Medical Billing Trends 2026 — 10 Shifts Every Practice Must Act On Right Now
Something fundamental shifted in medical billing this year.
It is not one thing. It is ten things happening at the same time — and if you are running a medical practice, every single one of them is quietly affecting how much of your earned revenue you actually collect.
Medical billing is changing faster than at any point in the past decade. Technology, regulation, and patient expectations are all pushing the industry in new directions. Practices that stay ahead of these changes will thrive. Those that ignore them will struggle.
That is not an exaggeration. The practices growing their revenue right now are not necessarily seeing more patients. They are collecting more of what they are already owed — because they understand the landscape they are operating in and they have adapted their billing workflows to match it.
This guide covers the 10 most important medical billing trends in 2026 — what is happening, why it matters, what it costs practices that are not paying attention, and what you can do about it today.
Trend 1 — AI Is Now Running the Revenue Cycle, Not Just Assisting It
A few years ago, “AI in medical billing” meant a chatbot that answered FAQs. In 2026, that definition is completely obsolete.
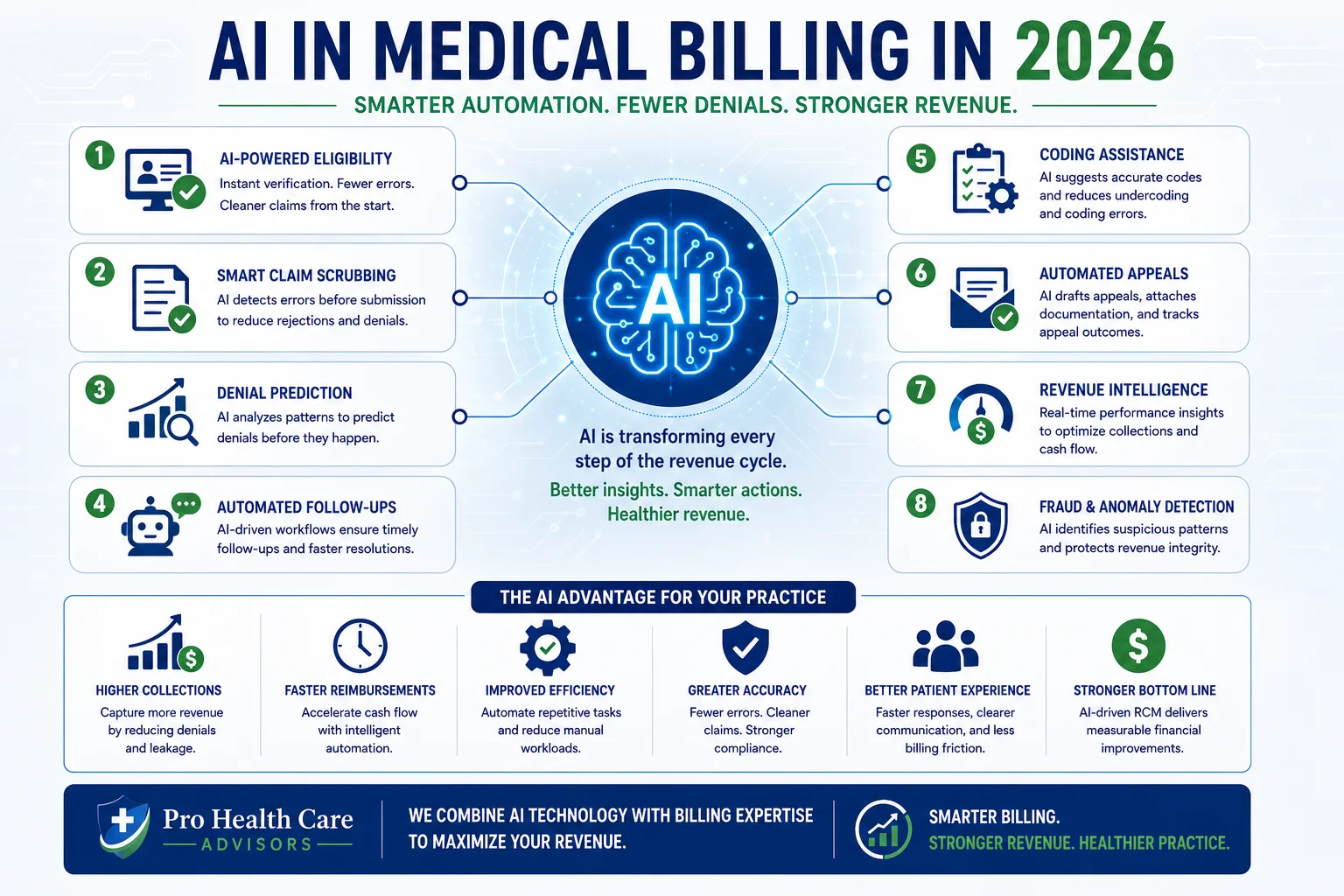
Artificial intelligence in medical billing is no longer limited to a single context. In 2026, it is actively reshaping how revenue cycles operate at every stage — from eligibility verification before a patient walks in, to denial pattern detection before claims go out, to automated follow-up on unpaid accounts.
AI-powered revenue cycle management uses machine learning to automate eligibility verification, claim scrubbing, denial prediction, prior authorization documentation, and patient collections across the billing workflow.
According to Guidehouse research, investments in medical billing automation — including AI-powered coding support, payer analytics, and prior authorization tools — ranked as the top RCM priority for medical groups in 2026.
Machine learning algorithms can now predict which claims are likely to be denied before submission. They can identify coding errors, flag missing documentation, and suggest corrections. Some systems are using AI to automate appeals — analyzing successful appeal letters and payer response patterns to generate appeal language that has a higher chance of overturning denials.
What this means for your practice: If your billing operation — in-house or outsourced — is not using AI-assisted claim scrubbing and denial prediction tools, you are operating at a structural disadvantage against every practice that is. The efficiency gap between practices with and without automation continues to widen.
Our medical billing and practice management services incorporate AI-assisted claim review as part of our standard billing workflow — catching errors before submission rather than managing denials after the fact.
Trend 2 — Prior Authorization Is Now the Biggest Single Revenue Threat
This is the number that should stop every practice owner in their tracks.
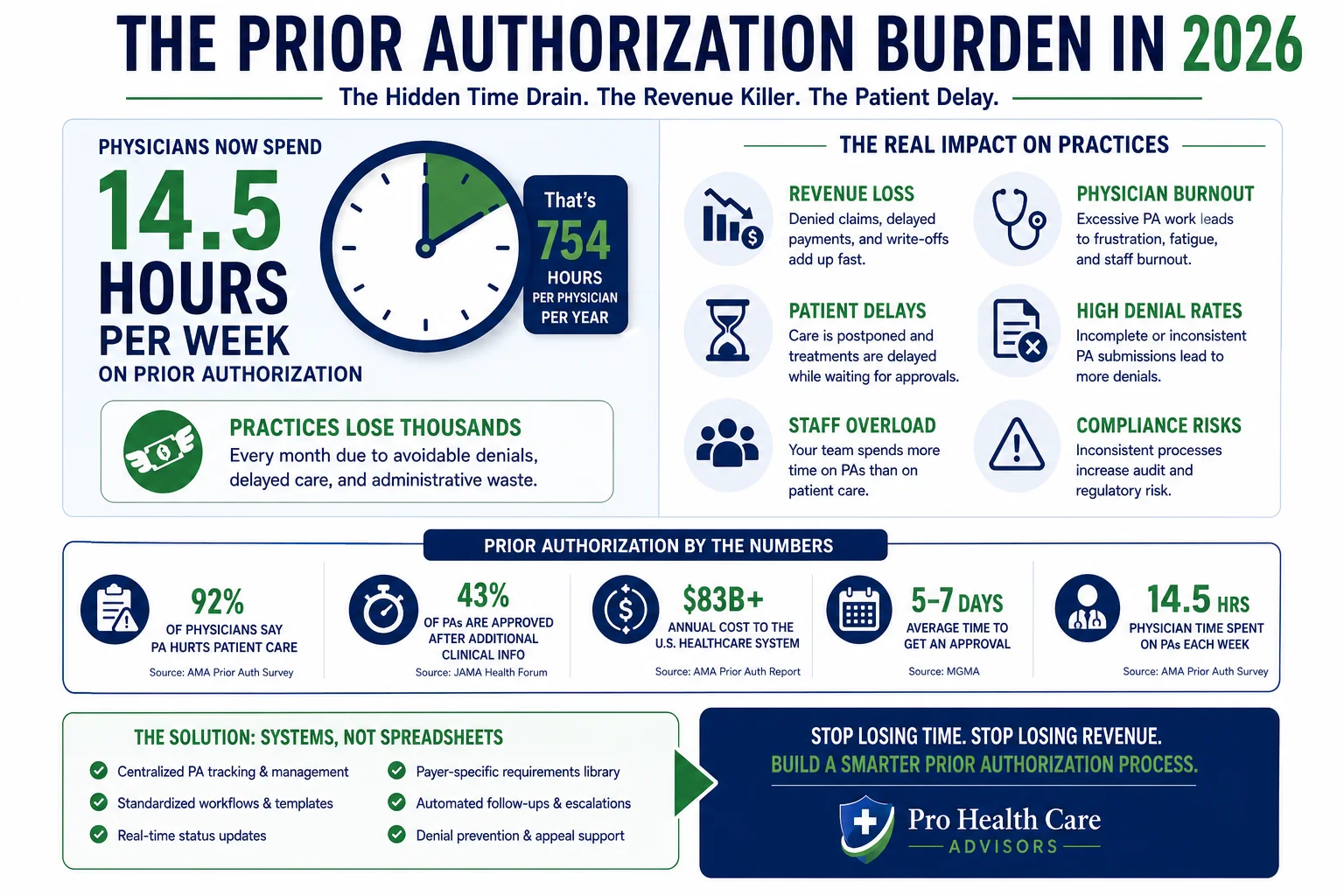
Physicians and their staff now spend an estimated 14.5 hours per week on prior authorizations alone — time taken directly from clinical care and practice operations. The American Medical Association reports that nearly 39 prior authorizations per physician per week are now required — and that prior authorization administrative overhead costs tens of billions of dollars annually across the US healthcare system.
One of the most frustrating medical billing trends in 2026 is the dramatic expansion of prior authorization requirements across payers and specialties. Medicare Advantage plans, commercial carriers, and Medicaid managed care organizations have all expanded their PA requirements in the past two years — and practices that do not have systematic authorization tracking workflows in place are generating a stream of CO-15 denials that quietly drains revenue month after month.
There is a small piece of good news inside this trend. Electronic prior authorization systems are becoming essential rather than optional in 2026. Some payers are offering real-time authorization for certain services, making approvals nearly instantaneous for practices with the right systems in place. CMS also launched WISeR — Wasteful and Inappropriate Service Reduction — a Center for Medicare and Medicaid Innovation pilot in January 2026 that uses AI-supported prior authorization for select procedures.
What this means for your practice: Prior authorization management is no longer a task your front desk handles between phone calls. It is a clinical-revenue process that requires dedicated workflows, tracking systems, and expertise in payer-specific authorization rules. Practices that treat it as anything less are absorbing avoidable revenue losses every month.
For more on how prior authorization denials translate into specific billing codes and what to do about them, see our complete guide to medical billing denial codes.
Trend 3 — Patient Collections Are Now a Bigger Challenge Than Insurance Collections
Ten years ago, billing meant submitting claims to insurance and waiting for payment. Patient balances were a small, manageable afterthought.
In 2026, that model has been turned upside down.
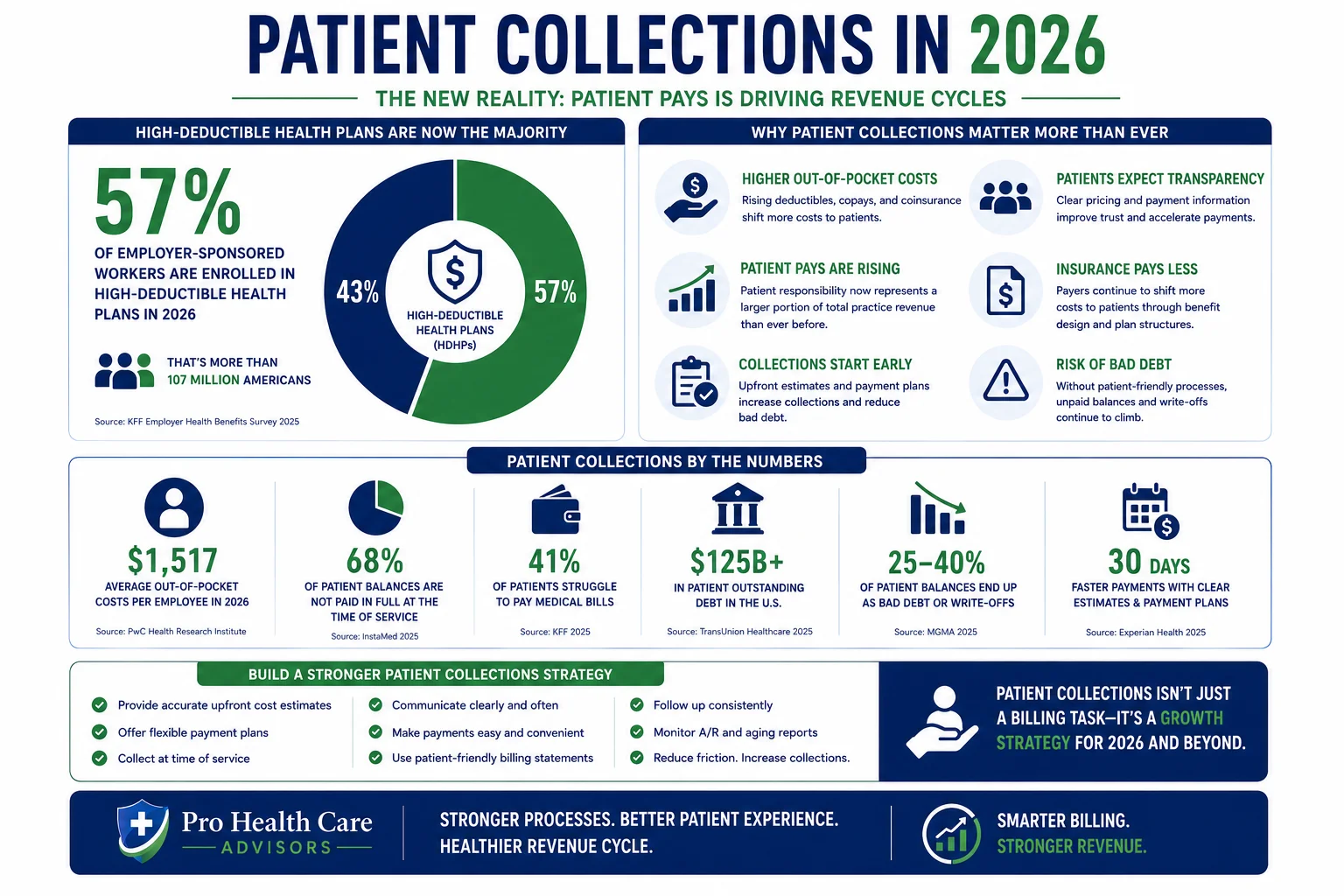
High-deductible health plans now cover more than 57 percent of employer-sponsored insured workers — making patient collections a larger share of the revenue cycle than ever before. High-deductible health plans have shifted more payment responsibility to patients. Collecting from patients is now a larger part of the revenue cycle than it was a decade ago. This trend shows no signs of reversing.
The numbers behind this trend are sobering. The US Consumer Financial Protection Bureau reports that approximately 100 million Americans owe a combined $220 billion in medical debt. Almost half of insured Americans report receiving unexpected medical bills — and approximately 1 in 5 people received a bill they disagreed with or could not afford.
What does that mean for your practice? It means that collecting from your patients is now as important — and often more difficult — than collecting from their insurance carrier. And practices that have not updated their patient billing workflows to reflect this reality are absorbing preventable collection losses every month.
Payment plans, financing options, and point-of-service collection are becoming essential. Clear communication about costs and easy payment methods improve collection rates. The practices that succeed in this environment make it easy for patients to pay. Online payment portals, text-to-pay options, and automated payment plans remove friction from the collection process.
What this means for your practice: Patient financial responsibility conversations need to happen before the visit — not after the EOB arrives. Collect estimated patient responsibility at time of service. Offer multiple payment methods. And build a structured follow-up process for outstanding patient balances. Our creative collection solutions address both the insurance and patient collection sides of your revenue cycle.
Trend 4 — Specialty-Specific RCM Is No Longer Optional
A critical medical billing trend in 2026 is the growing recognition that generalist billing knowledge is no longer sufficient. Different specialties face dramatically different billing challenges — from prior authorization requirements to specialty-specific coding rules.
For specialty practices including orthopedics, pain management, anesthesia, behavioral health, ambulatory surgery centers, and cardiology even minor shifts in reimbursement policy can directly affect cash flow, denial rates, and days in accounts receivable.
Back-office friction shows up wherever ownership is unclear and information is moving too slowly. Eligibility questions bounce between roles. Authorizations are handled differently by site. Documentation queries interrupt clinic flow because they arrive in inconsistent formats. Payer follow-up spills into nurses or front-desk staff because there is no single intake path.
The practices suffering most from this trend are those using a general billing service or generalist in-house billers for specialty work. A biller who does not understand cardiology-specific modifier rules, or behavioral health documentation requirements under CalAIM, or wound care Medicare coverage policies — will generate a consistent stream of specialty-specific denials that a specialist biller would never produce.
What this means for your practice: Verify that your billing company — or your in-house team — has specific, documented experience in your specialty. Ask for your specialty’s denial rate specifically, not just the overall practice denial rate. We serve more than 30 specialties at Pro Health Care Advisors — including cardiology, mental health, family practice, and wound care — with AAPC-certified billers who know each specialty’s specific payer requirements.
Trend 5 — Cybersecurity Is Now a Revenue Cycle Issue, Not Just an IT Issue
If cybersecurity still feels like an IT department problem to you, 2026 is the year that perception needs to change.
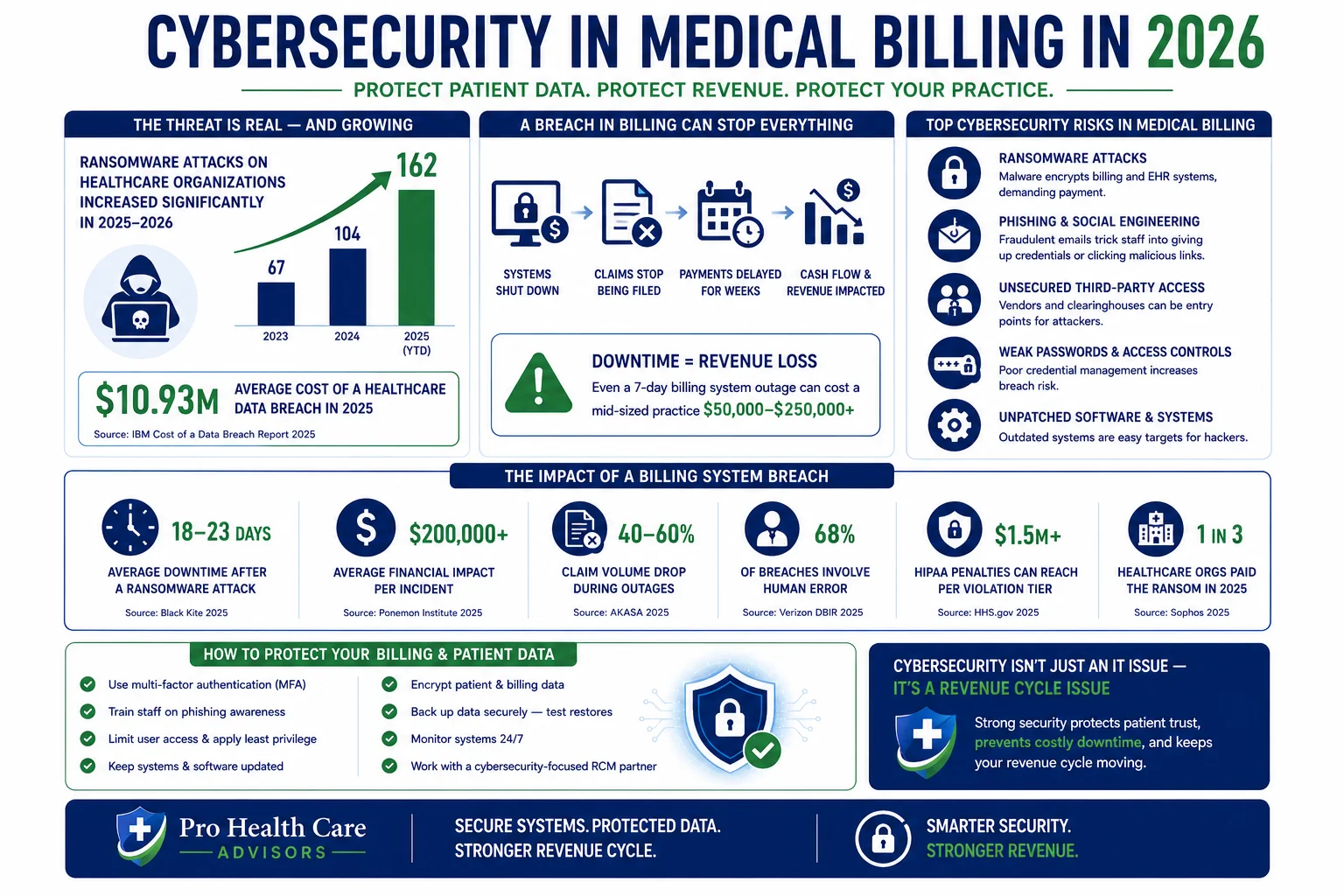
Ransomware attacks and breaches are still very common for healthcare providers, and their effects on the payment process have become even more pronounced in 2026. A cyber attack that leads to system failure can stop claim filing, delay payments, and disrupt cash flow for weeks. Cybersecurity practices will be inseparable from revenue cycle operations in 2026.
The Change Healthcare cyberattack of 2024 — which disrupted claims processing for thousands of practices across the country for weeks — made this connection viscerally clear. Many practices lost weeks of cash flow not because their own systems were breached, but because a billing clearinghouse they depended on was. The revenue cycle dependency on digital infrastructure is now impossible to ignore.
Cloud-based platforms that maintain enterprise-level encryption and HIPAA compliance provide a degree of resilience that on-premises or fragmented systems often cannot match.
What this means for your practice: Your billing company’s cybersecurity posture is now part of your revenue cycle risk profile. Ask your billing company or your in-house team specifically: what is your ransomware response plan? What happens to claims processing if your primary system goes down? Our HIPAA compliance services include documented security protocols and business continuity planning that protect your billing operations from exactly this category of disruption.
Trend 6 — The 2026 Medicare Physician Fee Schedule Changes Are Hitting Practices Now
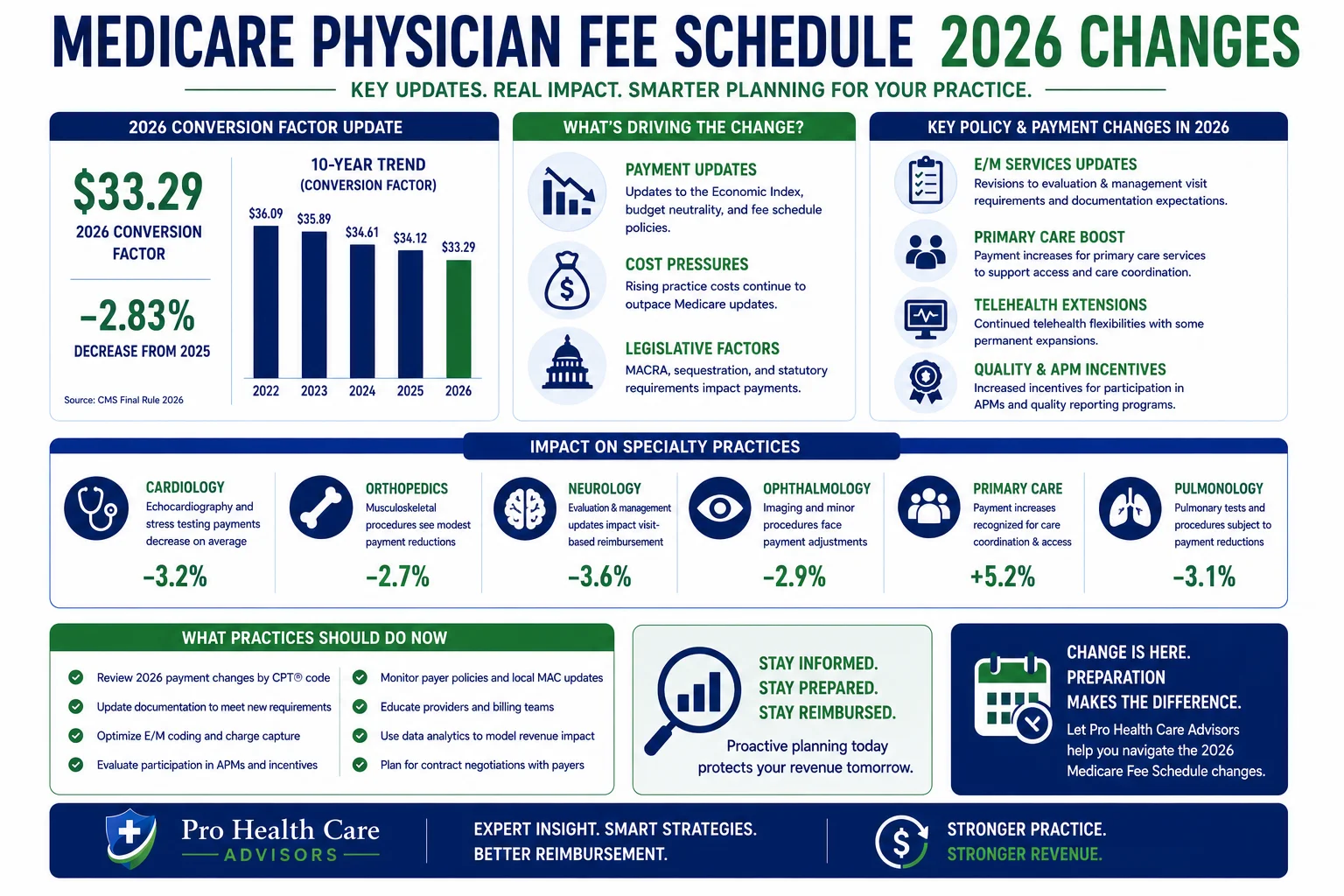
Every year, CMS updates the Medicare Physician Fee Schedule. Most years, the changes are incremental. In 2026, they are not.
CMS has finalized updates to the 2026 Medicare Physician Fee Schedule, including revised conversion factors and payment adjustments tied to participation in alternative payment models. ASCs, orthopedic practices, and behavioral health providers are particularly affected due to higher procedure costs and recurring care models.
The CMS Final Rule for 2026 has several updates on Medicare Part B payment policies that focus on equity, transparency, and quality. It further cements CMS’s direction toward value-based payment models that reward providers based on patient outcomes, not on volumes of services delivered. Practices will have to realign medical billing workflows to ensure that new quality measures and reporting criteria are in place and that the right data is present on the claim to prevent denials or delays. Increasingly, compliance and billing are becoming synonymous.
What this means for your practice: If your practice participates in Medicare Alternative Payment Models — or if you are considering it — the 2026 fee schedule changes directly affect your reimbursement strategy. Practices that are not actively monitoring CMS fee schedule updates are often collecting less than the allowed amount without realizing it. Our MD Audit Shield RAC service includes Medicare compliance monitoring that flags payment discrepancies and protects your practice from audit exposure tied to fee schedule misalignment.
Trend 7 — Denial Rates Are Still Rising — And Most Practices Are Not Winning the Appeals
What this means for your practice: every percentage point reduction in your denial rate translates directly to bottom-line revenue improvement. A practice with a 12 percent denial rate that improves to 3 percent can recover tens of thousands of dollars in annual revenue — simply by submitting cleaner claims.
The national initial claim denial rate hit 11.8 percent in 2024 and has continued rising into 2026. Medicare Advantage denial rates are even higher — running between 15 and 17 percent nationally. And the problem is compounded by the fact that <cite index=”59-1″>practices that make payment difficult will see their patient collection rates suffer</cite> — denial management and patient billing failures compound each other.
The most common denial codes driving this trend — CO-11, CO-15, CO-50 — all trace back to upstream process failures in documentation, prior authorization, and coding accuracy. They are almost entirely preventable.
What this means for your practice: If you do not know your current denial rate by payer and by denial code, you cannot fix it. Monthly EOB review is not enough — you need systematic denial categorization and pattern analysis. Our structured denial management workflow catches, categorizes, and appeals denials while feeding pattern data back upstream to prevent recurrence. For a complete breakdown of denial codes and fix steps, see our medical billing denial codes guide.
Trend 8 — Outsourcing Is Accelerating — And the Quality Gap Is Widening
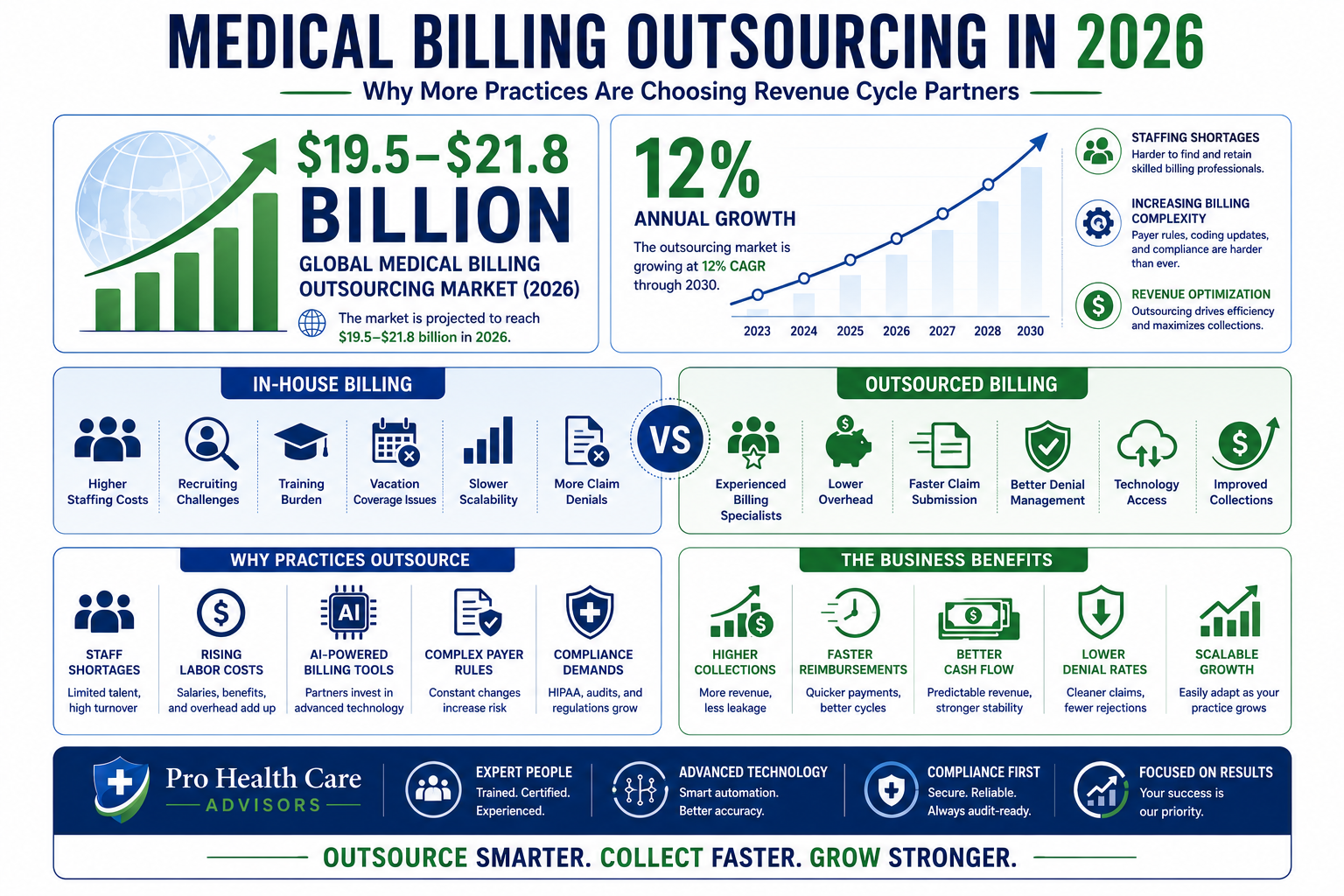
More providers are choosing to outsource their billing solutions than ever before. The reason is evident — in-house teams are struggling with the growing billing complexities. Outsourcing gives you access to better tools, experienced resources, and specialty-oriented expertise. Modern medical billing companies act as strategic partners — analyzing your performance, finding hidden revenue gaps, and addressing those gaps to target optimized revenue outcomes.
The medical billing outsourcing market reached $19.5 to $21.8 billion in 2026 and is growing at approximately 12 percent annually. Annual billing staff turnover runs between 33 and 40 percent — making in-house billing an increasingly expensive and unstable model for small and mid-size practices.
Staying ahead requires ongoing education, strategic technology investments, and sometimes, partnerships with specialists who can provide expertise your internal team may lack.
But here is the nuance inside this trend: not all outsourced billing companies are equal, and the performance gap between high-quality and average outsourced billing partners is widening just as fast as the gap between outsourced and in-house billing. A billing company with a 98.5 percent clean claim rate and a sub-2 percent denial rate produces dramatically different financial outcomes than one operating at 90 percent and 10 percent — even if both call themselves “outsourced billing companies.”
What this means for your practice: If you are considering outsourcing — or if you are already outsourced and not sure your current company is performing — the first step is getting the actual numbers. Not the pitch. The clean claim rate. The denial rate. The net collection rate. Those three numbers tell you everything. For a detailed comparison of in-house versus outsourced billing, read our complete guide to in-house vs outsourced medical billing.
Trend 9 — Physician Credentialing Delays Are Getting Longer — And Costing More
Credentialing has always been slow. In 2026, it is getting slower — and the financial consequences are getting larger.
The average time to complete physician credentialing with a new payer has stretched to 90 to 120 days in most markets — and in states with complex Medicaid managed care structures like California, Georgia, and Florida, it can run longer. Every day a provider is not credentialed with a payer is a day they are delivering care that cannot be billed.
Updates to physician workforce and visa policies may affect provider availability and staffing consistency, indirectly impacting documentation turnaround times and charge capture. New providers joining practices are particularly affected — the credentialing gap between a provider’s start date and their payer enrollment date creates a revenue void that is entirely preventable with proactive credentialing management.
What this means for your practice: Start credentialing new providers the moment their start date is confirmed — not when they arrive. And manage credentialing through the same company that handles your billing, so that enrollment status, NPI affiliations, and billing group registration are all synchronized. Our physician credentialing service handles the entire enrollment process with follow-up tracking that minimizes the gap between a provider’s first patient and their first paid claim.
Trend 10 — Compliance and Billing Are Becoming the Same Thing
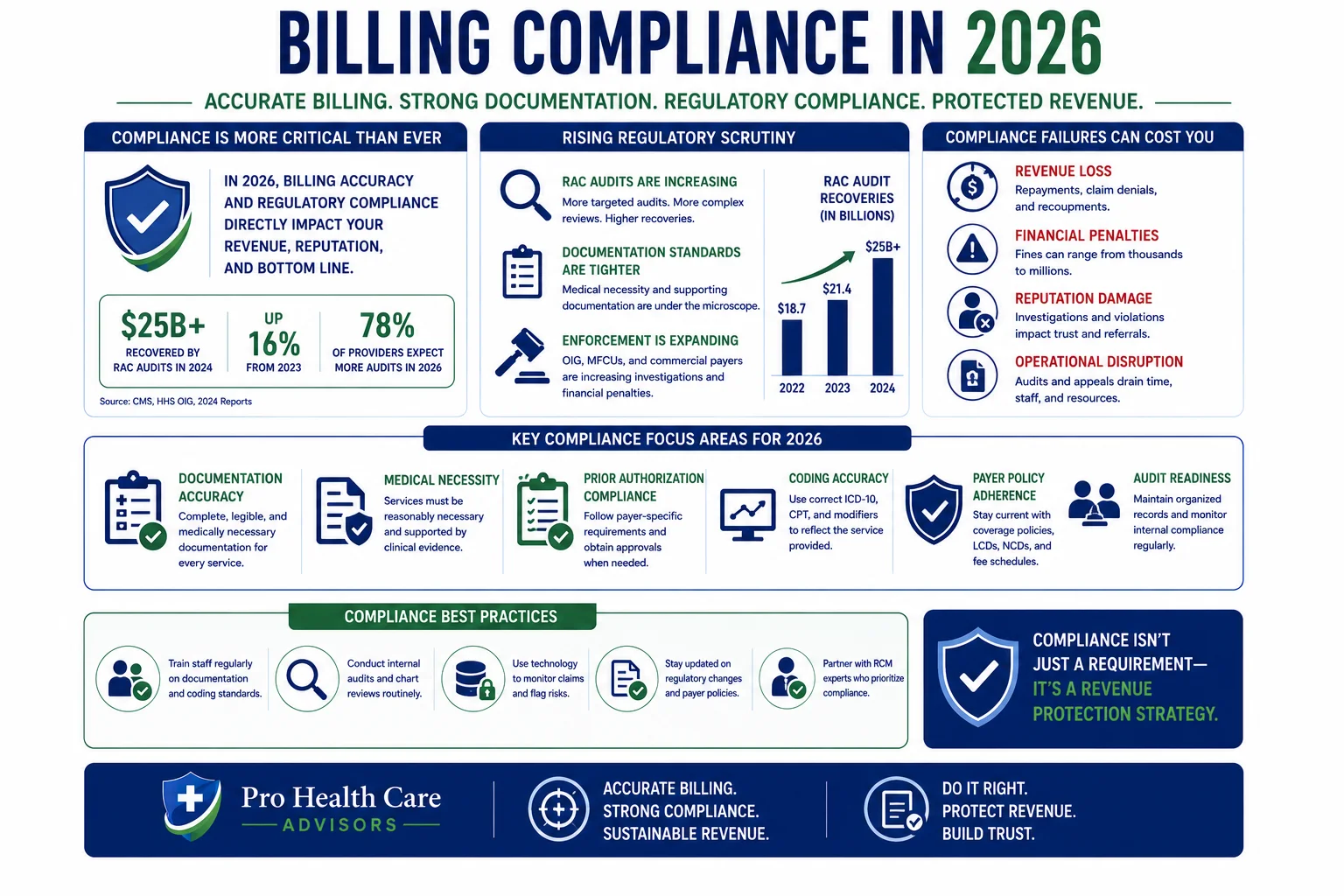
This is perhaps the most structurally important shift in the entire 2026 billing landscape — and the one most practices have not fully internalized yet.
Compliance and billing are becoming synonymous. Billing teams are increasingly looking for ways to apply sophisticated documentation, coding accuracy, and reporting tools. Practices will have to realign medical billing workflows to ensure that new quality measures and reporting criteria are in place and that the right data is present on the claim to prevent denials or delays.
Regulatory scrutiny around medical billing compliance, documentation accuracy, and audit readiness continues to intensify heading into 2026. RAC (Recovery Audit Contractor) activity is increasing. Medicare Advantage audits are expanding. And practices that treat billing and compliance as separate functions — or that have no audit preparation process at all — are exposed to financial recoupment risk that can dwarf the cost of building proper compliance workflows.
The HHS Office of Inspector General has consistently identified upcoding, improper place-of-service billing, and inadequate medical necessity documentation as the top compliance vulnerabilities in physician billing. All three are billing process failures, not clinical ones.
What this means for your practice: Every billing decision is a compliance decision. If your billing team is making decisions about code selection, modifier use, or place-of-service designation without a documented compliance rationale — you have audit exposure. Our MD Audit Shield RAC service and HIPAA compliance services build compliance into the billing process — not as a separate audit-prep exercise, but as a continuous operational standard.
How Pro Health Care Advisors Keeps Your Practice Ahead of Every One of These Trends

Every one of the 10 trends covered in this guide represents either a revenue opportunity or a revenue risk — depending on whether your billing operation is built to handle it.
Here is specifically how Pro Health Care Advisors addresses each trend for the practices we serve:
AI and automation — Our billing workflow incorporates AI-assisted claim scrubbing, denial prediction, and eligibility verification tools that catch errors before submission.
Prior authorization — We maintain systematic PA tracking workflows with payer-specific authorization rules built in — preventing CO-15 denials before they happen.
Patient collections — Our creative collection solutions address both insurance and patient balance recovery with structured follow-up that most in-house teams cannot sustain.
Specialty expertise — Our AAPC-certified billers cover 30+ specialties with specialty-specific payer knowledge. See our full specialties list.
Cybersecurity and HIPAA — Our HIPAA compliance services include enterprise-level security protocols, signed BAA management, and business continuity planning.
Medicare compliance — Our MD Audit Shield RAC service monitors fee schedule alignment and audit exposure continuously.
Denial management — Our sub-2 percent denial rate is built on upstream prevention — not reactive appeals. Learn more in our denial codes guide.
Credentialing — Our physician credentialing service minimizes the gap between a provider’s start date and their first paid claim.
Coding accuracy — Our CodeMAXX services add a dedicated coding review layer that catches errors before submission.
Compliance integration — Every billing decision we make is documented with a compliance rationale — protecting our clients from the audit exposure that comes from treating billing and compliance as separate functions.
The result: a 98.5 percent clean claim rate and a denial rate under 2 percent — consistently, across every trend reshaping the 2026 billing landscape.
For more billing education and resources, visit our articles and resources library.
Frequently Asked Questions — Medical Billing Trends 2026
Q: What is the biggest medical billing trend in 2026?
Prior authorization expansion is generating the most immediate revenue damage for practices right now — with physicians spending 14.5 hours per week on PA alone. But the broader trend of AI integration is the most structurally significant, because it is creating a widening performance gap between billing operations that have adopted AI-assisted workflows and those that have not.
Q: How is AI changing medical billing in 2026?
AI is now active across the full revenue cycle — predicting which claims will be denied before submission, automating eligibility verification, flagging coding errors, generating appeal language, and tracking prior authorization status in real time. According to Guidehouse research, AI-powered RCM investment is the top priority for medical groups in 2026.
Q: Why are patient collections harder in 2026?
High-deductible health plans now cover more than 57 percent of employer-sponsored insured workers — shifting a larger share of payment responsibility directly to patients. With 100 million Americans carrying medical debt, collecting from patients requires a structured, patient-friendly process that most practices have not fully built.
Q: Should I outsource my medical billing in 2026?
For most small and mid-size practices, yes — particularly given rising billing complexity, staffing instability, and the technology investment required to keep pace with AI-driven workflows. The true cost of in-house billing (including benefits, software, turnover, and uncollected denials) typically runs $70,000 to $120,000 per year for a small practice. For a complete analysis, read our in-house vs outsourced medical billing guide.
Q: How do the 2026 CPT code changes connect to these billing trends?
The 418 CPT code changes in 2026 — including 84 deletions and new AI Category I codes — directly intersect with the specialty RCM trend and the compliance-billing convergence trend. Practices using deleted codes are generating automatic rejections. Practices that have not adopted the new AI and RPM codes are leaving reimbursable services unbilled. For full details, see our CPT code changes 2026 guide.
Q: What is the biggest compliance risk in medical billing in 2026?
RAC audit activity is increasing, and the top vulnerabilities identified by the HHS Office of Inspector General are upcoding, improper place-of-service billing, and inadequate medical necessity documentation — all billing process failures with significant financial recoupment risk.