ICD-10 Codes for Cardiology 2026 — Common Mistakes to Avoid and Complete Billing Reference
Cardiology billing is not like billing for primary care. The stakes are higher, the procedures are more complex, and payer scrutiny is more intense than in almost any other specialty.
One wrong ICD-10 code on a cardiac catheterization claim can mean a denial worth thousands of dollars. Pair a procedure code with the wrong diagnosis and the entire claim gets flagged as medically unnecessary. Use a non-specific hypertension code when the documentation supports a more precise cardiac complication, and you are leaving reimbursement on the table on every similar encounter — month after month, without a single visible error ever appearing on a denial report.
According to data from MediBill RCM’s cardiology billing analysis, cardiology practices typically achieve clean claim rates of only 78 to 82 percent — compared to the 85 to 90 percent average across all specialties. That gap reflects how uniquely vulnerable cardiology is to coding-related denials. And according to RCM Experts’ cardiology billing guide, cardiology practices lose 5 to 8 percent of revenue annually due to claim denials, coding errors, and missed payments.
This guide is the complete 2026 ICD-10 coding reference for cardiology practices. It covers the most commonly used diagnosis codes by condition, the most common mistakes that generate denials, CPT and ICD-10 pairing rules, documentation requirements, and what your billing team needs to know right now to stop losing revenue to preventable coding errors.
Why Cardiology ICD-10 Coding Is More Complex Than Other Specialties
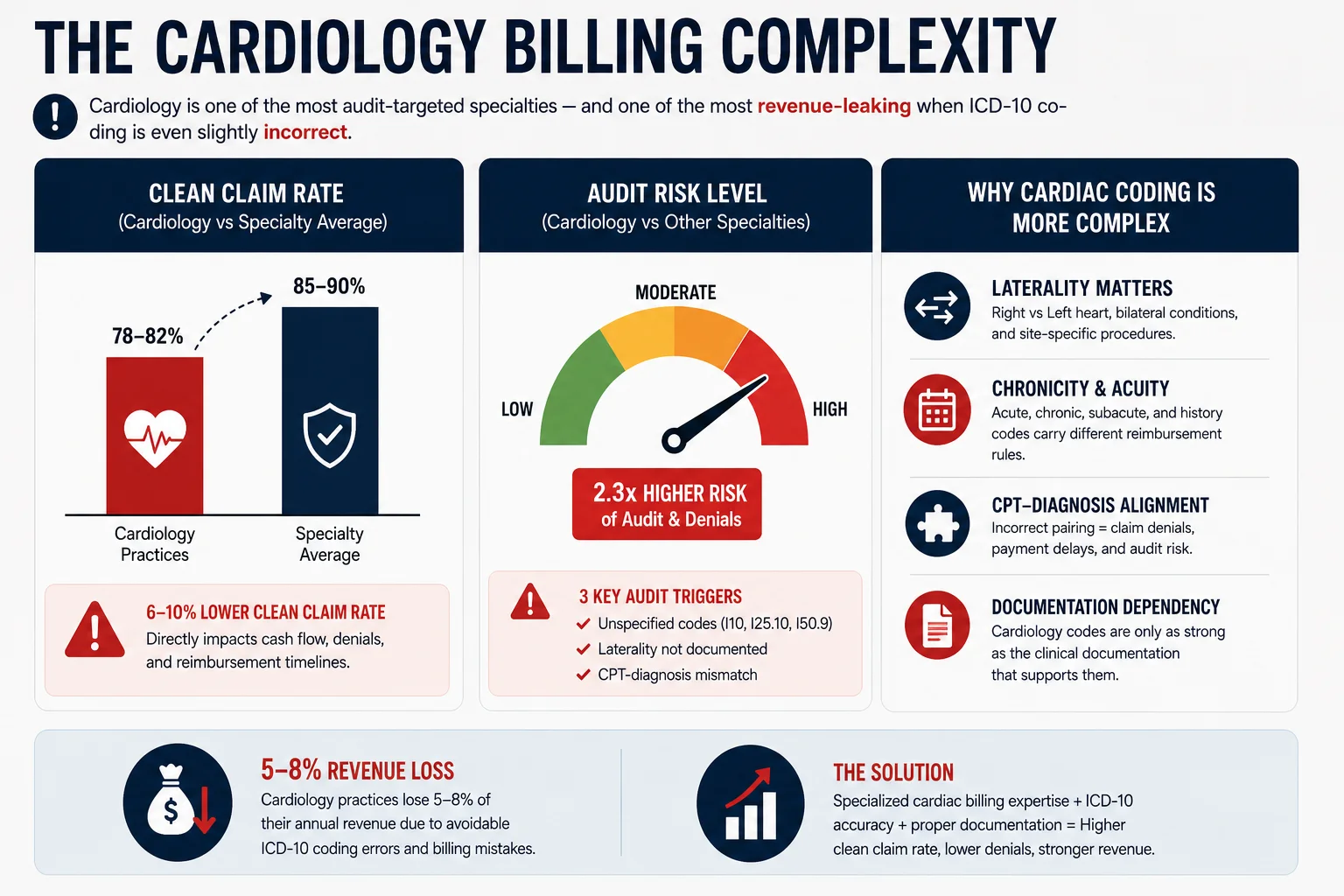
Three things make cardiology ICD-10 coding structurally harder than coding for most specialties:
Specificity requirements are unusually demanding. Cardiology ICD-10 codes require precise documentation of acuity (stable vs. unstable), chronicity (acute vs. chronic), laterality (left vs. right coronary artery), episode of care (initial vs. subsequent vs. sequela), and associated conditions (with or without heart failure, with or without angina). A non-specific code that lacks any of these elements will be rejected by payer automated scrubbers or generate a medical necessity denial.
CPT-ICD alignment is closely audited. Payers use automated claim-scrubbing systems that cross-reference the diagnosis code against the procedure code. When the procedure and diagnosis do not logically align — for example, billing a stent placement against a non-specific chest pain code — the claim triggers a medical necessity denial. According to MediBill RCM’s CPT and ICD-10 guide, CPT-ICD mismatches are among the top triggers for Recovery Audit Contractor (RAC) reviews in cardiology.
RAC audit risk is higher in cardiology than almost anywhere else. The OIG specifically targets cardiac procedures — including cardiac catheterizations, echocardiograms, stress tests, and device implantations — as high-priority audit categories. A single RAC audit finding based on a coding error can result in payment recoupments that wipe out months of revenue. For our audit protection approach, see our MD Audit Shield RAC service.
Understanding these three structural challenges is the foundation of good cardiology billing. Everything else in this guide builds on them.
The Most Common ICD-10 Codes in Cardiology — Complete 2026 Reference
Hypertension Codes
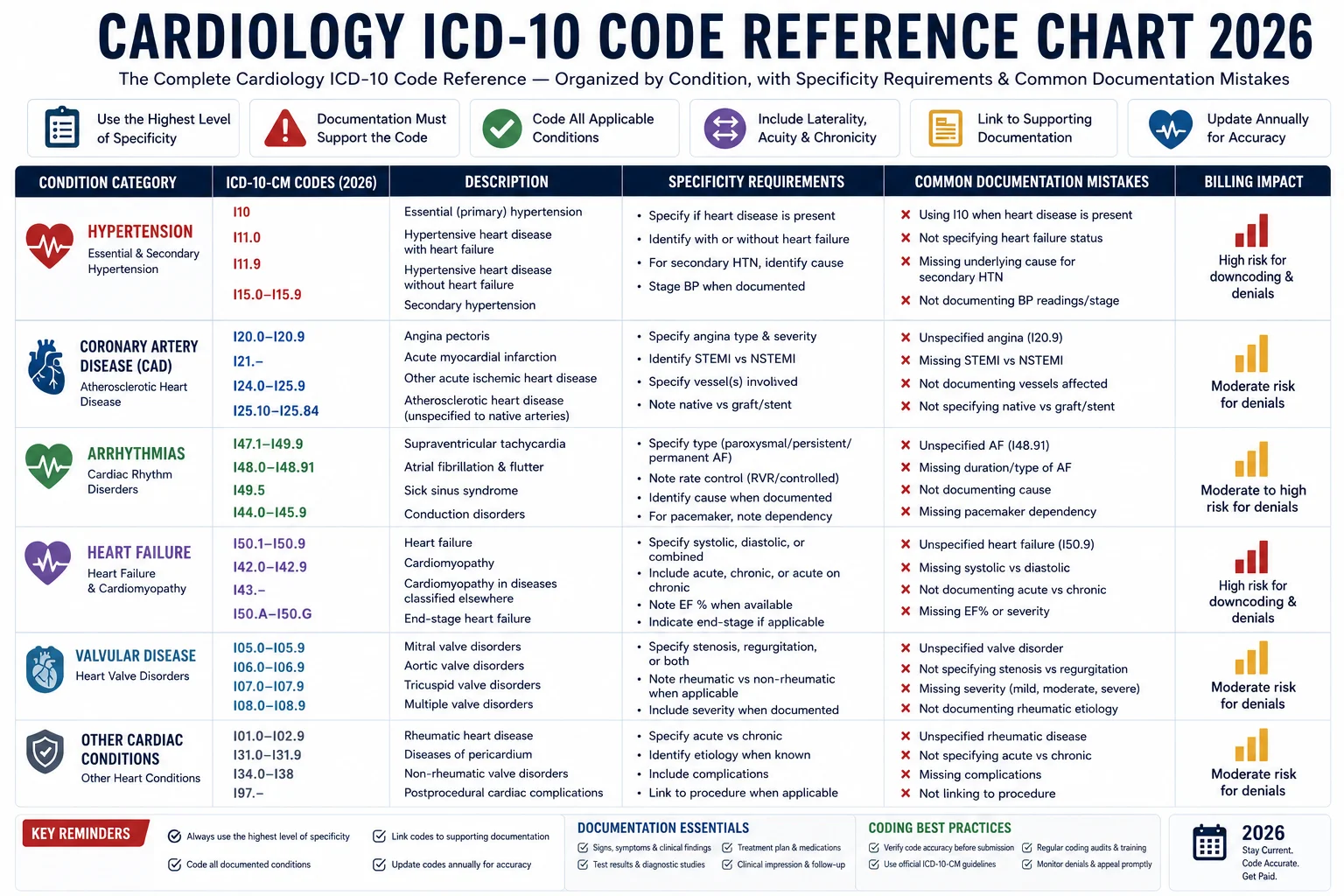
According to S10.AI’s cardiology coding analysis, essential hypertension (I10) appears in approximately 60 percent of cardiovascular encounters — making it the most frequently used code in cardiology by a wide margin.
| ICD-10 Code | Description | Key Documentation Requirement |
|---|---|---|
| I10 | Essential (primary) hypertension | Blood pressure readings; specify if controlled or uncontrolled |
| I11.0 | Hypertensive heart disease with heart failure | Must document causal relationship between hypertension and heart failure |
| I11.9 | Hypertensive heart disease without heart failure | Must document cardiac condition caused by hypertension |
| I12.9 | Hypertensive chronic kidney disease, stage 1–4 | CKD stage must be documented by the provider |
| I13.0 | Hypertensive heart and CKD with heart failure and stage 1–4 CKD | Most complex — requires documentation of HF, CKD stage, and BP control |
| I16.0 | Hypertensive urgency | Document symptomatic elevation without acute organ damage |
| I16.1 | Hypertensive emergency | Document acute organ damage as direct consequence of hypertension |
Most common mistake: Using I10 (essential hypertension) when the documentation supports a more specific code — such as I11.x for hypertensive heart disease or I12.x for hypertensive CKD. Always code to the highest specificity the documentation supports.
Coronary Artery Disease (CAD) and Atherosclerosis Codes
| ICD-10 Code | Description | Key Documentation Requirement |
|---|---|---|
| I25.10 | Atherosclerotic heart disease of native coronary artery without angina | Native vessel; no angina documented |
| I25.110 | Atherosclerotic heart disease of native coronary artery with unstable angina | Unstable angina must be documented clinically |
| I25.111 | Atherosclerotic heart disease with angina pectoris with documented spasm | Coronary artery spasm documented |
| I25.118 | Atherosclerotic heart disease with other angina pectoris | Stable angina without spasm |
| I25.2 | Old myocardial infarction | History of MI, no longer in acute phase |
| I25.700 | Atherosclerosis of coronary artery bypass graft without angina | CABG graft; no angina |
| I25.750 | Atherosclerosis of native coronary artery of transplanted heart without angina | Transplanted heart; native coronary |
Most common mistake: Using I25.10 (without angina) when angina is documented. If angina is present, the code must reflect the angina type — unstable (I25.110), stable (I25.118), or with documented spasm (I25.111). Using the wrong angina status is one of the most common medical necessity denial triggers in interventional cardiology.
Critical pairing rule: When billing for a cardiac catheterization (CPT 93454–93461) or PCI (CPT 92928, 92929), the ICD-10 diagnosis must clearly support the need for the procedure. According to MediBill RCM:
- Incorrect: R07.9 (Chest pain, unspecified) + 92928 (Stent placement) — automatic medical necessity denial
- Correct: I25.110 (Atherosclerotic heart disease with unstable angina) + 92928 — defensible clinical story
Heart Failure Codes
| ICD-10 Code | Description | Ejection Fraction Requirement |
|---|---|---|
| I50.20 | Systolic (congestive) heart failure, unspecified | EF below 40%; type unspecified |
| I50.21 | Acute systolic (congestive) heart failure | Acute onset, EF below 40% |
| I50.22 | Chronic systolic (congestive) heart failure | Chronic, EF below 40% |
| I50.23 | Acute on chronic systolic heart failure | Acute exacerbation of chronic HFrEF |
| I50.30 | Diastolic (congestive) heart failure, unspecified | EF 40% or above; type unspecified |
| I50.31 | Acute diastolic (congestive) heart failure | Acute onset HFpEF |
| I50.32 | Chronic diastolic (congestive) heart failure | Chronic HFpEF |
| I50.33 | Acute on chronic diastolic heart failure | Acute exacerbation of chronic HFpEF |
| I50.40 | Combined systolic and diastolic heart failure, unspecified | Both systolic and diastolic dysfunction |
| I50.9 | Heart failure, unspecified | Use only when type cannot be determined |
Most common mistake: Using I50.9 (heart failure, unspecified) when echocardiographic documentation specifies systolic or diastolic dysfunction. I50.9 is considered a non-specific code — and payers increasingly flag it as inadequate documentation for procedures like echocardiograms (CPT 93306), heart failure management visits, and remote monitoring.
Documentation requirement: The type of heart failure (systolic vs. diastolic) must be documented by the treating cardiologist — not inferred by the coder. If the echocardiogram shows EF below 40 percent but the physician note does not specify systolic heart failure, the coder cannot use I50.22. Query the physician first.
Atrial Fibrillation and Flutter Codes
According to OmniMD’s cardiology coding guide, atrial fibrillation has four billable subtypes — and defaulting to I48.91 (unspecified) when the documentation supports a more specific code is one of the most common cardiology coding errors.
| ICD-10 Code | Description | When to Use |
|---|---|---|
| I48.0 | Paroxysmal atrial fibrillation | Episodes that terminate spontaneously within 7 days |
| I48.11 | Longstanding persistent atrial fibrillation | Continuous AF for more than 12 months |
| I48.19 | Other persistent atrial fibrillation | AF for more than 7 days, less than 12 months |
| I48.20 | Chronic atrial fibrillation, unspecified | Permanent AF (rate control only, rhythm not pursued) |
| I48.21 | Permanent atrial fibrillation | Permanent AF with documented clinical decision to accept |
| I48.91 | Unspecified atrial fibrillation | Only when type is truly undeterminable |
| I48.3 | Typical atrial flutter | Type I flutter (counterclockwise) |
| I48.4 | Atypical atrial flutter | Type II flutter (clockwise or variant) |
Most common mistake: Using I48.91 (unspecified) when the clinical record documents paroxysmal, persistent, or permanent AF. Query the cardiologist if the record is unclear — defaulting to unspecified is not acceptable when specificity is documented elsewhere in the chart.
Acute Myocardial Infarction (AMI) Codes
| ICD-10 Code | Description | Documentation Required |
|---|---|---|
| I21.01 | ST elevation MI of left main coronary artery | STEMI; left main; initial encounter |
| I21.02 | ST elevation MI of left anterior descending | STEMI; LAD; initial encounter |
| I21.09 | ST elevation MI of other sites | STEMI; other vessel; initial encounter |
| I21.11 | ST elevation MI of right coronary artery | STEMI; RCA; initial encounter |
| I21.19 | ST elevation MI of other inferior wall | STEMI; inferior; other vessel |
| I21.4 | Non-ST elevation myocardial infarction | NSTEMI; initial encounter |
| I21.9 | Acute MI, unspecified | Only when STEMI vs NSTEMI not documented |
| I22.0 | Subsequent STEMI of anterior wall | Second AMI within 4 weeks — initial encounter only |
Most common mistake: Using I21.9 (unspecified MI) when the ECG and cardiac enzyme results clearly distinguish STEMI from NSTEMI. According to OmniMD, always specify laterality and acuity in MI coding — I21 codes differ by STEMI/NSTEMI and vessel site.
Critical rule: AMI codes (I21.x) are used only during the first 4 weeks after infarction. For patients with resolved or remote MI, use I25.2 (old myocardial infarction). Using I21.x for a healed MI beyond 4 weeks generates automatic denial.
Valvular Heart Disease Codes
| ICD-10 Code | Description |
|---|---|
| I35.0 | Nonrheumatic aortic (valve) stenosis |
| I35.1 | Nonrheumatic aortic (valve) insufficiency |
| I35.2 | Nonrheumatic aortic (valve) stenosis with insufficiency |
| I34.0 | Nonrheumatic mitral (valve) insufficiency |
| I34.1 | Nonrheumatic mitral (valve) prolapse |
| I34.2 | Nonrheumatic mitral (valve) stenosis |
| I36.0 | Nonrheumatic tricuspid (valve) stenosis |
| I37.0 | Nonrheumatic pulmonary valve stenosis |
Most common mistake: Failing to distinguish rheumatic from nonrheumatic etiology. Rheumatic valvular disease uses I05.x through I09.x codes. Using a nonrheumatic code (I34.x–I37.x) when rheumatic etiology is documented — or vice versa — creates a clinical inconsistency that payer automated systems flag for audit.
Chest Pain and Symptom Codes — When They Are Appropriate
Chest pain and symptom codes have a specific role in cardiology billing — but they are frequently used incorrectly, generating medical necessity denials.
| ICD-10 Code | Description | When Appropriate |
|---|---|---|
| R07.9 | Chest pain, unspecified | Only when diagnostic workup is ongoing and no cause established |
| R07.89 | Other chest pain | Atypical presentations under active evaluation |
| R00.0 | Tachycardia, unspecified | Workup in progress, no diagnosis yet |
| R00.1 | Bradycardia, unspecified | Workup in progress, no diagnosis yet |
The most critical rule in cardiology ICD-10 coding: Symptom codes are only appropriate when a definitive diagnosis has not yet been established. Once a diagnosis is confirmed — even on the same encounter — the confirmed diagnosis code replaces the symptom code. Continuing to bill R07.9 after a diagnosis of CAD or unstable angina has been documented is a compliance violation that attracts payer audit attention.
The 8 Most Common Cardiology ICD-10 Coding Mistakes in 2026
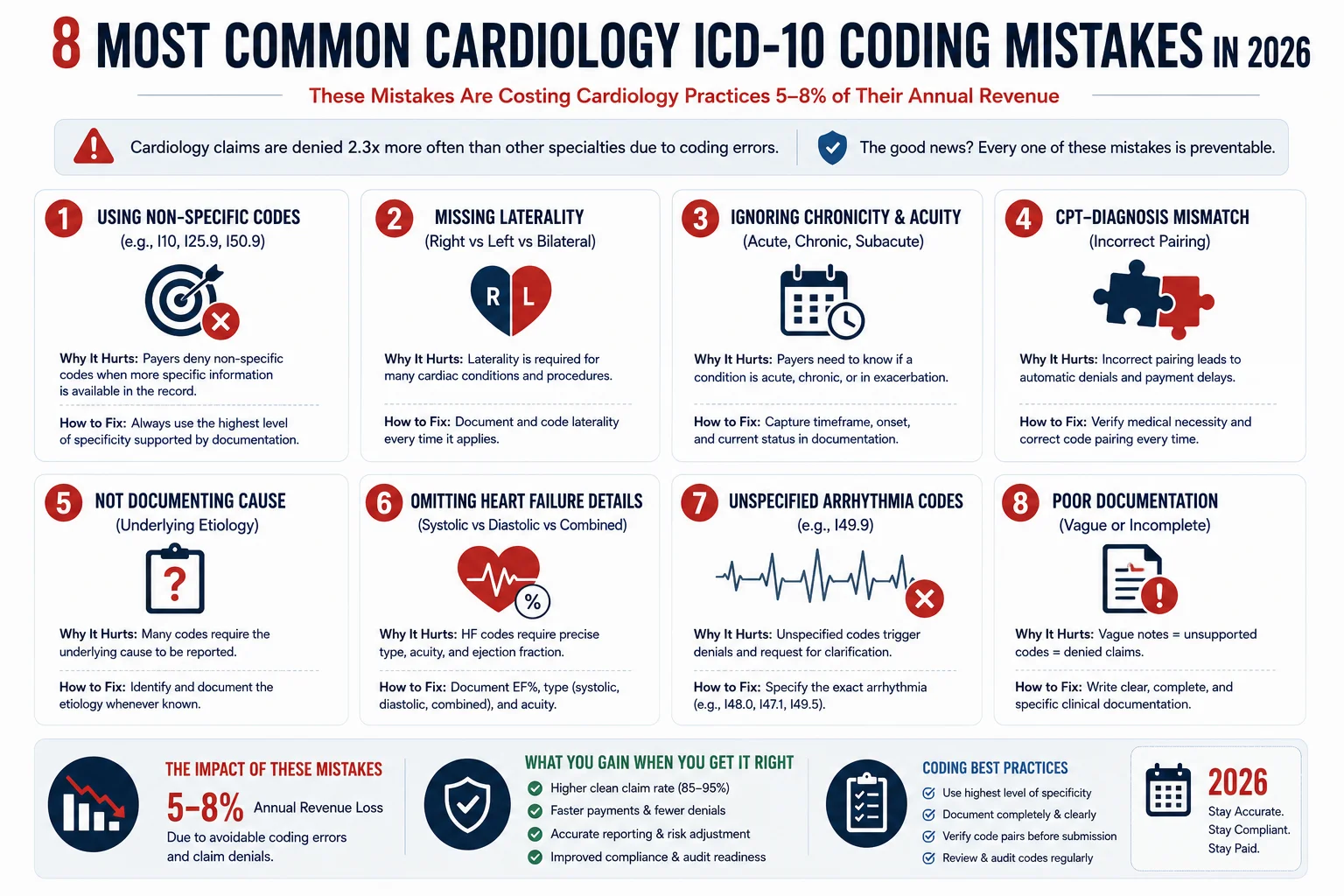
Mistake 1: Using Non-Specific Codes When Specificity Is Documented
Using I48.91 (unspecified atrial fibrillation) when the record documents paroxysmal AF. Using I50.9 (heart failure unspecified) when an echo documents systolic dysfunction. Using I25.10 (CAD without angina) when the patient has documented stable angina.
Non-specific codes generate lower reimbursement and increase audit risk. Payer automated scrubbers compare the specificity level of the ICD-10 code against the procedure being billed — and non-specific diagnosis codes paired with complex procedures are automatic red flags.
Fix: Every cardiology ICD-10 code should reflect the highest level of specificity the clinical documentation supports. If the documentation is ambiguous, query the physician before submitting.
Mistake 2: CPT-ICD Mismatch — Procedure Does Not Support Diagnosis
This is the fastest path to a medical necessity denial in cardiology. When the ICD-10 diagnosis code does not logically justify the procedure billed, payer systems deny the claim before it reaches human review.
Common examples:
- Cardiac catheterization (CPT 93454) billed with R07.9 (chest pain, unspecified) — denied
- Stress echocardiogram (CPT 93350) billed with I10 (hypertension only, no cardiac symptoms) — denied
- Ablation (CPT 93656) billed with I48.91 (unspecified AF) without documented clinical rationale — flagged for audit
Fix: Before submitting any complex cardiology procedure claim, verify that the ICD-10 code explicitly supports the medical necessity of the procedure. The diagnosis must tell the clinical story of why the procedure was performed.
Mistake 3: Missing Modifier -26 on Technical/Professional Component Splits
Cardiology diagnostic studies — particularly echocardiograms (CPT 93306), stress tests (CPT 93015–93018), and nuclear imaging (CPT 78451–78454) — often have separate professional and technical components. When billing the professional component only, modifier -26 must be appended.
According to Neolytix’s cardiology billing guide, missing or incorrect modifiers are a leading cause of automatic claim rejection in cardiology. When billing the global service (both components), no modifier is needed. When billing professional component only, append -26. When billing technical component only, append -TC.
Fix: Establish a modifier reference for every cardiology diagnostic code in your charge capture system — including whether the service is typically billed globally, professionally only, or technically only in your practice setting.
Mistake 4: Wrong PCI Vessel Modifier — LD, RC, LC, LI
Percutaneous coronary intervention (PCI) claims require vessel-specific modifiers that identify which coronary artery was treated:
| Modifier | Vessel |
|---|---|
| LD | Left anterior descending coronary artery |
| LC | Left circumflex coronary artery |
| RC | Right coronary artery |
| LI | Left main coronary artery |
| RI | Ramus intermedius |
According to MediBill RCM’s CPT guide, missing modifiers on PCI claims — especially failing to append LD, RC, or LC — are among the top denial triggers in interventional cardiology. Every PCI claim must identify the vessel treated.
Fix: Build a pre-submission check that confirms vessel modifier presence on every PCI claim before it leaves your system.
Mistake 5: Billing Diagnostic Angiography Separately When Bundled With PCI
When a diagnostic coronary angiography is performed on the same day as a PCI in the same vessel, CMS bundles the angiography into the PCI payment. Billing for the angiography separately generates an automatic CO-97 bundling denial.
Exception: If the angiography was medically necessary as a separate procedure in a different vessel, modifier -59 (or XU, XS, XE, XP) may apply — but this requires explicit documentation of the separate clinical indication.
Fix: Review NCCI edits before submitting any combined angiography and PCI claims. If separate billing is justified, document the specific clinical reason and append the correct unbundling modifier. For more on bundling denial codes, see our medical billing denial codes guide.
Mistake 6: Using AMI Codes Beyond 4 Weeks
Using acute MI codes (I21.x) for patients with healed myocardial infarction beyond the 4-week acute period. After 4 weeks from the date of infarction, the correct code is I25.2 (old myocardial infarction).
Fix: Track MI dates in your practice management system. Any encounter more than 28 days after the acute MI date should use I25.2, not I21.x.
Mistake 7: Global Period Billing Errors on Post-Procedure Visits
Many cardiology procedures — cardiac catheterizations, ablations, device implantations — carry 10-day or 90-day global periods. Billing separately for follow-up visits, complication management, or re-interventions within the global period without proper documentation and modifiers generates automatic denial.
Fix: Maintain a global period tracker in your billing system. When a follow-up visit occurs within the global period, confirm whether the service falls within or outside the global package before submitting. If outside, document the specific clinical reason and append the appropriate modifier.
Mistake 8: Symptom Codes After Diagnosis Is Established
Using chest pain (R07.9), palpitations (R00.2), or dyspnea (R06.0) codes on claims after a definitive diagnosis has been documented in the medical record.
This is a compliance risk — not just a coding error. Continuing to bill symptom codes for conditions that have been diagnosed can be interpreted as miscoding, which attracts OIG scrutiny. According to Pace Plus’s ICD-10 error analysis, the use of symptom codes after a definitive diagnosis is established is one of the most flagged errors in automated payer audits.
Fix: Train providers and coding staff that symptom codes are only appropriate when the cause has not yet been determined. Once a diagnosis is made, the diagnosis code replaces all symptom codes — even on the same visit.
Documentation Requirements That Prevent the Most Common Denials
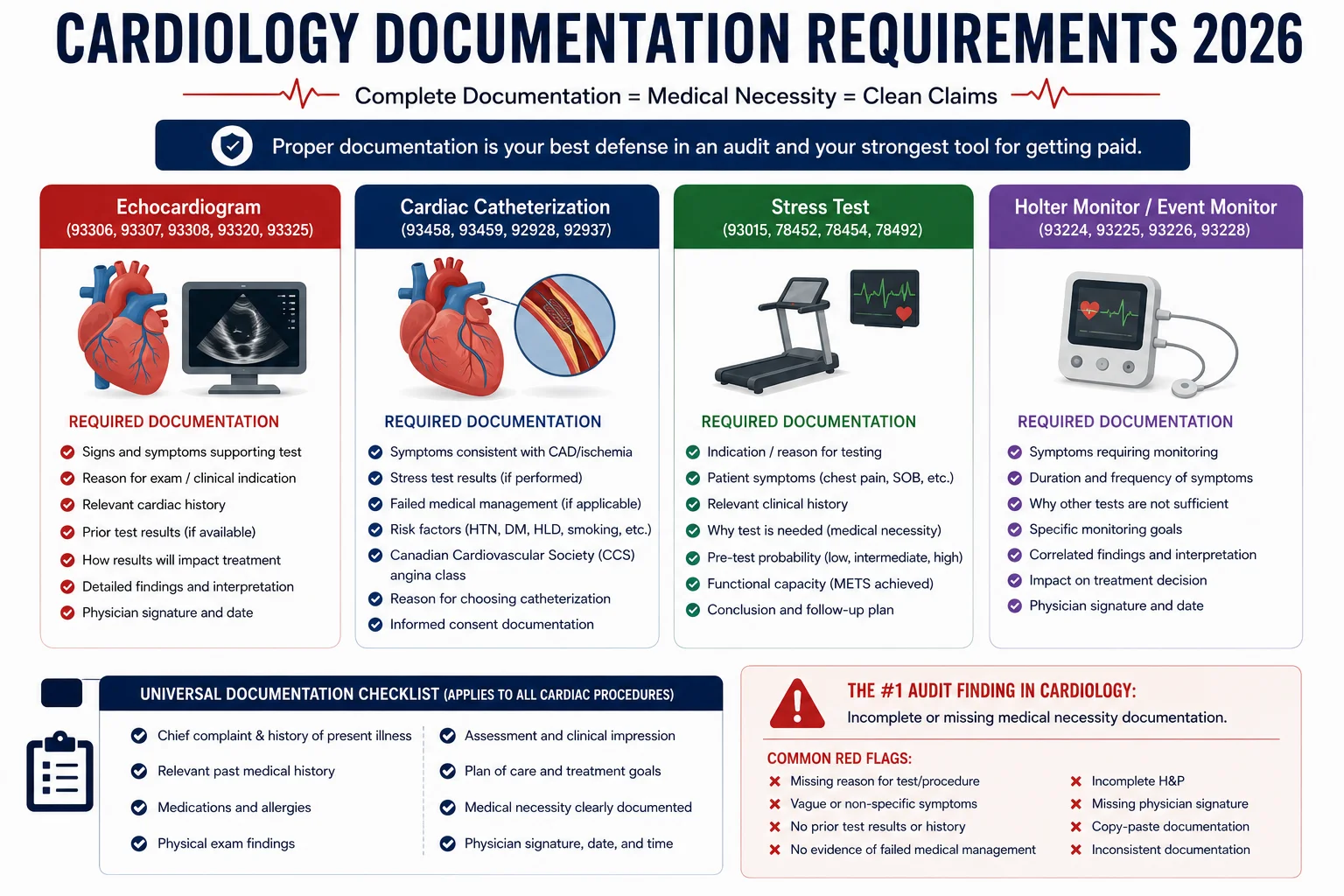
The most common denial reason in cardiology — after coding errors — is insufficient documentation of medical necessity. Here is what each major cardiology procedure requires in the clinical record to support its claim:
Echocardiogram (CPT 93306): Signed cardiologist interpretation report is required for Part B billing. Clinical indication documented in the order. If prior echo was performed within 12 months, clinical change or new indication must be documented.
Stress Test (CPT 93015–93018): Clinical indication (symptoms, risk factors, monitoring post-intervention). Contraindications to exercise stress reviewed and documented. Results of the test documented in a separate interpretation report.
Cardiac Catheterization (CPT 93454–93461): Specific clinical indication documented — not just “chest pain.” Prior non-invasive testing results. Documentation of why invasive testing is necessary given the clinical picture.
PCI (CPT 92928, 92929): Degree of stenosis — typically 70 percent or more for elective PCI, or hemodynamic significance documented for borderline lesions. Specific vessel treated and modifier confirmed. IVUS or FFR results if applicable.
Electrophysiology Study (CPT 93600–93641): ECG documentation of the arrhythmia. Failure of medical management documented. Specific indication for EP study beyond symptom reporting.
Nuclear Stress Test (CPT 78451–78454): Prior stress test results and why nuclear imaging is now needed. Clinical symptoms or findings that justify nuclear over standard stress testing. Cardiologist interpretation signed separately from the technician’s report.
For more on how documentation gaps generate specific denial codes, see our complete medical billing denial codes guide.
Prior Authorization in Cardiology — What Requires It in 2026
According to Neolytix’s cardiology guide, many cardiology procedures require prior authorization — and authorization failures are among the most expensive denial reasons in the specialty.
Procedures typically requiring prior authorization from major payers in 2026:
- Cardiac catheterization (most commercial payers and Medicare Advantage)
- PCI and stent placement
- Transcatheter aortic valve replacement (TAVR)
- Electrophysiology studies and ablations
- Device implantation (pacemakers, ICDs, CRT devices)
- Nuclear stress testing (Medicare Advantage and commercial payers)
- Advanced imaging (cardiac MRI, CT angiography)
Medicare fee-for-service does not require prior authorization for most cardiac procedures, but Medicare Advantage plans do — and with more than 51 percent of Medicare beneficiaries now in MA plans, prior authorization management is essential for practices with significant Medicare volume.
For more on the 2026 prior authorization rule changes and how to build systematic PA workflows, see our prior authorization rules guide.
How Pro Health Care Advisors Handles Cardiology ICD-10 Billing
Our cardiology billing services are built around the specific coding, documentation, and audit requirements of cardiovascular practice — with AAPC-certified coders who specialize in cardiology billing and understand the difference between billing an echo correctly and generating a denial.
Here is specifically what we do for cardiology practices:
AAPC-certified cardiology coding review. Every claim is reviewed by coders with specific cardiology coding experience — verifying ICD-10 specificity, CPT-diagnosis alignment, modifier accuracy, and vessel specification on PCI claims before submission. Our CodeMAXX services add a dedicated coding accuracy layer.
Pre-submission bundling edit review. We check every cardiology claim against NCCI edits before submission — catching the bundling errors that generate CO-97 denials on same-day angiography and PCI claims.
Prior authorization management. We maintain payer-specific authorization requirement tracking for cardiac catheterizations, ablations, device implants, and advanced imaging — preventing the CO-15 denials that occur when authorization is obtained incorrectly or not at all.
RAC audit protection. Our MD Audit Shield RAC service provides documentation review and audit response preparation specifically for cardiology practices facing RAC scrutiny on high-value cardiac procedures.
Global period tracking. We maintain global period records for all cardiology procedures — flagging post-procedure visits that fall within global periods and ensuring correct modifier use for services that fall outside.
HIPAA-compliant billing security. Cardiology practices handle sensitive cardiovascular patient data. Our HIPAA compliance services protect the data security of all cardiology billing operations.
The result: a 98.5 percent clean claim rate and a denial rate under 2 percent — in a specialty where the average clean claim rate is 78 to 82 percent.
Frequently Asked Questions — ICD-10 Codes for Cardiology 2026
Q: What is the most commonly used ICD-10 code in cardiology? I10 (essential hypertension) appears in approximately 60 percent of cardiovascular encounters, making it the most frequently billed cardiology diagnosis code. However, when hypertension has caused cardiac or renal complications, more specific codes (I11.x, I12.x, I13.x) must be used instead.
Q: What ICD-10 codes are used for atrial fibrillation in 2026? Atrial fibrillation has four billable subtypes: I48.0 (paroxysmal), I48.11 (longstanding persistent), I48.19 (other persistent), I48.20 (chronic, unspecified), and I48.21 (permanent). I48.91 (unspecified) should only be used when the type is truly undeterminable. Defaulting to unspecified when the record documents a specific subtype is a coding error.
Q: What is the difference between I21.x and I25.2 for myocardial infarction? I21.x codes are used for acute MI during the first 4 weeks after infarction. After 4 weeks, the MI is considered healed and coded as I25.2 (old myocardial infarction). Using I21.x beyond 4 weeks is a compliance error that generates denial and audit risk.
Q: Why do cardiology practices have lower clean claim rates than other specialties? Cardiology coding requires more specificity than most specialties — vessel laterality, episode of care, chronicity, and acuity all affect code selection. CPT-diagnosis alignment is closely audited by payer automated systems. And prior authorization requirements are more extensive than in most specialties. These factors combine to create a structurally more complex billing environment where errors are easier to make and more expensive when they occur.
Q: What modifiers are required for PCI claims? PCI claims require vessel-specific modifiers: LD (left anterior descending), LC (left circumflex), RC (right coronary artery), LI (left main), or RI (ramus intermedius). Missing these modifiers generates automatic denial. Multiple vessel PCI requires separate claim lines with appropriate modifiers for each vessel.
Q: How do prior authorization requirements for cardiology differ between Medicare and Medicare Advantage? Traditional Medicare fee-for-service does not require prior authorization for most cardiac procedures. Medicare Advantage plans do — and each MA plan has its own authorization requirements, documentation standards, and decision timelines. With more than 51 percent of Medicare beneficiaries now in MA plans, cardiology practices must maintain payer-specific authorization workflows for every major MA carrier in their market.
For more billing education and resources, visit our articles and resources library.

The Bottom Line — Cardiology Billing Rewards Precision and Punishes Shortcuts
Cardiology ICD-10 coding is not forgiving. A single missing modifier, a non-specific diagnosis code, or a CPT-diagnosis mismatch can deny a claim worth thousands of dollars — and in a specialty with RAC audit activity running above the national average, coding errors do not just cost you one claim. They create audit trails that generate recoupments reaching back months.
The practices that maintain clean claim rates above 90 percent in cardiology are not relying on general billing knowledge. They have AAPC-certified coders who specialize in cardiovascular coding. They verify CPT-ICD alignment on every claim before submission. They track global periods, vessel modifiers, and authorization requirements systematically. And they review their denial patterns monthly to catch the same errors before they repeat.
Pro Health Care Advisors builds exactly that kind of cardiology billing operation for practices across the country — with a 98.5 percent clean claim rate and a denial rate under 2 percent in a specialty where the average falls well short of both benchmarks.
If your cardiology practice is losing revenue to ICD-10 coding errors, CPT-diagnosis mismatches, or modifier mistakes — that is a billing process problem with a specific, fixable solution.
Schedule Your Free Consultation with Pro Health Care Advisors →
No pitch. No pressure. Just a real review of your cardiology billing performance and a clear picture of what better coding looks like for your practice.