CPT code delivered via real-time audio and video. For the Place of Service code, use POS 10 if the patient is at home, or POS 02 if at any other location. For audio-only sessions, use Modifier 93 and document why video was not used.
Q: What is a superbill and do I need one?
A: A superbill is a detailed receipt that lists the services provided, CPT codes, diagnosis codes, provider information, and practice details. It is used when patients pay out of pocket and then seek reimbursement from their own insurance. For practices that see self-pay patients or work with out-of-network insurers, clean superbills are essential. Our medical coding service can help you build accurate, compliant superbills.
Q: How far back can a RAC audit review my mental health claims?
A: Recovery Audit Contractors can review claims up to 3 years from the date of service. This is why maintaining detailed, accurate documentation for every session — including start and stop times — is not optional. It is your protection against future audit findings. If you want to understand your current audit risk, contact our team for a free billing review.