Top 10 Costly Medical Claim Denial Reasons & Proven Fixes in 2026
Here is a number that should stop every practice manager cold.
$262 billion.
That is how much US healthcare organizations lose every single year because of revenue cycle inefficiencies — with medical claim denial reasons sitting at the very top of that list. And the problem is getting worse, not better. According to data from the Healthcare Financial Management Association (HFMA), initial denial rates climbed to nearly 12% in 2024 — up from around 10% just three years earlier.
What makes this genuinely painful is the part that comes next: up to 65% of denied claims are never reworked at all. That money does not get recovered. It just disappears from your revenue cycle permanently, claim by claim, month after month.
But here is what most of those statistics do not tell you — and what our billing team sees every single day working with small and individual practices across the country:
The overwhelming majority of medical claim denial reasons are preventable.
Not some. Not most. The overwhelming majority.
The top medical claim denial reasons in 2026 are not mysterious. They are not the result of complex insurance conspiracy. They are predictable, patterned, and — with the right processes in place — stoppable before a single incorrect claim ever leaves your practice.
This guide walks through every one of the top 10 medical claim denial reasons in detail. For each one, we explain exactly what triggers it, how to recognize it when it hits your practice, and the specific fix that stops it from happening again.
The State of Medical Claim Denials in 2026 — Why This Matters Right Now
Before we get into the specific medical claim denial reasons, it helps to understand the environment your practice is operating in right now.
In 2024, initial denial rates increased to 11.81% across commercial payers. Approximately 38–41% of providers now report denial rates at or above 10%.
Nearly one in five in-network claims — 19.1% — were still denied across ACA Marketplace insurers in 2024, leaving millions of Americans with unpaid medical bills despite having coverage.
Commercial plan denials rose 1.5% from 2023 to 2024, while Medicare Advantage denials spiked 4.8% in the same period — a meaningful signal given how aggressively Medicare Advantage has expanded its share of US beneficiaries.
These are not abstract industry statistics. For a practice billing $150,000 per month with a 12% denial rate, that is $18,000 per month in claims that do not pay on first submission. Some of that comes back after appeals. A significant portion of it never does.
The medical claim denial reasons driving these numbers have not changed dramatically — but payers in 2026 are catching them faster, using AI-powered claim review systems that flag issues in seconds that used to take human reviewers days. Payers are increasingly using AI-driven tools to flag discrepancies at a scale and speed human reviewers never could — and the trend is accelerating in 2026.
Which means the margin for error in your billing process is shrinking. And the practices winning on revenue cycle performance are the ones who have closed these gaps proactively — not reactively.
Let us go through each one.
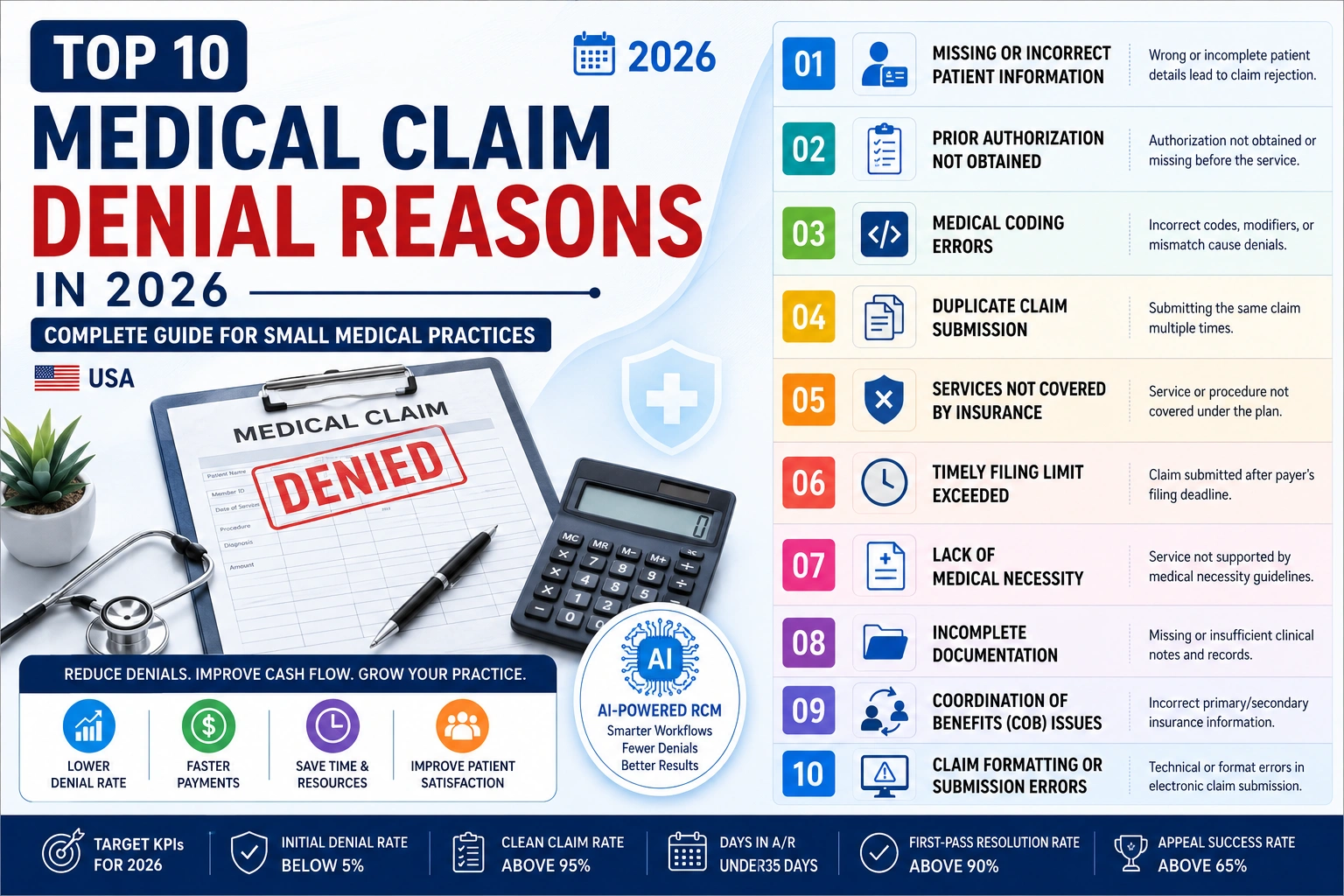
The Top 10 Medical Claim Denial Reasons in 2026 — And How to Fix Every One
Denial Reason #1: Incorrect or Incomplete Patient Information
How common: According to Experian Health’s State of Claims research, 26% of providers say that inaccurate or incomplete data collected at patient intake directly causes 10% or more of their denials. Patient information errors are among the top three medical claim denial reasons year after year.
What triggers it: A misspelled name. A wrong date of birth. An outdated address. The wrong insurance ID number copied from a card that the patient brought in two years ago. A gender marker that does not match what is on file with the payer. Any mismatch between what your practice submits and what the payer has in their system triggers an automatic rejection — not because the care was wrong, not because the coding was wrong, but because the demographic data did not match.
Real-world example: A patient whose legal name is “Kathryn” is registered as “Katherine” in your system. The claim goes out. The payer’s system does not recognize the name combination and rejects it automatically. The claim comes back six weeks later with a generic rejection code that takes your staff another hour to decode.
The proven fix:
- Verify patient name, date of birth, and insurance ID against the payer’s eligibility system — not just against what the patient writes on the form
- Scan both sides of the insurance card at every single visit, not just at new patient registration
- Run eligibility verification the day before each appointment so any issues surface before the patient arrives
- Update demographic information in your system immediately whenever a patient reports a change
This is one of the most preventable of all medical claim denial reasons, and it is still responsible for a significant share of rejections in practices that do not have a formal verification protocol.
Denial Reason #2: Insurance Eligibility Issues — Coverage That Is Not Active
How common: Eligibility problems are consistently in the top three medical claim denial reasons. A patient who had coverage last month may not have it this month — and the claim you submit will be denied as if they never had insurance at all.
What triggers it: Patient changed employers and their coverage lapsed during the transition. Patient’s premium payment was missed and coverage was terminated. Patient enrolled in a new plan but has not yet received their new card. Dependent coverage ended when the patient turned 26. The patient’s plan year reset and they are now in a different tier or deductible structure.
The specific 2026 wrinkle: Mental health and behavioral health benefits are frequently carved out to separate administrators — Optum, Beacon Health Options, Magellan Health. The medical coverage card in your system is correct, but the mental health payer is completely different. Billing mental health services to the medical payer is one of the most common hidden eligibility errors generating medical claim denial reasons in behavioral health practices right now.
The proven fix:
- Verify eligibility electronically for every patient, every visit — not just new patients
- Specifically verify behavioral health benefits separately from medical benefits for any mental health or counseling services
- For Medicare Advantage patients, verify coverage with the specific MA plan — not just Medicare generally
- When a patient reports a new insurance card, reverify from scratch rather than just updating the ID number
Working with a professional medical billing and practice management team that runs automated eligibility verification is the most effective way to eliminate this category of medical claim denial reasons entirely.
Denial Reason #3: Incorrect CPT or ICD-10 Coding Errors
How common: Incorrect or imprecise coding remains one of the top medical billing denial drivers in 2026. This includes missing modifiers, non-specific ICD-10 diagnosis codes, procedure-diagnosis mismatches, and evaluation and management level selections that do not align with documented medical decision-making complexity.
What triggers it: The wrong CPT code for the service actually performed. A diagnosis code (ICD-10) that does not support medical necessity for the procedure billed. A missing modifier that the payer requires. An E/M level (like 99214) that is not supported by the documented complexity of the visit. A code that is bundled with another code and cannot be billed separately without a modifier.
The American Medical Association releases CPT code updates every January — and in 2026, these updates include changes that affect billing across multiple specialties. Coding from last year’s superbill using this year’s patient encounters is a silent but steady source of denials.
The proven fix:
- Update all superbills and charge capture tools with current year CPT codes every January — before seeing a single patient in the new year
- Use the most specific ICD-10 code available for every diagnosis — unspecified codes get flagged more often than specific ones
- Train clinical staff annually on documentation requirements for common visit types — if the documentation does not support the code selected, change the documentation process, not the code
- Use claim scrubbing tools that catch code combinations that will be denied before submission
Our CodeMAXX medical coding service applies code validation to every claim before submission — catching these medical claim denial reasons before they ever reach a payer.
Denial Reason #4: Prior Authorization Not Obtained or Expired
How common: Missing or failed prior authorization is consistently one of the top five medical claim denial reasons. Some services require prior approval; therefore, not having the appropriate authorization will trigger a denial.
What triggers it: A service was performed without first obtaining required prior authorization from the payer. The authorization was obtained but expired before the service was rendered. The service performed does not match what was authorized. The authorization was for a different level of care than what was billed. The authorization was for a different facility or provider than where the service was delivered.
The 2026 reality: Prior authorization requirements have expanded significantly across commercial payers and Medicare Advantage plans over the past three years. Services that did not require authorization two years ago may require it now. This is especially true for behavioral health, high-cost imaging, specialty drugs, and elective surgical procedures.
The proven fix:
- Check authorization requirements every time a new procedure or service type is scheduled — payer requirements change regularly
- Track authorization approval dates and expiration dates in your scheduling system and flag appointments within 5 days of expiration
- Verify that the authorized service, provider, and facility all match exactly what will appear on the claim
- When authorization is denied on the clinical side, appeal immediately — do not assume the first denial is final
Prior authorization management is one of the most time-consuming billing tasks in a small practice. A dedicated billing service that manages authorization tracking removes this category of medical claim denial reasons from your staff’s plate entirely.
Denial Reason #5: Duplicate Claim Submission
How common: Duplicate claims are among the most avoidable medical claim denial reasons — and they happen more often than most practices realize, usually due to system glitches, manual resubmission errors, or billing staff who were not sure whether an original claim went through.
What triggers it: The same claim submitted twice with identical patient, date of service, provider, and procedure information. A claim resubmitted manually when the original was still processing. An EHR system that auto-resubmits on a schedule, sending a claim again before the first submission has resolved. A billing staff member who resubmits a claim thinking it was never sent, when it was sent and is pending.
The financial impact: Duplicate claims do not just get denied — they can trigger fraud alerts with certain payers if the pattern is consistent, which can escalate beyond a simple denial into a billing review.
The proven fix:
- Never resubmit a claim manually without first confirming in your clearinghouse or payer portal that the original is not pending
- Set up your practice management system to flag claims that have already been submitted before allowing resubmission
- Conduct monthly audits of denied claims to identify any duplicate patterns
- Train billing staff: “check before you resubmit” should be a standing rule
Denial Reason #6: Service Not Covered by the Patient’s Plan
How common: Non-covered service denials are a consistent source of medical claim denial reasons — and they are particularly frustrating because the clinical care was often completely appropriate. The problem is not what was done; it is whether the patient’s specific plan covers it.
What triggers it: A procedure that Medicare covers but the patient’s Medicare Advantage plan excludes. A mental health service that is covered under parity rules but the specific plan has carved it out or applies different criteria. A service that requires a specific diagnosis code to be covered but the diagnosis in the chart does not match the plan’s coverage criteria. A cosmetic or investigational procedure that is not covered under any circumstances.
The 2026 context: One of the most important things experienced denial specialists know is that the reason code on a denial EOB is frequently not the actual cause of the denial. Payers routinely return generic codes — “not medically necessary,” “insufficient documentation,” “non-covered service” — that obscure what actually triggered the rejection.
This means a denial coded as “non-covered service” may actually be a coding error, a medical necessity documentation gap, or a plan-specific exclusion — and understanding which one requires looking beyond the denial code itself.
The proven fix:
- For any high-cost or unusual procedure, verify coverage with the specific plan before scheduling — not just with the general payer
- Obtain Advance Beneficiary Notices (ABNs) for Medicare patients when you believe a service may not be covered — this protects you and gives the patient informed consent about their financial responsibility
- Document medical necessity explicitly and completely in the chart for every service that could be questioned
- When a service is denied as non-covered, research the actual coverage criteria before deciding whether to appeal or write off
Denial Reason #7: Missing or Incomplete Documentation
How common: Documentation issues are among the most cited medical claim denial reasons across all payer types. According to the Experian State of Claims survey, the top three reasons for denials are missing or inaccurate data, authorization issues, and inaccurate or incomplete patient information.
What triggers it: A claim is submitted without the supporting documentation the payer requires. The Additional Documentation Request (ADR) that arrived three weeks ago was not responded to within the deadline. A mental health claim was submitted without start and stop times documented. A home health claim went out without the required physician certification. A durable medical equipment claim was submitted without the detailed written order.
The specific documentation gaps that trigger medical claim denial reasons most often in 2026:
- Mental health: missing start/stop times for time-based psychotherapy codes
- Surgery: missing operative notes, missing pre-authorization documentation
- Home health: missing certificate of medical necessity from the ordering physician
- Physical therapy: missing functional assessment scores, missing plan of care signature
- All claims: missing physician signature or unsigned encounter notes
The proven fix:
- For every service type you bill regularly, create a documentation checklist that must be completed before the claim is submitted
- Respond to every Additional Documentation Request (ADR) within 10 business days — the 45-day deadline is not forgiving
- Set up a claims tracking system that flags any claim pending a documentation response
- Conduct quarterly internal audits of your documentation against payer requirements for your top five service types
If your practice receives a significant number of ADRs, it is worth reviewing whether there is a systemic documentation gap — or whether a pattern in your billing is attracting payer attention that our MD Audit Shield program can help you assess and address before it escalates.
Denial Reason #8: Provider Not Credentialed or Out of Network
How common: Credentialing-related medical claim denial reasons are among the most costly because they are often not caught until weeks of claims have accumulated under an unenrolled or lapsed provider.
What triggers it: A new provider starts seeing patients before their insurance credentialing is complete. An existing provider’s credentialing lapses at a payer because the recredentialing deadline was missed. A provider renders services at a facility where they are not privileged. A provider delivers services before their effective date of participation, even by a single day.
Provider credentialing operates invisibly when it is current — and catastrophically when it lapses. A single expired credentialing status with one payer means every claim submitted under that provider’s NPI for that payer will be denied. Those denials can accumulate for weeks before anyone identifies the root cause.
The 2026 update: NCQA now requires healthcare organizations to verify provider credentials on a monthly basis — a shift from the previous 6-month cycle. This means credentialing lapses that might have gone undetected for months in the past can now be caught faster by payers.
The proven fix:
- Begin credentialing for any new provider at least 120 days before their intended start date — not 60 days, not 30 days
- Create a credentialing expiration calendar with automated alerts at 180, 90, and 60 days before each recredentialing deadline
- Never allow a new provider to bill insurance until you have received written confirmation of their effective date from each payer
- Work with a dedicated physician credentialing service that tracks all expiration dates and initiates renewals proactively
Denial Reason #9: Timely Filing Deadline Missed
How common: Timely filing denials are among the most permanent medical claim denial reasons — because once the filing window closes, there is typically no path to appeal, no reconsideration, and no recovery. The revenue is simply gone.
What triggers it: A claim that was submitted after the payer’s timely filing deadline. Medicare requires claims within 12 months of the date of service. Most commercial payers require submission within 90 to 180 days. Some payers have windows as short as 60 days. A claim that sat in a queue, got lost in a system transition, or was set aside pending documentation — and was never followed up — can silently cross the deadline.
The numbers that put this in perspective: Accounts receivable does not age gracefully in US healthcare. Claims that remain unresolved beyond 90 days become progressively harder to collect. Beyond 120 days, payer contract terms and CMS regulatory provisions increasingly favor the payer. Beyond 180 days, most of that revenue is effectively gone.
The proven fix:
- Submit all claims within 30 days of the date of service — ideally within 14 days
- Set up your billing system to alert you when any claim approaches 60 days without resolution
- Conduct a weekly aged accounts receivable review — any claim over 45 days should be actively investigated, not just sitting in a queue
- Know the timely filing deadline for every payer in your mix — and document these in a payer reference sheet that your billing team can access quickly
Denial Reason #10: Coordination of Benefits (COB) Errors
How common: COB errors are a frequently misunderstood category of medical claim denial reasons that trip up practices handling patients with dual coverage — Medicare plus a supplemental plan, two commercial plans from different employers, or Medicare with Medicaid.
What triggers it: A claim is submitted to the secondary payer before the primary payer has processed it. The primary and secondary payer designations on the claim are reversed. A patient failed to update their coordination of benefits information with Medicare when they acquired other coverage. A patient who is covered by both their own employer plan and their spouse’s employer plan — and neither your registration staff nor the patient is certain which one is primary.
The specific COB rule that trips up practices most often in 2026: When a patient has Medicare and is still actively working at a company with 20 or more employees, the employer plan is primary and Medicare is secondary — not the other way around. Billing Medicare first in this situation results in automatic denial, and the practice then has to reprocess through the employer plan, which may have its own timely filing window already closing.
The proven fix:
- At every new patient intake and every insurance update, ask explicitly: “Do you have any other health insurance coverage?” — not just “Is this your only insurance?”
- Verify COB status with Medicare for any patient who also has employer coverage
- When processing secondary claims, always include the primary payer’s EOB with the submission
- Set up your billing system to flag any account with multiple active insurances for COB review before claim submission
Medical Claim Denial Reasons by the Numbers — 2026 Snapshot
| Denial Category | Share of Total Denials | Preventable? |
|---|---|---|
| Patient information / eligibility errors | ~26% | ✅ Fully preventable |
| Prior authorization issues | ~18% | ✅ Fully preventable |
| Coding errors (CPT/ICD-10) | ~16% | ✅ Fully preventable |
| Missing documentation | ~14% | ✅ Largely preventable |
| Non-covered services | ~10% | ✅ Largely preventable |
| Duplicate claims | ~6% | ✅ Fully preventable |
| Credentialing / network issues | ~5% | ✅ Fully preventable |
| Timely filing missed | ~3% | ✅ Fully preventable |
| COB errors | ~2% | ✅ Largely preventable |
The math that matters: If 90% of medical claim denial reasons are preventable, and your practice has a 12% denial rate, a comprehensive denial prevention program could realistically bring that rate to 2–3%. On $150,000 in monthly claims, that is the difference between $18,000 in denied claims per month and $3,000–$4,500. The difference is recoverable revenue.
Your Medical Claim Denial Prevention Checklist — Print and Use Daily
Before Every Patient Visit:
- Eligibility verified electronically — specific to the services being rendered
- Behavioral health benefits verified separately if applicable
- Prior authorization confirmed and within approved service limits
- COB status confirmed for any patient with multiple coverages
- Provider credentialing active with all payers being billed
Before Submitting Every Claim:
- Patient demographics match payer records exactly
- CPT codes current — from current year code set
- ICD-10 codes specific — not unspecified when a more specific code is available
- Diagnosis supports medical necessity for every procedure billed
- All required modifiers present
- No duplicate claim already pending for this date of service
- Authorization number on claim if service required prior auth
- Documentation complete and signed before claim submission
- Claim submission within 14 days of date of service (never exceed 30 days)
Weekly Billing Review:
- Review denial report — identify patterns, not just individual denials
- Pull aged AR report — flag any claim over 45 days for active follow-up
- Check timely filing deadlines — any claims approaching 60 days need immediate action
- Appeal any denied claims within 30 days of denial date

How Pro Health Care Advisors Stops Medical Claim Denial Reasons Before They Start
Understanding medical claim denial reasons is one thing. Having the systems, staff, and expertise to prevent them consistently — across hundreds or thousands of claims per month — is another.
At Pro Health Care Advisors, our medical billing and RCM service is built specifically around preventing the medical claim denial reasons that cost small practices the most revenue. Here is exactly how we do it:
Front-End Eligibility Verification We verify insurance coverage electronically before every appointment — including behavioral health carve-outs, coordination of benefits, and prior authorization requirements. Eligibility surprises do not reach the claim stage.
Accurate Coding Through CodeMAXX Our CodeMAXX coding service validates every CPT and ICD-10 code combination before submission — catching mismatches, missing modifiers, and bundling errors that generate medical claim denial reasons when they reach payer claim systems.
Prior Authorization Tracking We track authorization approvals, session limits, and expiration dates across every payer in your mix. Renewals are initiated proactively before claims get denied for expired authorizations.
Credentialing Management Our physician credentialing service tracks every provider’s credentialing status and recredentialing deadlines — ensuring no claim is ever submitted under a lapsed or pending enrollment.
HIPAA-Compliant Documentation Standards Working within HIPAA compliance guidelines, we help practices maintain documentation standards that satisfy payer requirements — reducing medical claim denial reasons related to insufficient documentation.
RAC Audit Monitoring Through our MD Audit Shield program, we monitor your billing patterns for anomalies that attract payer or CMS auditor attention — protecting your practice from escalating beyond individual denials into formal audit proceedings.
Denial Appeals Management When a claim is denied despite our prevention efforts, we build the appeal with the specific documentation and regulatory arguments each denial requires — and we track appeals through every level until the claim is resolved.
Contact our team today for a free billing review. We will identify which medical claim denial reasons are costing your practice the most, and show you exactly what it would take to fix them.
Frequently Asked Questions About Medical Claim Denial Reasons
Q: What is the most common medical claim denial reason in 2026?
A: Patient information and eligibility errors consistently rank as the leading medical claim denial reason across all payer types. Experian Health reports that 26% of providers say inaccurate data at patient intake directly causes 10% or more of their denials. The fix is straightforward: verify eligibility electronically before every appointment, not just at initial registration.
Q: How long do I have to appeal a denied medical claim?
A: Appeal timelines vary by payer. Medicare requires appeals — called redeterminations — within 120 days of the denial date. Most commercial payers allow 30 to 180 days to appeal, with 60 days being the most common standard. Medicaid timelines vary by state. The practical rule: never let a denial sit for more than 30 days without action. The sooner you appeal, the more context you have about why the denial happened and what documentation to include.
Q: Can I bill the patient when a claim is denied?
A: It depends on the denial reason and your contract. For participating providers, balance billing patients for services covered under the plan contract is generally not permitted when a denial is a billing error on your side. If a service is genuinely non-covered and you obtained a signed ABN (Advance Beneficiary Notice) in advance, you may bill the patient. If a claim is denied for prior authorization failure, billing the patient depends on whether they were informed in advance that the service might not be covered. Consult your payer contracts and, when in doubt, consult a healthcare billing attorney before billing patients for denied claims.
Q: What percentage of denied claims can actually be recovered through appeal?
A: It depends significantly on the denial reason. Studies show that of denied Medicare Advantage claims, 57% were ultimately overturned on appeal. For commercial payer denials where the reason is administrative — wrong eligibility, missing modifier, expired authorization — recovery rates through corrected claim resubmission are often 80% or higher. For denials based on medical necessity determinations, recovery depends heavily on the quality of the clinical documentation in the appeal. The key is appealing quickly, appealing with complete documentation, and understanding which denial reasons are genuinely winnable versus which ones are better written off and prevented going forward.
Q: How do I know if my denial rate is too high?
A: The benchmark for a healthy first-pass claim acceptance rate is 95% or higher — meaning your denial rate should be 5% or below. Approximately 38–41% of providers now experience denial rates of 10% or higher. If your denial rate is consistently above 5%, it is worth doing a root-cause analysis on your top denial reasons. Most practices find that 2–3 specific medical claim denial reasons account for the majority of their denials — and fixing those root causes moves the needle significantly.
Q: Does having a professional billing service really reduce medical claim denial reasons?
A: The data says yes — consistently. Practices that work with professional billing services that have systematic verification, coding validation, and authorization tracking processes see meaningfully lower denial rates than those managing billing in-house without those systems. The key difference is prevention: a professional billing team catches medical claim denial reasons before claims go out, rather than chasing them after denials arrive. Contact us for a free billing review that shows you exactly where your denial patterns are concentrated.
Q: What happens if I miss a timely filing deadline?
A: Once a timely filing deadline passes, the claim is typically not recoverable through standard appeals. Some payers have a process for filing deadline exceptions in cases of documented system errors or other extraordinary circumstances — but this is not guaranteed. The practical answer: submit claims within 14 days of service, review aged AR weekly, and never let a claim go unaddressed past 45 days. Once revenue is past the timely filing window, it is gone. Prevention is the only strategy that works for this category of medical claim denial reasons.
Q: Are RAC audits related to medical claim denial reasons?
A: Yes, indirectly. Certain medical claim denial reasons — particularly coding errors, medical necessity documentation gaps, and overbilling patterns — are exactly what RAC auditors look for when selecting practices for review. A practice that consistently bills specific codes at rates higher than peers in their specialty, or that has documentation gaps across a large volume of claims, creates the kind of statistical anomaly that attracts audit attention. Our MD Audit Shield program monitors your billing patterns for these risk indicators and helps you address them before they escalate. You can also learn more about RAC audit protection strategies on our services page.