Medical Billing in 2026 | The Complete Guide for Private Practices
Medical Billing in 2026 — It Is Not What It Used to Be
Ask any practice manager what keeps them up at night in 2026, and billing comes up almost every time.
Not because it is a new problem. Medical billing has always been complicated. But something shifted in the last two years that made “complicated” feel like an understatement. Payers are tighter. Denial rates are higher. Documentation requirements are more specific. Patients owe more out of pocket and are paying more slowly. And the technology gap between practices running modern billing systems and those still relying on manual workflows is now wide enough that it directly shows up in collections.
Medical billing is no longer a back-office task you hand to a staff member and forget about. In 2026, it is a strategic function — one that either protects your revenue or quietly drains it depending on how well your process is working.
This guide covers everything a private practice needs to understand about medical billing right now: what the term actually covers, what is changing in 2026, the most common reasons practices lose money they already earned, and how to know whether your current billing setup is working or slowly costing you.
From the ProHealth Care Advisors team: We help private practices across Georgia and nationally with billing, revenue cycle management, and prior authorization support. Everything in this guide reflects the current state of medical billing as of May 2026. Visit ProHealth Care Advisors to talk through your specific situation.
What Medical Billing Actually Covers — The Full Picture
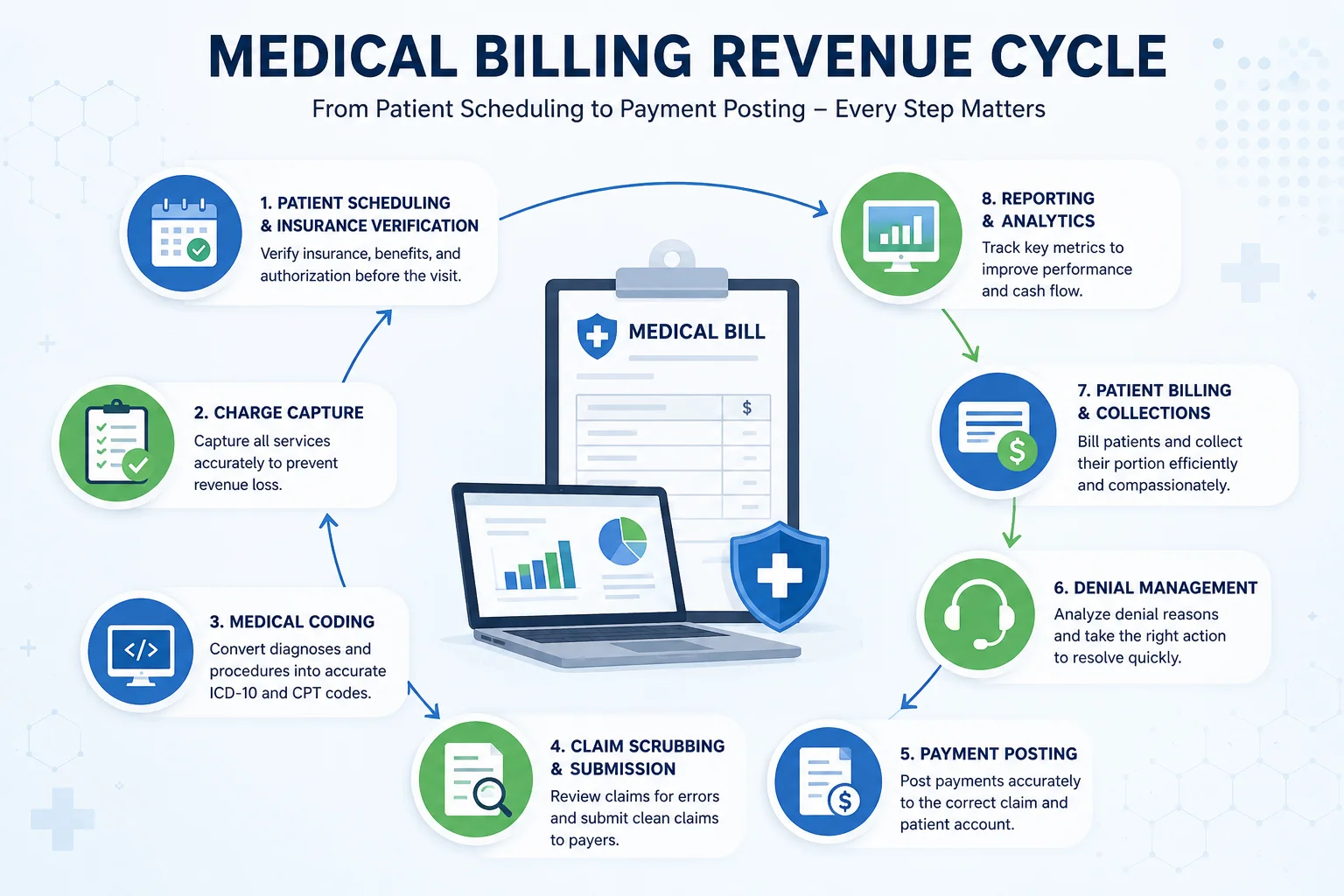
A lot of people use “medical billing” to mean just one thing — submitting a claim to an insurance company. But the term covers an entire chain of connected steps, and a weakness anywhere in that chain affects the revenue at the end of it.
Here is what the full medical billing process actually involves:
Patient scheduling and insurance verification. Before a single patient is seen, billing starts. Checking that the patient’s insurance is active, confirming that your practice is in-network, and identifying any prior authorization requirements before the appointment happens — all of this determines whether the claim that follows will go through cleanly or bounce back.
Charge capture. After the visit, the services provided need to be captured accurately and completely. Missed charges — services that were provided but never billed — are one of the most common and most preventable sources of revenue loss in private practice.
Medical coding. Every diagnosis and every procedure gets translated into standardized codes — ICD-10 codes for diagnoses, CPT codes for procedures. Coding errors are the most common reason claims are denied on first submission. A wrong modifier, a mismatched code pair, or a code that is not supported by the documentation will trigger a rejection.
Claim scrubbing and submission. Before a claim goes to the payer, it should be reviewed — or “scrubbed” — for errors. Practices using modern systems do this electronically and automatically. Practices relying on manual review miss errors that automated systems catch consistently.
Payment posting. When the insurance company pays, that payment needs to be posted accurately against the right claim and the right patient account. Errors here create confusion in the AR and can cause follow-up on accounts that were actually paid — wasting staff time on work that does not need to be done.
Denial management. When claims are rejected or denied, they need to be worked — quickly and specifically. The denial reason tells you what went wrong, and different types of denials require different responses. This is the step where most practices leave the most money behind.
Patient billing and collections. After insurance pays its share, the patient’s portion needs to be billed and collected. In 2026, patients carry a larger share of their healthcare costs than at any point in the past decade — which means patient collections are both more important and more difficult than they used to be.
Reporting and analytics. A billing operation without reporting is flying blind. Key metrics — clean claim rate, denial rate, days in accounts receivable, net collection rate, and cash flow timing — tell you whether your billing is performing or silently underperforming.
Each of these steps can go wrong independently. And when multiple steps have gaps, the effect on revenue is compounding.
What Changed in Medical Billing in 2026 — The Honest Summary
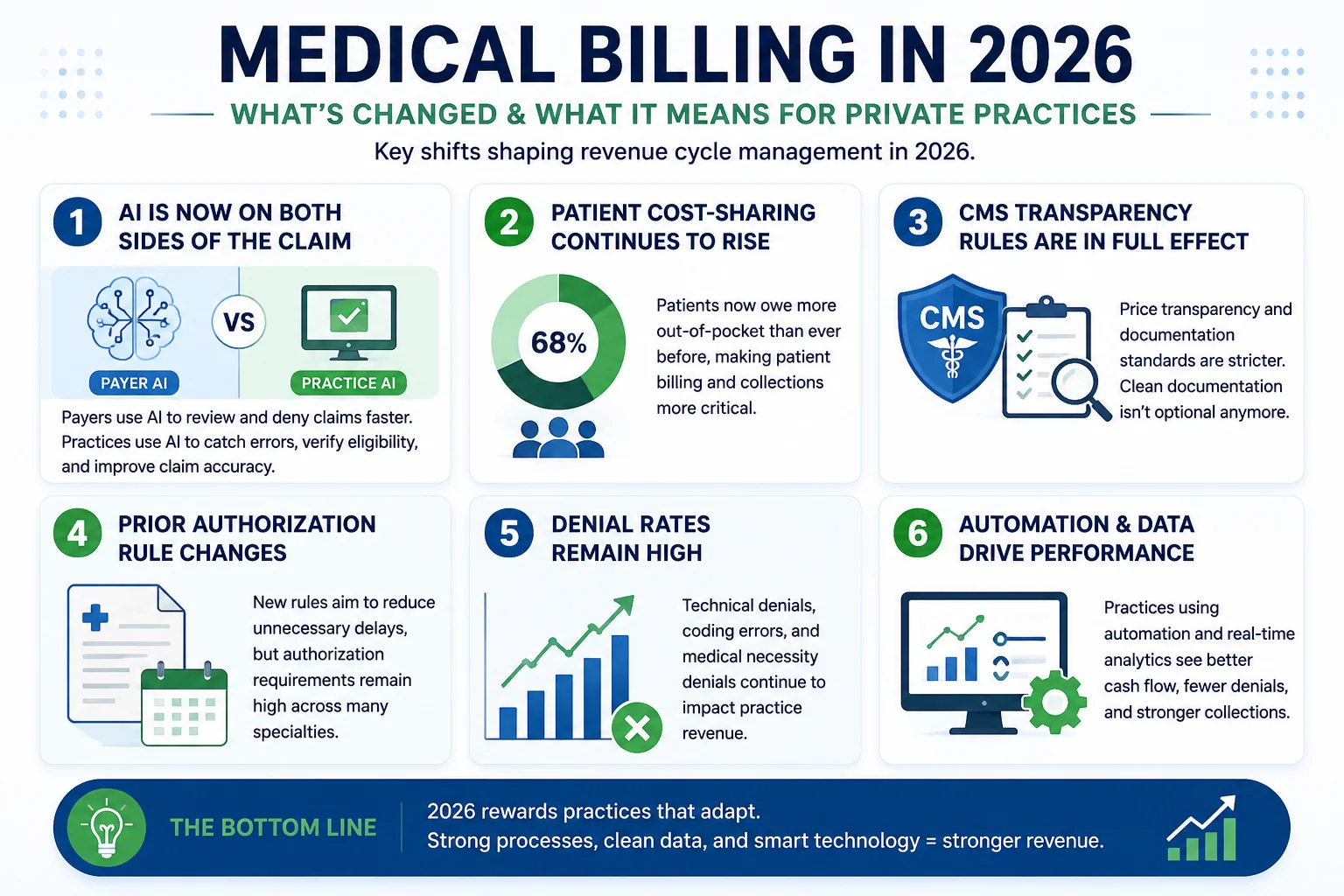
2026 brought several changes to medical billing that private practices are still adjusting to. Here is the plain-language summary of what shifted.
AI Is Now on Both Sides of the Claim
Payers have deployed AI-powered claim review algorithms that process prior authorization requests and claims in seconds — often without meaningful human review. These algorithms flag outlier claims, deny requests that fall outside expected documentation patterns, and reject code combinations that look inconsistent to the system even when they are clinically accurate.
According to Guidehouse research, investments in medical billing automation — including AI-powered coding support, payer analytics, and prior authorization tools — ranked as the top revenue cycle management priority for medical groups in 2026. Practices that are using AI on their own side to catch errors before submission are dramatically outperforming practices that are not. Practices using AI-assisted claim scrubbing are catching documentation mismatches and eligibility gaps before the claim ever leaves the office.
The practical implication: if your billing process does not include some form of pre-submission claim review — automated or manual — you are sending claims blind into a system that is actively looking for reasons to deny them.
Patient Financial Responsibility Kept Growing
A 2025 Gallup survey found that 12 percent of U.S. adults — roughly 31 million Americans — borrowed approximately $74 billion in the past year specifically to cover healthcare costs. A separate 2024 consumer study found that 72 percent of patients view affordability as their biggest challenge when paying larger healthcare bills, and 47 percent said difficulty paying a bill hurt their overall wellbeing or recovery.
For private practices, this means patient collections in 2026 are both more consequential and more sensitive. Patients who cannot easily pay their bills after insurance processes are not simply slow payers — they are people navigating real financial stress. The practices that handle this well — offering payment plans, providing upfront cost estimates, making the billing process easy to understand — collect more and maintain better patient relationships simultaneously.
Price Transparency Requirements Are Real
Regulations requiring healthcare providers to post prices publicly have shifted patient expectations in a concrete way. Patients now arrive with price comparisons already done. They want to know their out-of-pocket cost before they receive care — not after they receive a bill. Practices that cannot provide accurate cost estimates at the point of scheduling are losing patients to practices that can.
Billing teams now need to coordinate with front desk staff on cost estimate workflows. The financial conversation that used to happen at checkout needs to happen at scheduling.
CMS 2026 Rules Changed the Payer Accountability Landscape
The CMS Interoperability and Prior Authorization Final Rule — CMS-0057-F — went into effect January 1, 2026. For medical billing specifically, the most important changes are:
Standard prior authorization decisions must now come back within 7 days. Urgent decisions within 72 hours. Every denial must include a specific clinical reason rather than a vague rejection code. Payers must publicly report their approval and denial rates.
These changes shifted accountability in a direction that helps practices — but only if billing teams know the rules and use them. Specific denial reasons mean specific appeal arguments. Documented response timelines mean practices can escalate when payers are non-compliant. Public reporting data means practices can identify high-denial payers on specific service types and build stronger first submissions.
For the full breakdown of the 2026 prior authorization rule changes, see our Prior Authorization Rules Changed 2026 guide.
Telehealth Billing Is Growing But Still Inconsistent
Telehealth has become a permanent part of private practice care delivery. But telehealth billing remains one of the most inconsistent areas in the revenue cycle. Coverage varies by payer. Audio-only visit coverage differs from video visit coverage. Documentation requirements vary. Modifier use varies. Some payers have extended pandemic-era telehealth flexibilities permanently. Others have rolled them back.
The practices losing the most telehealth revenue are those whose billing teams learned the rules for one or two major payers and assumed they applied across the board. In 2026, telehealth billing requires payer-specific policies to be tracked actively — not assumed from general knowledge.
The Most Common Ways Private Practices Lose Money in Medical Billing
This is the part that matters most for practices that feel like they should be doing better financially than their billing reflects.
Leaving Claims in the Denial Queue
Industry data consistently shows that 65 percent of denied claims are never reworked or appealed. The time pressure of daily operations means denials pile up and get reviewed “later” — and later often never comes. For a practice with a 10 percent denial rate on a $1.5 million annual billing volume, that pile of unworked denials represents $150,000 in submitted revenue sitting without follow-up.
Missing Charges at the Point of Care
Charge capture errors — services provided but not billed — are invisible by definition. You do not see what was never entered. Common sources include injections or supplies used during procedures, extended visit times that justify a higher evaluation and management code, new patient codes applied to established patients, and telehealth visits that were not properly flagged for billing.
Eligibility Verification Done Once and Not Again
A patient’s insurance that was active at scheduling may have changed by the date of service. In 2026, with approximately 2.9 million Medicare Advantage patients displaced into new plans, this risk is higher than at any point in recent years. Verifying eligibility at scheduling but not again on the date of service is the most common single source of preventable denials in 2026.
Coding That Does Not Match the Documentation
This gap works in two directions. Undercoding — billing for a lower-complexity service than what was actually provided — happens when clinicians default to familiar codes rather than the codes their documentation supports. Overcoding — billing for more than what is documented — creates compliance risk. Both are problems. The fix is regular coding audits that compare what is being billed against what the documentation actually supports.
Slow Patient Collections Without a Follow-Up Process
Billing a patient once and waiting is not a collections process. In 2026, effective patient collections requires timely statements, multiple contact methods, early identification of patients who need payment plans, and a clear escalation path for accounts that age beyond a certain threshold. Practices without this structure collect a fraction of what they are owed in patient responsibility.
Not Knowing the Numbers
The most common billing problem of all is practices that do not track their own performance. If you do not know your clean claim rate, your denial rate, your days in AR, and your net collection rate by payer, you cannot see problems developing in time to fix them. Billing without metrics is reactive rather than managed.
For a structured look at how your current billing performance compares to 2026 benchmarks, our Revenue Cycle Health Check covers each of these metrics in detail.
In-House Medical Billing vs. Outsourcing — The Honest Comparison
This decision comes up for nearly every growing private practice. Here is the straightforward version.
In-house billing makes sense when: Your practice has a dedicated billing team of three or more people who do nothing other than billing. Your claim volume is high enough to keep them fully occupied without pulling them into other administrative tasks. You have the budget and time to keep that team trained on constant payer policy changes, coding updates, and compliance requirements. And you have clear reporting in place so you can measure whether their work is performing.
Outsourcing makes sense when: Your billing team is also handling front desk, scheduling, patient calls, and other tasks. You are experiencing denial rates above 8 percent without a clear plan to address the root causes. You are growing and do not want to hire additional billing staff. You want access to specialty-specific coding expertise without building it internally. Or you simply do not have the reporting visibility to know how your billing is performing right now.
The financial math for most small and mid-sized private practices in 2026 favors outsourcing. A qualified medical billing service charges 4 to 9 percent of collected revenue — and the improvement in clean claim rates, denial overturn rates, and cash flow timing typically more than offsets that cost against the combined expense of internal billing staff, training, and the revenue lost to unworked denials.
The practices that keep billing in-house successfully are the exception, not the rule — and they are usually larger groups with genuinely dedicated billing infrastructure.
For more on what to look for when evaluating a billing partner, see our Medical Billing Services page.
Medical Billing by Specialty — Why It Is Not One-Size-Fits-All
One of the most consistent findings in 2026 billing research is that generalist billing knowledge is no longer enough. Different specialties face genuinely different billing challenges, and a billing team built for one specialty may perform poorly in another.
Family medicine and primary care: High visit volume, complex evaluation and management coding, chronic care management billing, and growing telehealth volume. The challenge is coding accuracy at speed — and capturing all the add-on codes and time-based charges that are regularly missed.
Behavioral health and psychiatry: Payer coverage is inconsistent. Some plans cover 50 minutes of therapy; others cover 45. Documentation requirements for mental health services are specific and frequently audited. Telehealth billing for behavioral health has its own set of rules that differ from the general telehealth guidelines.
Orthopedics and pain management: Modifier-heavy coding. High prior authorization requirements. The WISeR model in six states now adds Medicare prior authorization requirements for specific orthopedic and pain procedures. One modifier used incorrectly on a surgical claim can deny the entire submission.
Cardiology: Complex procedure coding. High-cost imaging and diagnostic services with elevated prior authorization and medical necessity documentation requirements. Significant exposure to the Medicare Advantage denial trends discussed in our Medicare Advantage Denials Up 56% article.
OB/GYN and women’s health: Global billing packages for obstetric care create specific bundling complexities. Preventive service coding interacts with diagnostic coding in ways that trigger payer coordination issues if not handled carefully.
The point is not that every specialty needs a completely different billing system. It is that the billing team — whether in-house or outsourced — needs genuine specialty experience, not just general billing knowledge.
7 Things Your Medical Billing Process Must Include in 2026
Use this as a working checklist against your current setup.
1 — Real-time eligibility verification at scheduling and on the date of service. Not once. Twice. With 2.9 million Medicare Advantage patients in new plans and insurance changes happening constantly, eligibility data from even two weeks ago can be wrong today.
2 — Pre-submission claim scrubbing — automated if possible. Every claim should be reviewed for coding accuracy, documentation support, and payer-specific requirements before it leaves your practice. This is where clean claim rates are built.
3 — A specific process for working denials the same day they are received. Denials need to be routed, triaged, and assigned the day they arrive — not batched at the end of the month. A denial that sits for 30 days before being worked may miss the payer’s appeal deadline.
4 — Specialty-specific coding expertise. Your billing team needs to know the specific codes, modifiers, and documentation requirements for your specialty. General billing knowledge is not sufficient in 2026.
5 — Patient cost estimate capability at the point of scheduling. Patients expect to know their out-of-pocket cost before they arrive. Practices that provide this information at scheduling collect more from patients and receive fewer post-service billing disputes.
6 — Regular coding audits — at minimum quarterly. Audits catch undercoding, overcoding, and documentation gaps before they become compliance problems or persistent claim failures.
7 — Monthly reporting on the metrics that matter. Clean claim rate. Denial rate. Days in accounts receivable. Net collection rate. Appeal overturn rate. If you do not track these numbers monthly, you are managing your billing by feel rather than by data.
For help building any of these processes, our Medical Billing and Practice Management services are built specifically for private practices.
Medical Billing in Georgia — What Makes the State Market Specific
Georgia private practices operate in a billing environment that has some layers specific to this state — and a good billing operation needs to account for them.
Georgia Medicaid through managed care organizations. Georgia Medicaid operates through three CMOs: Amerigroup, Peach State Health Management, and WellCare. Each has different prior authorization requirements, different timely filing windows, and different documentation standards layered on top of the CMS baseline rules. A billing team that treats Georgia Medicaid as a single uniform payer will miss plan-specific requirements consistently.
The GAMMIS portal and 2026 enrollment requirements. Georgia Medicaid’s management system — GAMMIS — implemented multi-factor authentication requirements in 2026. The Group/Billing Enrollment Requirement that took effect January 1, 2026 added another layer of enrollment complexity. Billing teams that are not current on GAMMIS compliance risk claims being delayed or rejected at the system level.
Georgia Pathways billing complexity. The Medicaid Pathways extension brought working-age adults with employment requirements into Georgia Medicaid coverage. Billing for this population requires understanding the documentation standards tied to their eligibility criteria — something not every billing team has been trained on.
Fragmented commercial payer market. Georgia private practices regularly bill to BCBS of Georgia, Cigna, Aetna, UnitedHealthcare, Humana, and multiple regional carriers — each with distinct timely filing limits, fee schedules, and modifier requirements. Tracking these differences accurately is one of the most time-consuming parts of Georgia private practice billing.
For a detailed guide to Georgia-specific billing requirements, see our Georgia Medical Billing Guide for Private Practices.
External resource: Georgia Department of Community Health — Medicaid Provider Portal for current Georgia Medicaid billing requirements.
Frequently Asked Questions — Medical Billing 2026
What is medical billing and how does it work?
Medical billing is the process of submitting and following up on claims with health insurance companies to receive payment for healthcare services. It covers everything from verifying a patient’s insurance before an appointment, to coding the services provided, submitting the claim, managing any denials, and collecting the patient’s remaining balance after insurance pays. A complete billing cycle for a single patient encounter can take days to weeks depending on the payer and whether the claim is accepted on first submission.
What is a clean claim rate and why does it matter?
A clean claim rate is the percentage of claims your practice submits that are accepted and paid without needing to be corrected or resubmitted. The industry target is 95 percent or higher. A clean claim rate below 95 percent means more than 1 in 20 of your claims is requiring additional work after submission — which costs staff time, delays cash flow, and risks missing timely filing limits if the follow-up is slow.
What is a good denial rate for a private practice?
A denial rate below 5 percent is the benchmark most revenue cycle professionals use as a target. If your practice is above 8 percent, that is a signal that something in the billing workflow — eligibility verification, documentation, coding, or claim scrubbing — has a gap that needs to be addressed. High denial rates compound over time because unworked denials age out of appeal eligibility.
How much does it cost to outsource medical billing?
Most medical billing services charge between 4 and 9 percent of collected revenue. The percentage varies by specialty, claim volume, and scope of services included. Behavioral health and lower-volume specialties tend to sit at the higher end. The cost comparison against in-house billing should factor in staff salary, benefits, training, software, and the revenue impact of unworked denials — not just the headline percentage.
What is the difference between medical billing and medical coding?
Medical coding is the step within billing where diagnoses and procedures are translated into standardized codes — ICD-10 codes for diagnoses and CPT codes for procedures. Medical billing is the broader process that includes coding as one of its steps, along with claim submission, denial management, payment posting, and patient collections. Some billing services include coding; others expect the practice to provide coded superbills.
How do I know if my medical billing is performing well?
The key numbers to review are: clean claim rate (target 95%+), denial rate (target under 5%), days in accounts receivable (target under 35 for most specialties), net collection rate (target 95–98%), and appeal overturn rate. If you do not currently have visibility into all of these numbers, that is the first gap to fix. Our Revenue Cycle Health Check is designed to surface these metrics for practices that do not have clear reporting right now.
What is accounts receivable (AR) in medical billing?
Accounts receivable refers to the total amount your practice is owed but has not yet collected — money that is owed by insurance companies, patients, or both. Days in AR measures the average number of days it takes from when a service is provided to when payment is received. High days in AR means cash flow is slower than it should be. Anything above 45 days for most specialties signals that something in the billing cycle is causing payment delays.
Should a small private practice outsource medical billing?
For most small practices — those with fewer than five providers or a dedicated billing team of fewer than two people — outsourcing to a qualified medical billing service is the financially stronger choice in 2026. The improvement in clean claim rates, denial management, and cash flow timing typically more than offsets the billing service cost. The practices that keep billing in-house most successfully are larger groups with genuinely dedicated billing infrastructure and strong internal reporting.