Heart Failure ICD-10 Codes 2026 — Complete I50 Series Billing Guide
Of all the coding decisions in cardiology, heart failure is where the most expensive mistakes happen.
Not because the codes are hard to find. Because coders default to I50.9 — unspecified heart failure — when the clinical documentation actually supports a far more specific code. And that one shortcut costs practices in two ways simultaneously: it triggers payer audits and medical necessity denials, and it removes the patient from HCC risk adjustment categories that generate significant revenue in value-based care arrangements.
According to PROMBS’s 2026 heart failure coding analysis, using I50.9 when documentation supports a more specific diagnosis is one of the most common — and most expensive — errors in cardiac billing. I50.9 signals a lack of clinical detail to payers, which frequently triggers claim denials and audits.
And here is what makes it particularly costly in 2026: under the updated CMS HCC Model v28 now fully in effect, specific heart failure codes (I50.2x, I50.3x) map to HCC 85 — a high-weight risk adjustment category worth significant per-member-per-month revenue in Medicare Advantage and ACO arrangements. I50.9 does not carry the same weight. Coding unspecified heart failure when systolic or diastolic can be coded is leaving money on the table twice.
This guide is the complete 2026 reference for I50 heart failure codes — what each code means, how to choose between them, what documentation the physician must provide, and the six mistakes that generate the most denials in heart failure billing.
For the complete cardiology ICD-10 reference covering hypertension, CAD, atrial fibrillation, and acute MI, see our ICD-10 codes for cardiology guide.
The Three Axes of Heart Failure Coding
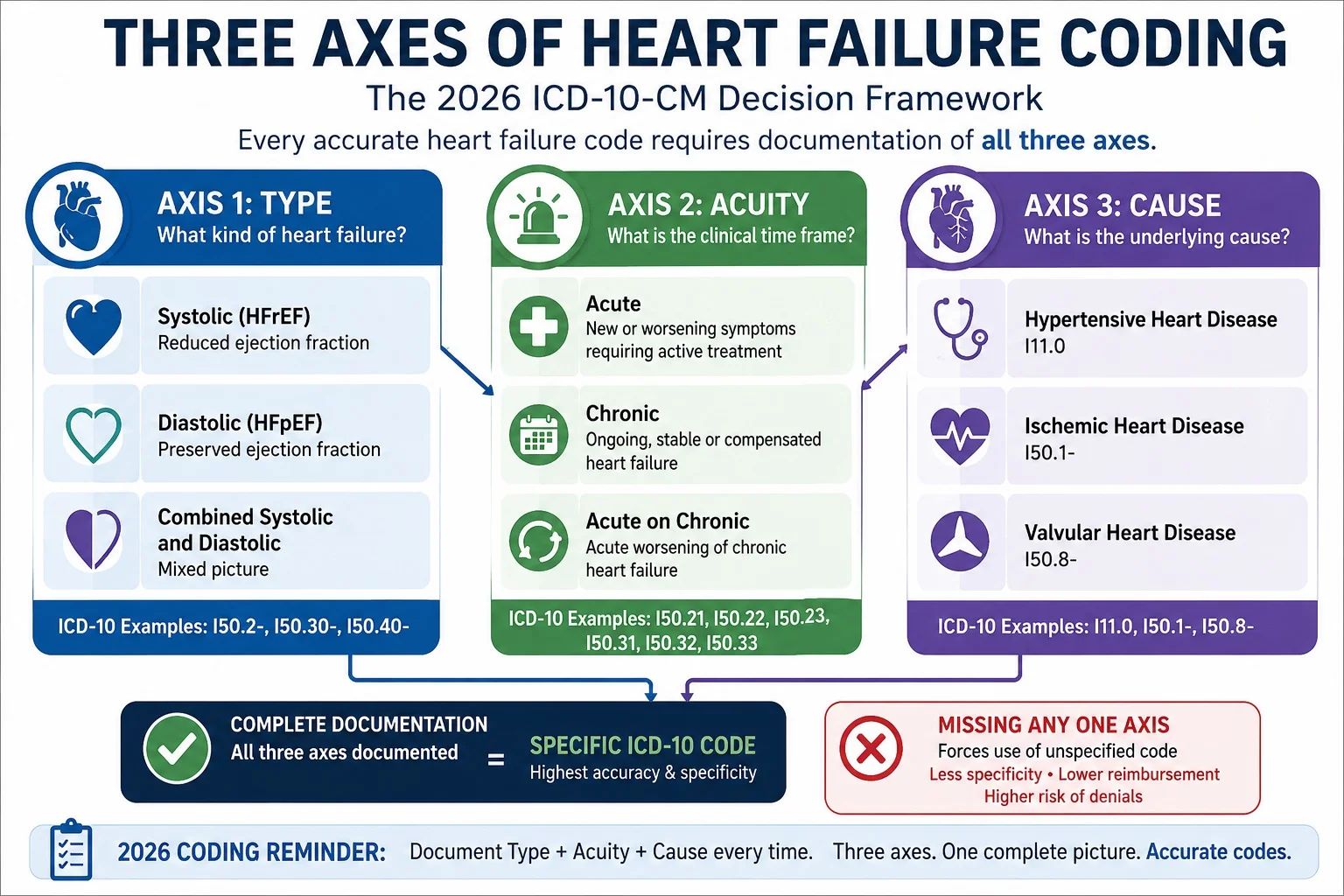
Accurate heart failure ICD-10 coding requires three documented elements — and all three must appear in the physician’s note, not just in a lab report or echocardiogram result. According to PROMBS’s documentation guidance, accurate assignment of the correct CHF ICD-10 code depends entirely on the specificity of the provider’s clinical notes.
Axis 1 — Type (The “What”):
- Systolic = HFrEF (Heart Failure with Reduced Ejection Fraction) — EF below 40%
- Diastolic = HFpEF (Heart Failure with Preserved Ejection Fraction) — EF 50% or above
- Combined = both systolic and diastolic dysfunction present
Axis 2 — Acuity (The “When”):
- Acute = new onset or rapid decompensation
- Chronic = stable, longstanding condition
- Acute-on-chronic = acute exacerbation of existing chronic heart failure
Axis 3 — Cause (The “Why”):
- Hypertensive → sequence I11.0 first, then the specific I50.x code
- Ischemic cardiomyopathy → add the appropriate CAD code
- Valvular etiology → add the appropriate valvular code
- No cause specified → I50.x code alone with no additional cause code
The most important rule in 2026 heart failure coding: the ejection fraction number alone does not assign the code. According to OmniMD’s CHF coding guide, the provider must clearly document “systolic heart failure,” “HFrEF,” “reduced ejection fraction,” or similar language in the assessment or plan. A reduced EF that appears only in an echocardiogram report — without a provider-stated diagnosis — does not meet the coding requirement. The physician’s words create the diagnosis. The EF value supports it.
Complete I50 Heart Failure Code Reference — 2026
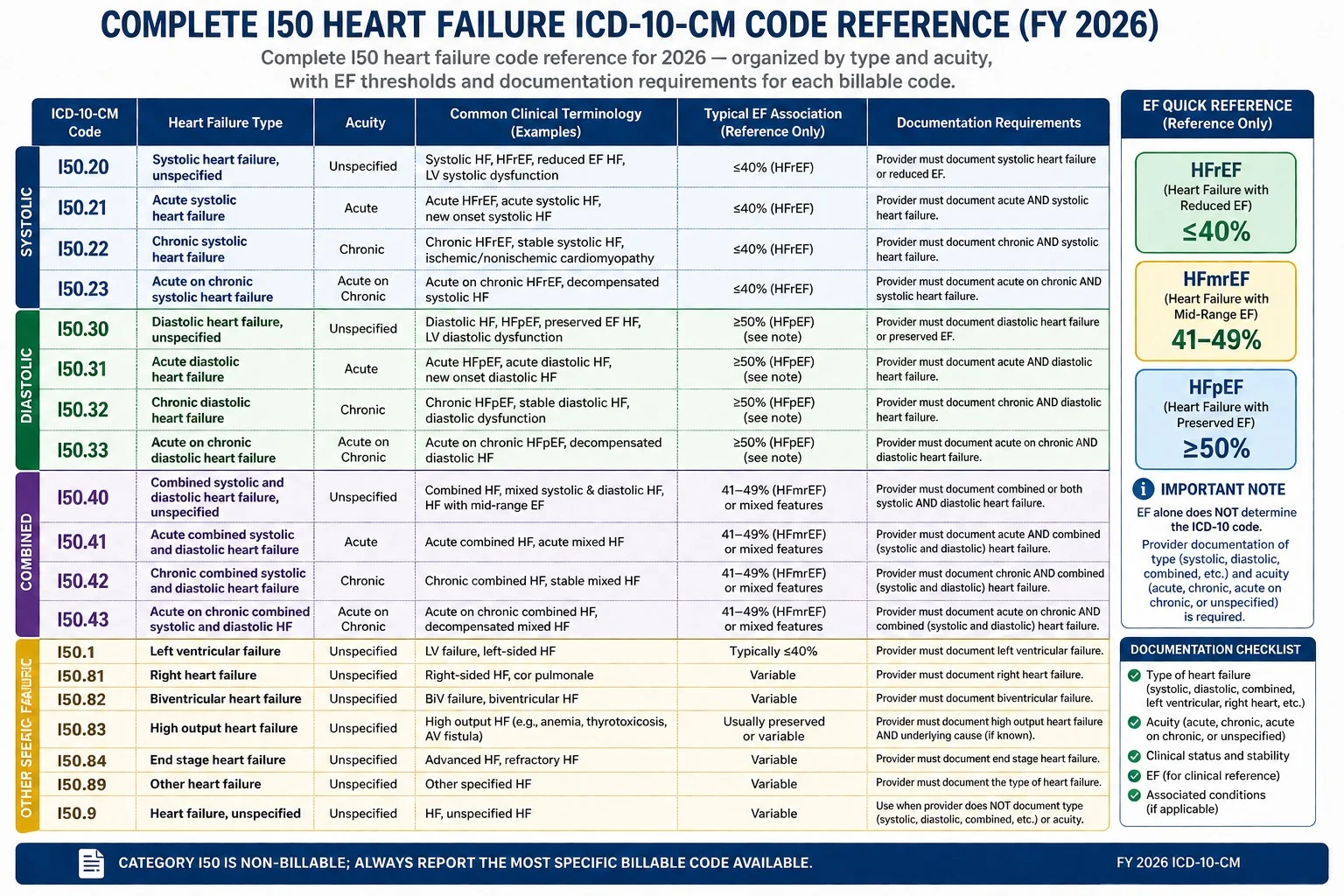
I50.1 — Left Ventricular Failure
| Code | Description | When to Use |
|---|---|---|
| I50.1 | Left ventricular failure, unspecified | Only when provider documents “left ventricular failure” or “left heart failure” without specifying systolic or diastolic mechanism |
According to Skriber’s HFrEF coding guide, I50.1 is a tricky code. It is often used for acute pulmonary edema — but official guidelines clarify that I50.2 (HFrEF) is the preferred code for chronic systolic failure. Use I50.1 only when the provider documents “left ventricular failure” without the terms “systolic” or “HFrEF.” If both mechanism and acuity are known, I50.2x or I50.3x always gives a more complete picture. I50.1 has no acuity subcategories — meaning you cannot distinguish acute from chronic within this code.
I50.2x — Systolic Heart Failure (HFrEF)
Systolic heart failure = the heart muscle is too weak to squeeze effectively. EF is 40% or below. Also known as Heart Failure with Reduced Ejection Fraction (HFrEF).
| Code | Description | EF / Documentation Required |
|---|---|---|
| I50.20 | Systolic HF, unspecified | HFrEF documented but acute/chronic not specified |
| I50.21 | Acute systolic HF | New onset or acute decompensation; EF ≤40%; “acute” in physician note |
| I50.22 | Chronic systolic HF | Stable, longstanding HFrEF; EF ≤40%; “chronic” in physician note |
| I50.23 | Acute on chronic systolic HF | Acute exacerbation of established HFrEF; EF ≤40%; both documented |
Documentation must explicitly state: “systolic heart failure,” “HFrEF,” or “reduced ejection fraction” in the physician’s assessment or plan — along with the acuity (acute, chronic, or acute-on-chronic).
Real documentation example for I50.22: “Chronic systolic heart failure (HFrEF), LVEF 32% by echocardiogram [date]. Patient at current clinical baseline on optimized GDMT. No evidence of acute decompensation.” — This gives the coder everything needed: type (systolic/HFrEF), EF (32%), and acuity (chronic, no acute decompensation).
Real documentation example for I50.23: “Acute on chronic systolic heart failure. Patient with known HFrEF (LVEF 28%) presenting with acute decompensation — new onset dyspnea, orthopnea, and 8-pound weight gain over 3 days.” — This clearly establishes the chronic baseline and the acute event.
I50.3x — Diastolic Heart Failure (HFpEF)
Diastolic heart failure = the heart muscle is too stiff to relax and fill properly between beats. EF is 50% or above. Also known as Heart Failure with Preserved Ejection Fraction (HFpEF).
| Code | Description | EF / Documentation Required |
|---|---|---|
| I50.30 | Diastolic HF, unspecified | HFpEF documented but acute/chronic not specified |
| I50.31 | Acute diastolic HF | New onset or acute decompensation; EF ≥50%; “acute” in physician note |
| I50.32 | Chronic diastolic HF | Stable HFpEF; EF ≥50%; “chronic” in physician note |
| I50.33 | Acute on chronic diastolic HF | Acute exacerbation of established HFpEF; EF ≥50%; both documented |
Per 2026 HFpEF definition: The provider must document preserved ejection fraction, diastolic dysfunction, or HFpEF — AND objective evidence of elevated filling pressures such as elevated BNP, abnormal E/A ratio, or reduced E’ velocity on tissue Doppler. An echo showing preserved EF is not sufficient alone — the provider must connect that finding to a clinical diagnosis of diastolic heart failure.
Key distinction — do not use I50.3x if: The provider documents preserved EF but does NOT diagnose diastolic heart failure. The code requires the provider’s explicit diagnosis, not the coder’s inference from a normal EF value.
I50.4x — Combined Systolic and Diastolic Heart Failure
| Code | Description | When to Use |
|---|---|---|
| I50.40 | Combined HF, unspecified | Both systolic and diastolic documented; acuity unspecified |
| I50.41 | Acute combined HF | Acute onset; both mechanisms documented |
| I50.42 | Chronic combined HF | Chronic; both mechanisms documented |
| I50.43 | Acute on chronic combined HF | Acute exacerbation; both mechanisms documented |
Use I50.4x only when both systolic dysfunction (EF ≤40%) AND diastolic dysfunction are explicitly documented by the provider. This is not simply a “we are not sure which type” code — it requires clear documentation that both mechanisms are present.
I50.8x — Other Heart Failure Types
| Code | Description |
|---|---|
| I50.810 | Right heart failure, unspecified |
| I50.811 | Acute right heart failure |
| I50.812 | Chronic right heart failure |
| I50.813 | Acute on chronic right heart failure |
| I50.814 | Right heart failure due to left heart failure |
| I50.82 | Biventricular heart failure |
| I50.83 | High output heart failure |
| I50.84 | End stage heart failure (Stage D) |
| I50.89 | Other heart failure |
I50.84 — End Stage Heart Failure (Stage D): This code requires an additional code specifying the type — the provider must document both “Stage D” or “end stage heart failure” AND the specific type (systolic, diastolic, or combined). I50.84 is never used alone.
I50.83 — High Output Heart Failure: Used for heart failure caused by conditions that increase cardiac demand beyond what the heart can meet — sepsis, severe anemia, thiamine deficiency, hyperthyroidism, arteriovenous fistula. Requires an additional code identifying the underlying cause.
I50.9 — Heart Failure, Unspecified
| Code | Description | When Acceptable |
|---|---|---|
| I50.9 | Heart failure, unspecified | ONLY when the type and acuity truly cannot be determined from any available documentation |
I50.9 is the code of last resort — not the default. It is appropriate only when the provider documents heart failure without any specification of type or acuity, AND no other documentation in the record (echo report, prior notes, consultant letters) provides enough clinical detail to support a more specific code.
Using I50.9 when documentation supports a specific code is both a coding error and a financial mistake. It triggers payer audits, reduces reimbursement, and eliminates the patient from HCC 85 risk adjustment in Medicare Advantage and ACO models.
The Ejection Fraction Rule — What Coders Must Understand
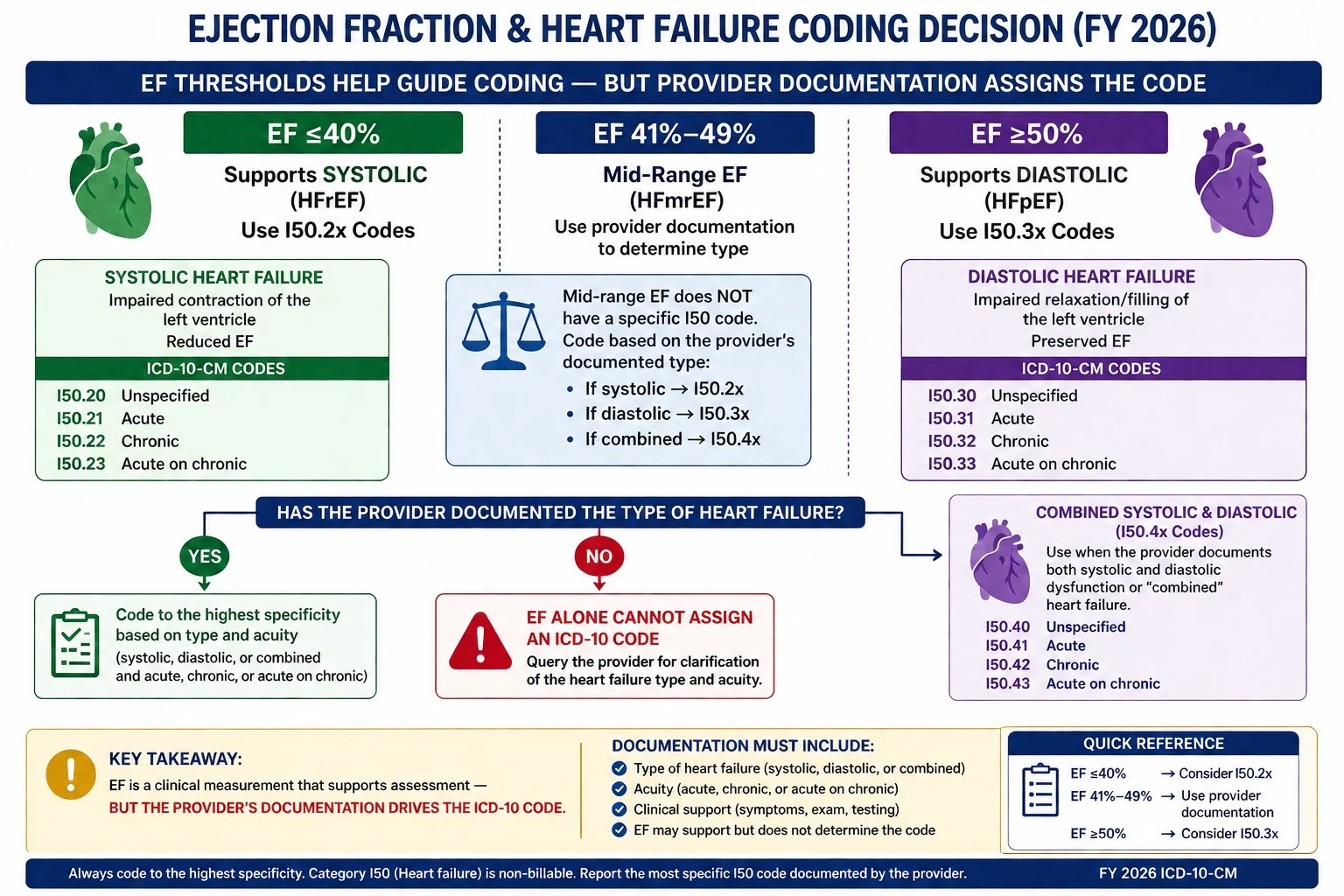
The ejection fraction thresholds for 2026 heart failure coding are straightforward — but the rule about who can use them is not.
EF ≤ 40% → supports I50.2x (systolic heart failure / HFrEF) EF 41–49% → heart failure with mildly reduced EF — provider must specify; no single standard code EF ≥ 50% → supports I50.3x (diastolic heart failure / HFpEF)
The critical rule: the EF number alone does not assign the code. The provider must explicitly state the diagnosis — “systolic heart failure,” “HFrEF,” “diastolic heart failure,” or “HFpEF” — in their assessment or plan section. An echocardiogram showing EF of 32% does not authorize the coder to assign I50.22. The cardiologist must say “systolic heart failure” or “HFrEF” in their own words.
What happens when EF is documented but diagnosis is not explicitly stated? The coder must query the provider. Do not infer. Do not code from the echo report alone. Query the physician and wait for a response before assigning a specific I50.2x or I50.3x code.
This distinction — EF supports the code, but the provider’s words create it — is the most commonly misunderstood aspect of heart failure coding in 2026. Getting it wrong in either direction creates problems: coding specific when documentation does not support it creates audit risk; coding unspecified when it is supported costs revenue.
Sequencing Rules — Heart Failure With Hypertension, CAD, or Other Causes
The cause of heart failure directly affects code sequencing — and sequencing errors are a documented audit trigger in cardiology billing.
When heart failure is due to hypertension: Sequence I11.0 (hypertensive heart disease with heart failure) FIRST, then add the specific I50.x code. Do not sequence the heart failure code first when hypertension is the established cause.
Example: Hypertensive patient with chronic systolic heart failure → I11.0 + I50.22 (not I50.22 + I11.0)
When heart failure is due to ischemic cardiomyopathy (CAD): The appropriate I25.x code is sequenced based on the clinical context. The I50.x heart failure code is added as a secondary code.
Example: CAD with chronic systolic HF → I25.10 + I50.22 (sequencing depends on reason for encounter)
When heart failure is due to valvular disease: The valvular code (I34.x–I38) is coded, with the I50.x code as additional.
When both hypertension AND CKD exist alongside heart failure: Use the I13.x combination code (hypertensive heart and CKD), not separate I11.x and I12.x codes. The specific heart failure type (I50.x) and CKD stage (N18.x) are then added.
Example: Hypertension + CKD stage 3 + chronic systolic HF → I13.0 + I50.22 + N18.3
For the complete hypertension combination code rules including I13.x sequencing, see our hypertension ICD-10 codes guide.
The 6 Most Common Heart Failure ICD-10 Coding Errors in 2026
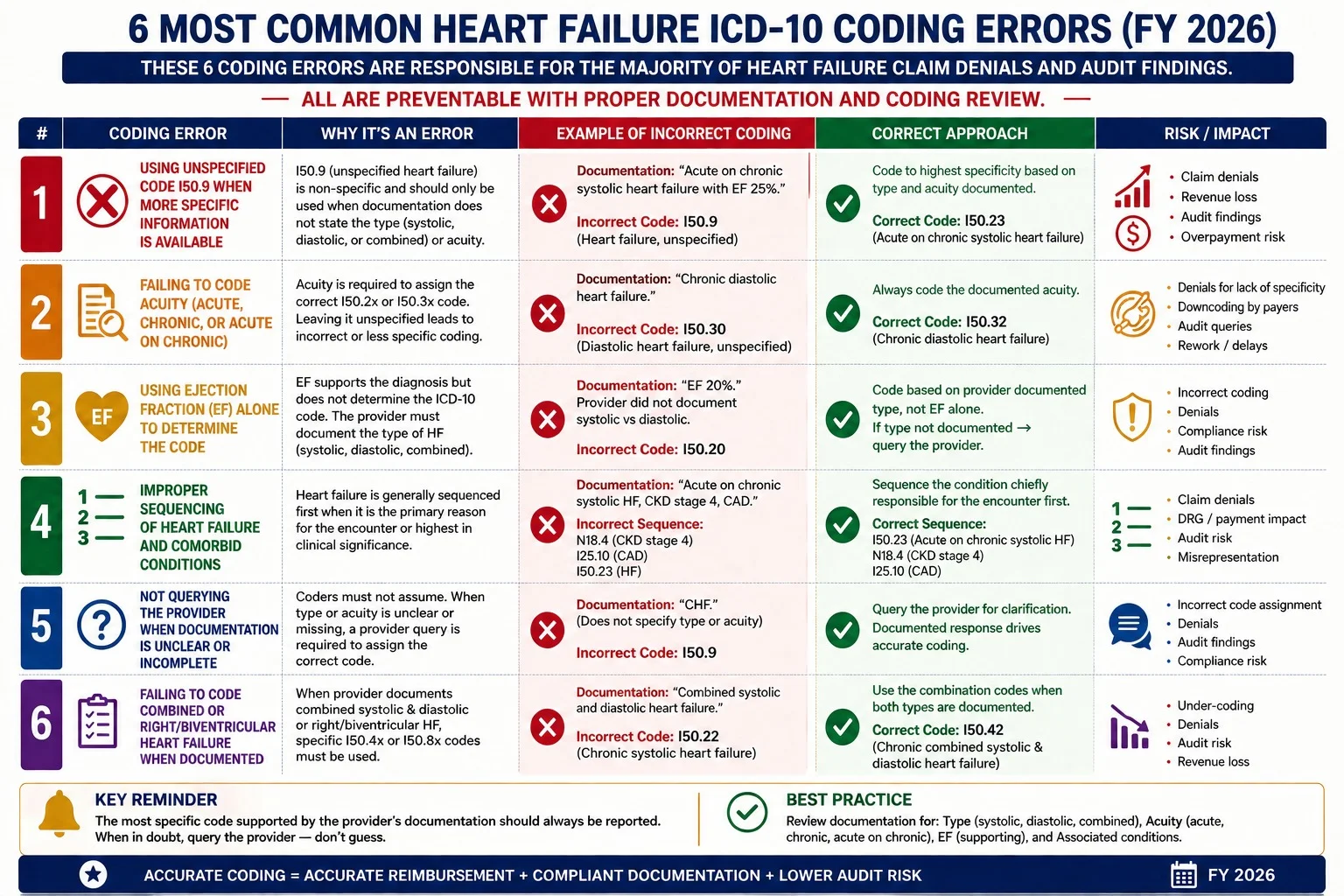
Error 1: Defaulting to I50.9 when specific codes are supported. The single most common and most expensive heart failure coding mistake. If the physician note documents “chronic systolic heart failure” or provides an EF with a corresponding diagnosis, I50.9 is never correct. Query the provider if documentation is unclear — but do not default to unspecified when specificity is available.
Error 2: Coding from the echo report instead of the physician note. A reduced EF in an echocardiogram report does not authorize coding systolic heart failure. The provider must state the diagnosis. Code from the physician’s assessment and plan — not from objective test results alone.
Error 3: Sequencing the I50.x code before I11.0 when hypertension is the cause. When hypertension is documented as the cause of heart failure, I11.0 must be sequenced first. Placing I50.22 before I11.0 is a sequencing error that triggers payer review.
Error 4: Using I50.4x for unclear or unspecified heart failure. I50.4x (combined systolic and diastolic) is not a fallback for uncertainty. It requires explicit documentation that BOTH systolic dysfunction (EF ≤40%) AND diastolic dysfunction are present. When the type is uncertain, I50.9 applies — not I50.4x.
Error 5: Missing I50.x code when billing I11.0. I11.0 (hypertensive heart disease with heart failure) always requires an additional I50.x code specifying the type of heart failure. Submitting I11.0 alone is incomplete coding — it will not capture the HCC risk weight for the specific heart failure type.
Error 6: Not updating the heart failure code after acute-on-chronic resolution. A patient admitted with acute-on-chronic systolic heart failure (I50.23) who stabilizes before discharge should have their discharge diagnosis reflect the current clinical status. If the patient returns to chronic baseline, the discharge code is I50.22 — not I50.23. Ongoing use of acute codes for stable patients attracts audit attention.
Heart Failure Coding and HCC Risk Adjustment in 2026
Heart failure coding has direct financial implications in Medicare Advantage and ACO arrangements through Hierarchical Condition Categories (HCC) risk adjustment.
Under the CMS HCC Model v28 — fully implemented for 2026 — specific heart failure codes map to HCC 85 (Congestive Heart Failure), which carries a significant risk adjustment factor. I50.9 (unspecified) does carry some HCC weight — but specific systolic and diastolic codes carry greater specificity value in risk adjustment validation, and payers increasingly conduct clinical validation reviews to confirm that the specificity of the coded diagnosis is supported by the documentation.
What this means practically: a practice with 200 Medicare Advantage patients with heart failure who are coded as I50.9 instead of I50.22 or I50.32 is not necessarily losing HCC credit entirely — but it is creating clinical validation exposure that can result in risk adjustment recoupments if auditors determine the unspecified code does not reflect the documented clinical reality.
The correct approach: code to the highest specificity the provider has documented, query when documentation is unclear, and educate providers on the three documentation elements (type, acuity, cause) that determine which I50.x code applies.
For more on how HCC coding affects revenue cycle performance, see our revenue cycle management complete guide.
How Pro Health Care Advisors Handles Heart Failure Coding

Our cardiology billing services include AAPC-certified coders who apply the three-axis framework to every heart failure claim — verifying type, acuity, and cause before code assignment, querying providers when documentation is incomplete rather than defaulting to I50.9, and confirming sequencing when hypertension or other causes are documented.
Our CodeMAXX services specifically flag I50.9 usage on claims where the record contains echo EF data or provider language suggesting a more specific code is appropriate — routing those claims for provider query before submission rather than after denial.
For more on how denial codes work and what to do when heart failure claims are denied, see our medical billing denial codes guide.
For the complete cardiology ICD-10 reference, see our ICD-10 codes for cardiology guide.
Frequently Asked Questions — Heart Failure ICD-10 Codes 2026
Q: What is the ICD-10 code for congestive heart failure in 2026? There is no single correct code for CHF — it depends on type and acuity. Systolic CHF uses I50.2x codes (I50.21 acute, I50.22 chronic, I50.23 acute-on-chronic). Diastolic CHF uses I50.3x codes. Combined uses I50.4x. I50.9 (unspecified) should only be used when type and acuity truly cannot be determined from any documentation.
Q: What is the difference between I50.21 and I50.22? I50.21 is acute systolic heart failure — new onset or acute decompensation of HFrEF. I50.22 is chronic systolic heart failure — stable, longstanding HFrEF without acute decompensation. The physician must explicitly document “acute” or “chronic” in their note for either code to apply. Both require documentation of systolic dysfunction or HFrEF with EF at or below 40%.
Q: Can I code I50.22 from an echocardiogram showing EF of 30%? No. An echocardiogram showing reduced EF does not authorize the coder to assign I50.22. The physician must explicitly state “systolic heart failure,” “HFrEF,” or “reduced ejection fraction” in their clinical note — assessment or plan section. If the provider has not made this diagnosis explicit, query them before assigning a specific code.
Q: When is I50.9 appropriate to use in 2026? I50.9 is appropriate only when the provider documents heart failure without specifying type or acuity, and no other documentation in the record (prior notes, echo reports, consultant letters) supports a more specific assignment. If there is any clinical information that points toward systolic or diastolic failure, query the provider rather than defaulting to I50.9.
Q: How does heart failure coding affect Medicare Advantage reimbursement? Specific heart failure codes (I50.2x, I50.3x) map to HCC 85 under the CMS HCC Model v28, affecting risk adjustment revenue in MA plans and ACO arrangements. Coding I50.9 when specific codes are supported creates clinical validation exposure and may result in risk adjustment recoupments if auditors determine the coded diagnosis does not match the documented clinical reality.
Q: What code is used when a patient has both hypertension and heart failure? When hypertension causes heart failure, use I11.0 (hypertensive heart disease with heart failure) as the primary code, followed by the specific I50.x heart failure type code. For example, hypertension with chronic systolic heart failure is coded I11.0 + I50.22. When hypertension, heart failure, AND chronic kidney disease are all present, use I13.0 + the specific I50.x code + N18.x (CKD stage). For complete rules, see our hypertension ICD-10 codes guide.
For more billing education and resources, visit our articles and resources library.
The Bottom Line — Heart Failure Coding Rewards Documentation Specificity
Every I50.9 on a claim where I50.22 or I50.32 applies is a missed opportunity — not just for correct coding, but for proper reimbursement, accurate risk adjustment, and audit protection.
The solution is not complicated. It is three questions: What type of heart failure? What acuity? What caused it? When the physician’s note answers all three, the coder has everything needed. When it does not, the right next step is a provider query — not a default to unspecified.
Pro Health Care Advisors builds exactly this kind of coding discipline into every cardiology claim we process — with a 98.5 percent clean claim rate and a denial rate under 2 percent across our cardiology client base.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pitch. No pressure. Just a real review of how your heart failure claims are being coded and whether there are specific, fixable opportunities to improve your reimbursement.