Medical Billing vs Medical Coding: The Ultimate 2026 Guide to 7 Key Differences
Walk into any medical office in America and you will hear both terms used in the same breath — medical billing and medical coding. Ask most people what the difference is and you will get a vague answer about “paperwork” and “insurance.”
Here is the truth: medical billing vs medical coding is one of the most confused topics in all of healthcare administration — and that confusion costs doctors, practice managers, and patients real money every single day.
These are two distinct roles, two completely different skill sets, and two separate steps in the healthcare revenue cycle. Treating them as the same thing — or hiring one person and expecting them to do both without proper training — is one of the most common and costly mistakes a small medical practice can make.
In this guide, we are going to clear up the confusion around medical billing vs medical coding once and for all. You will learn exactly what each role does, where they overlap, how they differ, what each pays in 2026, which certifications matter, and — most importantly — how understanding the difference makes your practice run cleaner and get paid faster.
Whether you are a physician, a practice manager, or someone considering a career in healthcare administration, this is the guide you need.
The One-Sentence Answer to “Medical Billing vs Medical Coding”
Before we go deep, here is the clearest possible answer:
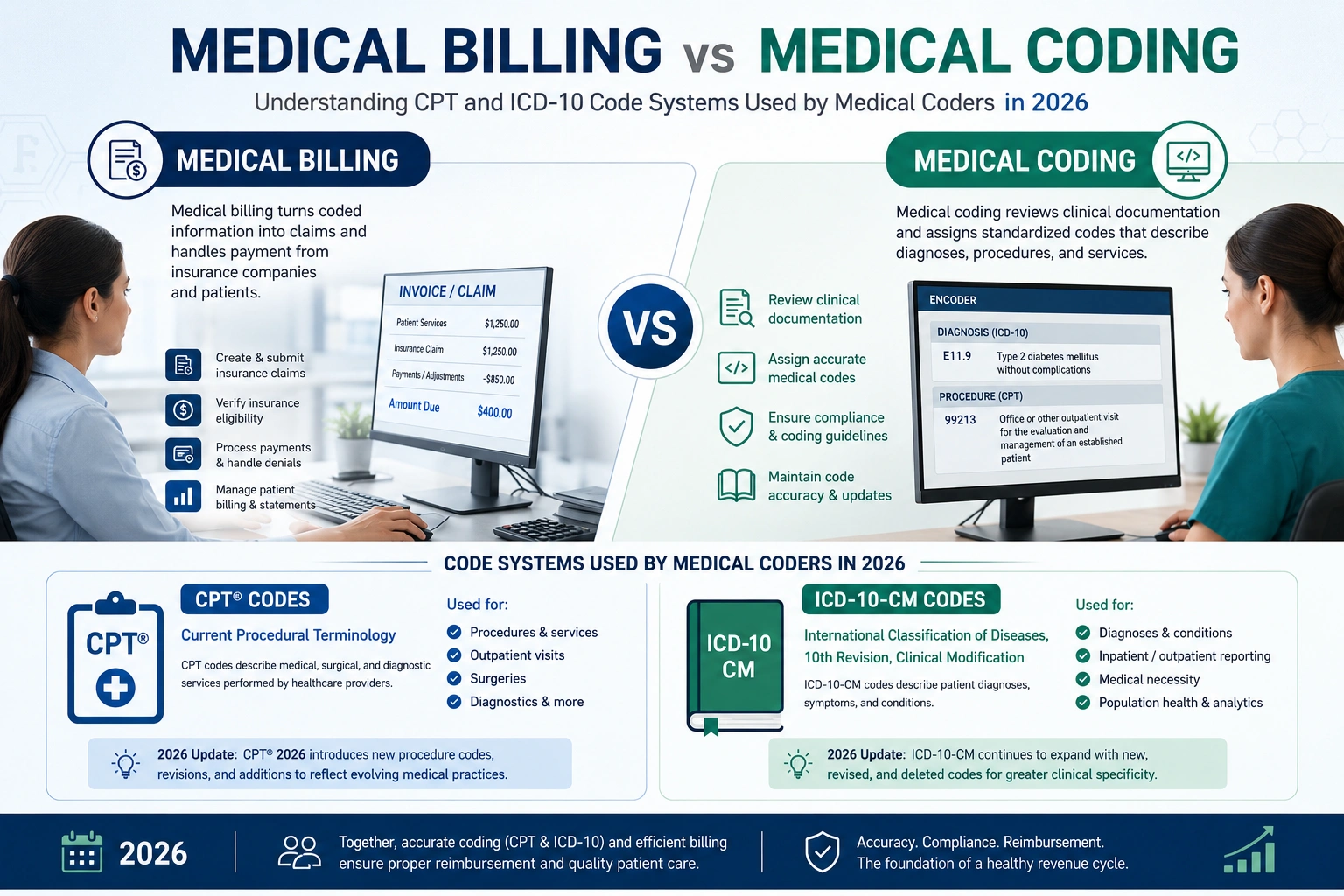
Medical coders translate what happened clinically into standardized codes. Medical billers use those codes to get your practice paid.
That is the core distinction. Everything else is detail built on top of that foundation.
A medical coder reads a physician’s note after a patient visit and converts the diagnosis and every procedure performed into specific numeric and alphanumeric codes — from standardized code sets like ICD-10, CPT, and HCPCS. The coder does not talk to insurance companies. They do not follow up on payments. They work entirely within clinical documentation.
A medical biller takes those codes, attaches them to a claim form, verifies the patient’s insurance coverage, submits the claim to the correct payer, follows up when the claim stalls, appeals when it gets denied, and manages the entire payment collection process until the practice receives its money.
Two separate steps. Two separate skill sets. Two separate roles — that work in sequence, not in parallel.
Now let us go through the seven key differences in detail.
7 Key Differences: Medical Billing vs Medical Coding
Difference #1: What Each Role Actually Does Every Day
What a Medical Coder Does:
A medical coder’s day revolves entirely around clinical documentation. They receive physician notes, operative reports, discharge summaries, lab results, and radiology reports — and their job is to translate everything that happened during that patient encounter into standardized codes.
The primary code systems they work with are:
- ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) — used to code diagnoses. Every condition, symptom, and reason for the visit gets an ICD-10 code. As of the October 2025 update, ICD-10-CM contains over 72,000 codes. The American Medical Association and CMS jointly maintain these standards.
- CPT (Current Procedural Terminology) — used to code procedures and services. Every injection, evaluation, surgery, therapy session, and diagnostic test has a CPT code. The AMA owns and updates CPT codes annually — 2026 includes 418 code changes from the previous year.
- HCPCS Level II — used primarily for supplies, equipment, drugs, and non-physician services that CPT does not cover. Common in billing for durable medical equipment, home health, and infusion therapy.
The coder’s output is a coded encounter record — a document that describes every clinical event in the numeric language that insurance companies and regulators understand.
What a Medical Biller Does:
A medical biller takes that coded encounter record and turns it into a financial claim. Their day involves:
- Verifying the patient’s insurance coverage and eligibility before or at each visit
- Building the CMS-1500 claim form (for physician services) or UB-04 form (for facilities) using the codes provided by the coder
- Submitting the claim electronically through a clearinghouse to the correct payer
- Monitoring claim status — tracking which claims are pending, which have been paid, and which have been denied
- Working denied claims — identifying the reason for denial, correcting the issue, and resubmitting or appealing
- Following up on unpaid claims as they age in accounts receivable
- Posting payments from insurance companies and patients
- Sending patient statements and managing patient collections
- Reporting on denial rates, collection rates, and revenue cycle performance
The biller lives at the intersection of clinical information and financial operations. They speak both the language of healthcare and the language of insurance — and they are the last line of defense between the care your practice delivered and the revenue your practice collects.
Difference #2: The Tools and Systems Each Role Uses
Medical Coders use:
- ICD-10-CM code books and encoder software
- CPT code books updated annually
- EHR/EMR systems to access clinical documentation
- Coding reference tools like 3M Encoder, TruCode, or Optum360
- Clinical documentation improvement (CDI) tools
- Anatomy and medical terminology references
- Compliance guidelines from CMS and payer LCDs (Local Coverage Determinations)
Medical Billers use:
- Practice management software (Epic, athenahealth, eClinicalWorks, AdvancedMD, DrChrono)
- Electronic clearinghouses (Availity, Change Healthcare, Office Ally)
- Insurance eligibility verification portals
- Electronic remittance advice (ERA) systems
- Accounts receivable management dashboards
- Patient billing and payment portals
- Denial tracking and appeals management software
The tools do not overlap much — which is a useful reminder that while both roles support the same goal (getting the practice paid), they operate in fundamentally different software environments and require different technical knowledge.
Difference #3: The Skills Each Role Requires
Skills a Medical Coder needs:
- Deep knowledge of anatomy, physiology, and medical terminology — without this, you cannot accurately translate clinical notes into codes
- Mastery of ICD-10, CPT, and HCPCS code sets, including their annual updates
- Understanding of coding guidelines from CMS, the AMA, and payer-specific rules
- Precision and attention to detail — a single wrong digit in a code can change the diagnosis entirely
- Ability to read and interpret complex clinical documentation
- Knowledge of modifier rules — when to add a modifier, which modifier, and why it matters for reimbursement
Skills a Medical Biller needs:
- Strong understanding of insurance plans, benefit structures, and payer-specific billing rules
- Knowledge of the claim lifecycle from submission to payment
- Communication skills — billers regularly speak with insurance company representatives, patients, and clinical staff
- Ability to read and interpret explanation of benefits (EOB) documents and denial reason codes
- Persistence and problem-solving — denial management requires figuring out what went wrong and how to fix it
- Basic accounting and financial reporting skills for accounts receivable management
- Familiarity with HIPAA regulations and patient privacy requirements — our HIPAA compliance page covers what practices need to know
The honest truth about medical billing vs medical coding skills: both require significant training and expertise. Neither is “easier” than the other — they are simply different. Coders need more clinical knowledge. Billers need more financial and communication knowledge.
Difference #4: Education and Certifications
Medical Coding Certifications (2026):
The two most respected coding credentials in the United States are:
- CPC (Certified Professional Coder) — offered by the AAPC (American Academy of Professional Coders). The CPC is the gold standard for physician office coding. It covers ICD-10, CPT, HCPCS, medical terminology, anatomy, and coding guidelines. According to AAPC, certified coders earn 20.7% more than non-certified coders.
- CCS (Certified Coding Specialist) — offered by AHIMA (American Health Information Management Association). The CCS is highly respected for inpatient hospital coding. It is considered more difficult than the CPC and commands higher salaries in hospital settings.
Other valuable coding credentials include:
- CCS-P (Certified Coding Specialist — Physician-based)
- CRC (Certified Risk Adjustment Coder) — provides 10–15% higher earnings
- CPMA (Certified Professional Medical Auditor)
- Specialty credentials in oncology, cardiology, orthopedics coding
Medical Billing Certifications (2026):
- CPB (Certified Professional Biller) — offered by AAPC. The most recognized billing-specific credential.
- CBCS (Certified Billing and Coding Specialist) — offered by NHA. Covers both billing and coding.
- CPC-A (Certified Professional Coder — Apprentice) — entry-level coding credential for new professionals.
Education requirements:
Neither medical billing nor medical coding requires a four-year college degree. Most employers look for:
- A postsecondary certificate (6 months to 2 years of training)
- At least one professional certification
- Some employers prefer an associate degree in health information technology or a related field
The Bureau of Labor Statistics projects 9% employment growth for medical records specialists from 2023 to 2033 — faster than the average for all occupations. Both billing and coding professionals are part of that growing demand.
Difference #5: Salary — Who Earns More in 2026?
This is one of the most searched questions in the medical billing vs medical coding conversation — and the answer is more nuanced than most sources admit.
Medical Coder Salaries in 2026:
| Experience Level | Annual Salary Range |
|---|---|
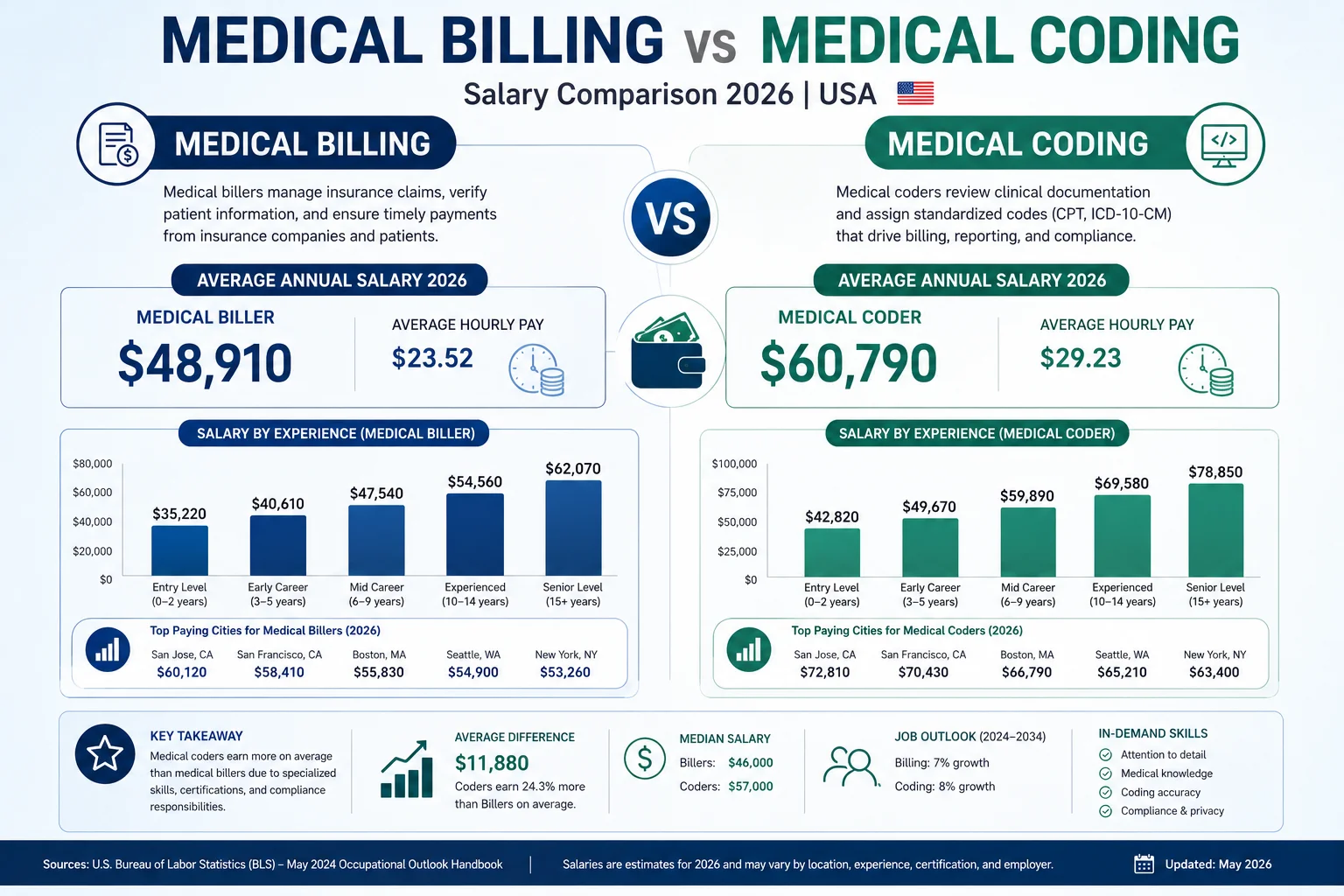
| Entry-level (0–2 years) | $34,500 – $42,000 |
| Mid-level (3–7 years) | $50,000 – $62,000 |
| Senior / Specialty Certified | $65,000 – $85,000 |
| CDI Specialist (hospital) | $70,000 – $85,000 |
| Remote coder (national average) | $43,482 – $50,887 |
Source: BLS, AAPC 2026 Annual Salary Survey, Research.com
Medical Biller Salaries in 2026:
| Experience Level | Annual Salary Range |
|---|---|
| Entry-level (0–2 years) | $29,500 – $38,000 |
| Mid-level (3–7 years) | $42,000 – $55,000 |
| Senior / Revenue Cycle Manager | $55,000 – $75,000 |
| Remote biller (national average) | $40,000 – $58,000 |
Source: ZipRecruiter, Indeed, BLS
The salary verdict for medical billing vs medical coding:
Medical coders consistently earn somewhat more than medical billers at every experience level — primarily because coding requires more specialized clinical knowledge and the consequences of coding errors (claim denials, compliance violations, audit exposure) are more severe.
However, the most important salary factor in both roles is certification. According to AAPC data, certified coders earn 20.7% more than non-certified coders. A certified biller with 5 years of experience working in a high-volume practice or revenue cycle management company can match or exceed the salary of an uncertified coder.
Geography matters significantly too. California, New York, Massachusetts, and Washington pay 15–25% above the national average for both billing and coding roles. Washington D.C. ranks among the highest-paying markets, with average earnings of $62,810 per year for medical records specialists.
Remote work has become a major factor in 2026. Remote medical coding jobs offer salaries comparable to in-office positions — typically between $48,000 and $75,000 annually for experienced professionals. This flexibility has made both billing and coding increasingly attractive careers for people who want to work in healthcare without clinical patient contact.
Difference #6: Where Each Role Fits in the Revenue Cycle
Understanding medical billing vs medical coding means understanding where each step happens in the overall revenue cycle flow.
Here is how a single patient visit moves through the system:
Step 1 — Patient Visit The physician sees the patient, performs services, and documents everything in the medical record.
Step 2 — Medical Coding (Coder’s job) The coder reviews the documentation and assigns:
- ICD-10 codes for every diagnosis
- CPT codes for every procedure and service
- Modifiers where required
- HCPCS codes for supplies or drugs if applicable
The coded encounter is now ready for billing.
Step 3 — Charge Capture The coded charges are entered into the practice management system. In many practices, this step bridges coding and billing.
Step 4 — Claim Building (Biller’s job starts) The biller builds the claim using the codes, attaches patient and provider demographic information, verifies insurance eligibility, and checks for any payer-specific requirements.
Step 5 — Claim Scrubbing The claim goes through a scrubber — either manual review or automated — to catch errors before submission.
Step 6 — Claim Submission The biller submits the claim electronically through a clearinghouse to the payer.
Step 7 — Payment or Denial The payer processes the claim and either pays it, partially pays it, or denies it.
Step 8 — Denial Management / Appeals (Biller’s job continues) If denied, the biller identifies the reason, works with the coder to correct any coding issues if needed, and resubmits or appeals.
Step 9 — Payment Posting The biller posts the payment and reconciles the ERA against the original claim.
Step 10 — Patient Billing Any remaining patient responsibility is billed directly to the patient.
This sequence makes one thing very clear: coding happens first, and billing depends on coding being right. A coding error that makes it past the coder creates a problem the biller has to fix — often weeks later, after a denial. This is why the relationship between billing and coding teams matters so much in a healthy revenue cycle.
Difference #7: Compliance Risk and Audit Exposure
This is the difference between medical billing vs medical coding that most guides skip over — and it is arguably the most important one for practice owners to understand.
Coding compliance risk:
Every code a coder assigns creates a documented record that can be audited. The Office of Inspector General (OIG) conducts work plans annually that identify high-risk billing patterns, and Recovery Audit Contractors (RAC) use data analytics to flag practices whose coding patterns deviate from specialty peers.
Coding errors that create compliance risk include:
- Upcoding — billing a higher-level service than what was documented
- Unbundling — billing separately for procedures that should be billed together
- Using unspecified ICD-10 codes when more specific codes are available
- Mismatching diagnosis and procedure codes
A coder who consistently makes these types of errors creates audit exposure for the entire practice — not just for the specific claims that are wrong.
Billing compliance risk:
Medical billers create compliance risk when they:
- Submit claims for services that were not documented
- Bill services under an incorrectly credentialed provider
- Fail to apply correct payer-specific rules and modifiers
- Miss timely filing deadlines and attempt to conceal this
- Bill patients incorrectly after insurance payment
Our MD Audit Shield program monitors billing patterns for both coding and billing compliance risk — flagging anomalies before they attract payer or CMS audit attention. Understanding medical billing vs medical coding compliance is essential for any practice that bills Medicare or Medicaid.
The CMS Medicare Physician Fee Schedule governs how codes translate to payment rates, and any systematic miscoding — even unintentional — can result in overpayment demands, fines, and exclusion from Medicare participation in the most serious cases.
When Are Medical Billing and Coding Combined Into One Role?
In the medical billing vs medical coding discussion, one practical reality must be addressed: many small and mid-sized practices combine both roles into a single position.
This is common in:
- Solo physician practices and small group practices (1–5 providers)
- Specialty practices with manageable patient volume
- Rural practices with limited staffing budget
- Mental health and behavioral health practices
A combined billing and coding specialist handles documentation review, code assignment, claim building, submission, follow-up, and denial management — all in one position. This works reasonably well when the practice has manageable volume and the specialist is well-trained and certified.
The risks of combining the roles:
- High cognitive load increases error rates over time
- When one person is out sick or on vacation, the entire revenue cycle stalls
- Specialization in complex coding (oncology, cardiology, orthopedics) requires deep focus that is hard to maintain alongside billing responsibilities
- The person’s strengths in one area (billing communication, for example) may create gaps in the other area (coding precision)
The benchmark question: if your practice has more than 3 providers or bills more than $50,000 per month in claims, separate coding and billing functions — either through dedicated staff or through a professional billing service — will almost certainly produce better financial results than a combined role.
Medical Billing vs Medical Coding: Which Does Your Practice Actually Need?
Here is the practical question every practice owner or manager is really asking when they research medical billing vs medical coding.
The answer depends on where your revenue cycle pain is coming from:
You need better coding if:
- Your first-pass claim acceptance rate is below 90%
- You are receiving frequent medical necessity denials
- You have been flagged by a payer for unusual billing patterns
- Your coders are not certified or have not completed recent training
- You are billing complex specialties (oncology, cardiology, mental health) with generic coding knowledge
You need better billing if:
- Your days in accounts receivable consistently exceed 45 days
- Your denial rate is above 5%
- Denied claims are not being appealed systematically
- You have unworked claims sitting in your A/R beyond 90 days
- Patient collections are lagging behind insurance collections
You need both if:
- Your overall net collection rate is below 95%
- You have experienced a billing audit or received a RAC demand letter
- Your practice is growing and current processes cannot scale
- You are bringing on new providers and need credentialing plus billing setup
Our medical billing and practice management service handles both the coding and billing sides of the revenue cycle — so the sequencing, quality control, and follow-up happen as a connected system rather than two separate functions that have to be coordinated manually.
And our CodeMAXX coding service specifically handles the coding accuracy side — applying AI-assisted code validation to every claim before it reaches the billing stage, so errors do not travel downstream into denials.
Medical Billing vs Medical Coding — The Full Comparison Table
| Feature | Medical Coding | Medical Billing |
|---|---|---|
| Primary focus | Clinical documentation → codes | Codes → payment from insurance |
| Code systems used | ICD-10, CPT, HCPCS | CMS-1500, UB-04 claim forms |
| Talks to insurance companies? | Rarely | Daily |
| Talks to patients? | Rarely | Frequently |
| Primary certification | CPC (AAPC), CCS (AHIMA) | CPB (AAPC), CBCS (NHA) |
| Average 2026 salary (mid-level) | $50,000 – $62,000 | $42,000 – $55,000 |
| Where in revenue cycle? | Step 2 — after clinical visit | Steps 4–10 — claim through payment |
| Primary skill | Clinical knowledge + precision | Financial knowledge + communication |
| Compliance risk | Upcoding, unbundling, specificity | Timely filing, credentialing, patient billing |
| Remote work availability | Very high | High |
| Entry requirements | Certificate + CPC preferred | Certificate + CPB preferred |
| Job growth outlook (BLS) | 9% through 2033 | 9% through 2033 |
The Medical Billing vs Medical Coding Workflow Checklist
If you are a practice manager evaluating your current billing and coding setup, use this checklist to find gaps:
Coding Side:
- All coders have current-year CPT and ICD-10 code books or encoder access
- Coders are certified (CPC, CCS, or equivalent)
- Annual training on CPT code updates completed (new year = new codes)
- Specific ICD-10 codes used — not defaulting to unspecified when specific is available
- Modifier usage reviewed and documented
- High-risk CPT codes audited quarterly for documentation support
Billing Side:
- Eligibility verified for every patient before every visit
- Behavioral health benefits verified separately where applicable
- Prior authorization status checked and tracked before every authorized service
- Claims submitted within 14 days of date of service
- Aged A/R reviewed weekly — any claim over 45 days flagged
- Denial rate tracked monthly — benchmark below 5%
- Every denial appealed within 30 days
- Provider credentialing current with all active payers
Combined:
- Coder and biller (or billing service) communicate directly when denials involve coding questions
- Medical necessity documentation standards reviewed with clinical staff
- HIPAA compliance training current for all billing and coding staff
- RAC audit risk monitored — unusual billing patterns investigated before they attract attention
How Pro Health Care Advisors Handles Both Sides
When practices come to us trying to figure out the medical billing vs medical coding question for their own operations, the answer is almost always: you need both working together — not one or the other managed separately.
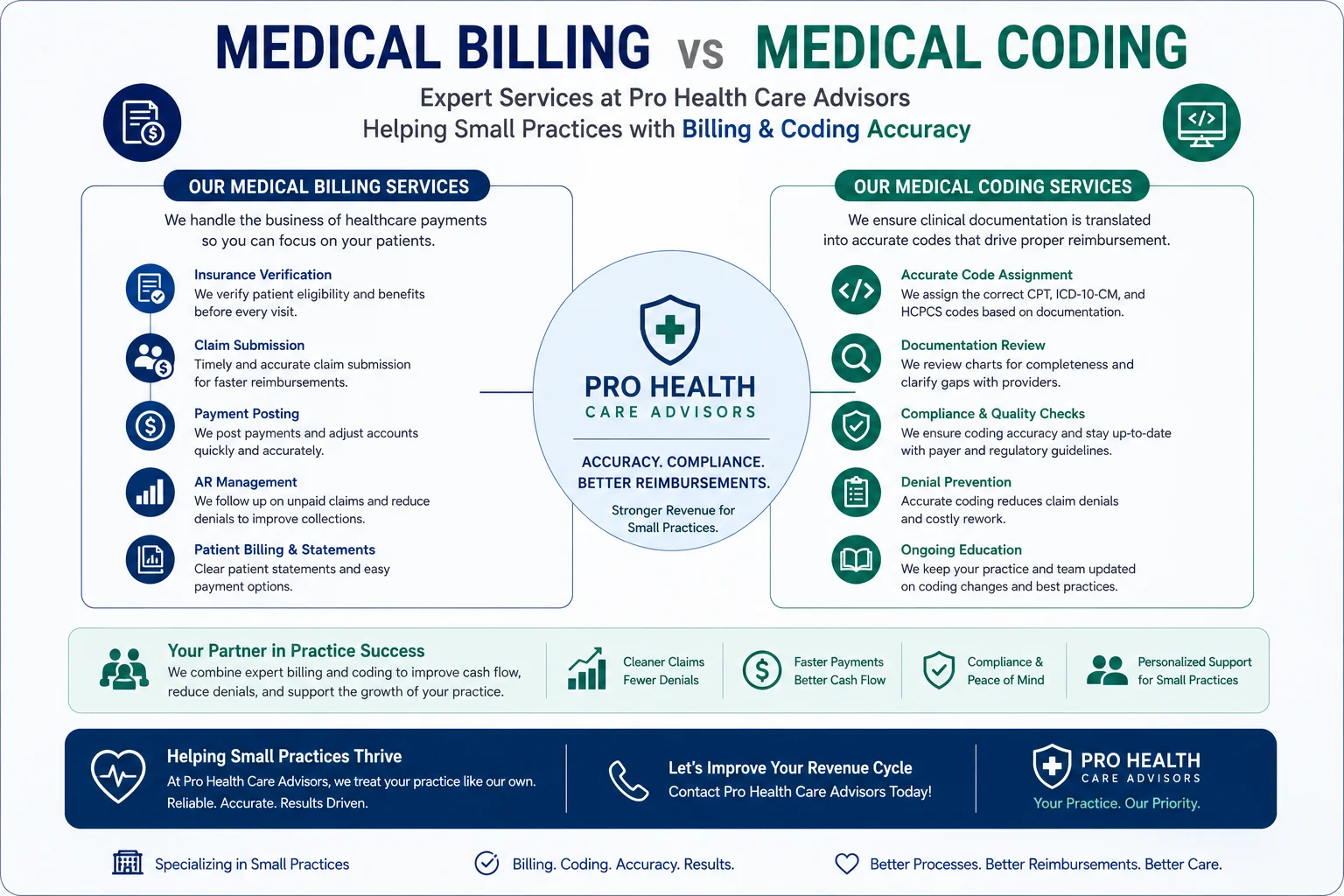
At Pro Health Care Advisors, our integrated service handles the entire revenue cycle as a connected system:
Coding accuracy through CodeMAXX: Our CodeMAXX medical coding service reviews clinical documentation, assigns accurate ICD-10 and CPT codes, applies the correct modifiers, and validates every code combination before it moves to the billing stage. This is where medical billing vs medical coding integration matters most — a coding error caught before submission costs zero. The same error caught after denial costs staff time, patient delays, and sometimes the claim itself.
Clean claim billing: Our medical billing team takes those coded claims, verifies eligibility, builds and scrubs the claim, submits to the correct payer, follows up systematically, and manages the denial and appeals process.
Credentialing to protect both: No coding or billing works if the provider is not properly credentialed with the payer. Our physician credentialing service ensures every provider’s enrollment is current, every recredentialing deadline is tracked, and no claim goes out under a lapsed or pending enrollment.
Audit protection across both: Our MD Audit Shield program monitors patterns across both coding and billing to identify audit risk before it becomes an audit.
The result is a revenue cycle where the coding side and the billing side speak the same language, share the same quality standards, and produce clean claims on first submission — rather than learning about problems through denials.
Contact our team for a free billing and coding review. We will show you exactly where your current process has gaps — and what it would take to close them.
Frequently Asked Questions: Medical Billing vs Medical Coding
Q: Is medical billing or medical coding harder to learn?
A: They are hard in different ways. Medical coding requires more clinical knowledge — you need to understand anatomy, physiology, medical terminology, and the clinical reasoning behind diagnoses and procedures. Medical billing requires more administrative and financial knowledge — insurance structures, claim submission rules, denial management, and patient communication. Most people find that whichever they learned first feels more natural, and the other requires genuine additional study.
Q: Can one person do both medical billing and medical coding?
A: Yes — and in small practices, this is common. A combined billing and coding specialist handles both functions. The risk is that high volume or complex specialties stretch one person’s expertise thin. Practices billing more than $50,000 per month or serving complex specialties generally see better results with separated functions — either through dedicated staff or a billing service that handles both.
Q: Which pays more — medical billing vs medical coding?
A: Medical coders consistently earn slightly more on average. The 2026 BLS median for medical records specialists is $50,250 per year. Medical coders with specialty certifications (CRC, oncology, cardiology coding) can earn $65,000–$85,000. Experienced senior billers and revenue cycle managers can reach $55,000–$75,000. Certification in either field significantly increases earnings — AAPC reports certified coders earn 20.7% more than non-certified peers.
Q: What is the job outlook for medical billing vs medical coding in 2026?
A: Both fields are growing. The Bureau of Labor Statistics projects 9% employment growth for medical records specialists from 2023 to 2033 — faster than the average for all occupations. Remote work has expanded significantly in both fields. Many large health systems, insurance companies, and billing services now hire fully remote coders and billers, making geographic location less of a limiting factor than it was five years ago.
Q: Does a medical practice need to hire a coder AND a biller separately?
A: Not necessarily — especially for small practices. Many small practices outsource both functions to a professional billing service rather than hiring in-house staff for either role. In-house billing requires salaries between $55,000 and $75,000 plus 20–30% in benefits and payroll taxes, plus management overhead. Outsourced billing typically costs 5–8% of collections — often significantly less in total, with better performance and no HR complexity.
Q: How does medical coding affect RAC audits?
A: Directly and significantly. Recovery Audit Contractors use data analytics to compare a practice’s coding patterns against specialty peers. Practices that consistently upcode, use unspecified diagnosis codes, or bill code combinations that do not clinically make sense attract audit attention. The coder’s accuracy is the first line of defense against audit risk — but the biller’s pattern of submission (how often certain codes are used, at what frequency, with what modifiers) is what the auditor actually sees. Both sides of medical billing vs medical coding contribute to audit risk. Our MD Audit Shield service monitors both.
Q: What is the difference between ICD-10 and CPT codes in medical billing vs medical coding?
A: ICD-10-CM codes describe diagnoses — what condition the patient has, what symptom brought them in, what disease is being treated. CPT codes describe procedures — what the provider did during the visit. In the medical billing vs medical coding workflow, coders assign both ICD-10 and CPT codes. Billers use those codes to build the claim. The payer uses the combination to determine whether the service was medically necessary and how much to pay.
Q: Can I learn medical billing and coding online?
A: Yes — and this has become one of the most common paths into both fields. Online certificate programs in medical billing and coding typically take 6 months to 2 years to complete. Many include preparation for the CPC, CBCS, or CCA certification exams. The AAPC and AHIMA both offer online resources and exam preparation. Certification significantly increases both employability and starting salary in both billing and coding roles.