Value-Based Care Billing 2026 | How the Shift from Fee-for-Service Changes Your Revenue
The Rules of Getting Paid Just Changed
For decades, the formula was simple: see more patients, bill more services, collect more money. Volume was everything. The more procedures you performed, the more claims you submitted, the more revenue came through the door. Fee-for-service was not just a billing model — it was the engine that ran American medical practice.
That engine is not dead. But it is being replaced, piece by piece, with something fundamentally different.
In 2026, the Centers for Medicare and Medicaid Services (CMS) made a move that officially divided physicians into two financial classes — those participating in value-based care models and those who are not. For the first time in the history of the Medicare Physician Fee Schedule, there are now two separate conversion factors, and the gap between them is not symbolic. It is real money.
This article breaks down exactly what value-based care billing means in 2026, what changed in the CMS Physician Fee Schedule Final Rule, which codes and programs your practice needs to know about, and how to protect — and grow — your revenue in this new environment.
📌 Not sure whether your practice qualifies for Advanced APM participation? Our team at ProHealth Care Advisors can review your payer mix and help you identify the right pathway.
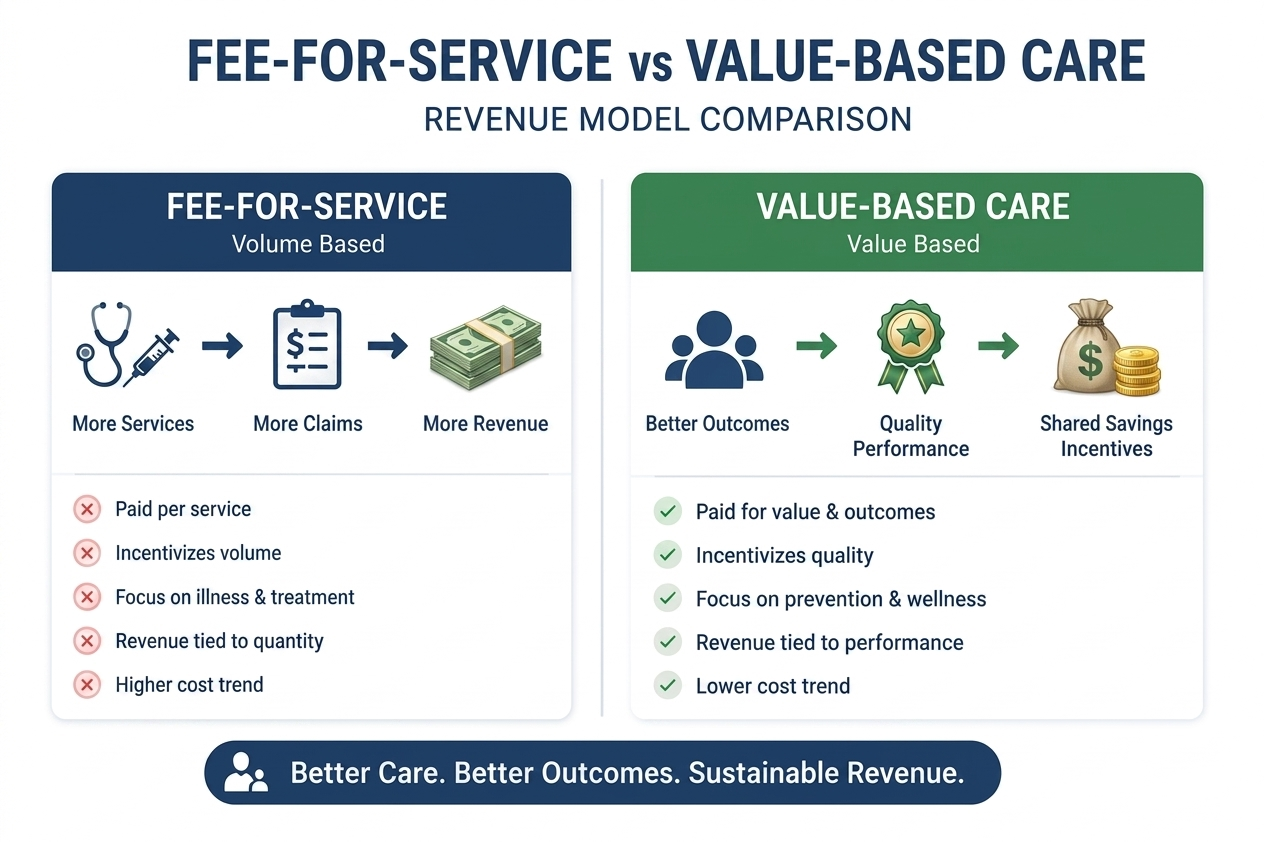
First, What Is Value-Based Care — In Plain English?
Think about two plumbers. The first one charges you by the hour. Whether the pipe gets fixed or not, you pay for their time. The second one charges you only when the leak is actually fixed — and charges you more if the repair holds longer than average.
Fee-for-service medicine works like the first plumber. You get paid for every service you deliver, regardless of whether the patient actually gets better.
Value-based care works like the second plumber. You get paid based on the outcomes your patients experience — their health, their hospital readmission rate, their adherence to treatment plans, and how efficiently you managed their care.
This is not a theoretical concept anymore. In 2026, it is how Medicare — the single largest payer in the United States — is structuring its physician payments. And commercial payers are following CMS’s lead faster than most practices realize.
The 2026 Split That Every Physician Needs to Understand
The single most important structural change in the 2026 CMS Physician Fee Schedule is something that sounds technical but has very direct financial consequences: the creation of two separate conversion factors.
A conversion factor is the dollar amount CMS multiplies by your Relative Value Units (RVUs) to calculate your Medicare payment. Every CPT code you bill has an RVU attached to it. The higher the conversion factor, the more you get paid for the same service.
Here is what the 2026 numbers look like:
| Physician Category | 2026 Conversion Factor | Change from 2025 |
|---|---|---|
| Qualifying APM Participants | $33.57 | +3.77% increase |
| Non-Qualifying APM Participants | $33.40 | +3.26% increase |
| Previous 2025 Rate (all physicians) | $32.35 | — |
At first glance, both numbers look like good news — and they are, relatively speaking. This is the first meaningful increase for physicians in several years, driven by provisions in the Medicare Access and CHIP Reauthorization Act (MACRA) and the One Big Beautiful Bill Act.
But here is what the raw numbers hide: the gap between qualifying and non-qualifying APM participants is growing, and practices outside value-based programs are accumulating a compounding disadvantage year after year.
According to one analysis of primary care practices billing $2–5 million annually, remaining in volume-based billing creates an immediate annual revenue disadvantage of $204,000–$306,000 compared to Advanced APM participation. Project that gap forward to 2030, and the accumulated shortfall climbs into seven figures.
What Is an APM and Do You Qualify?
APM stands for Alternative Payment Model. It is the umbrella term CMS uses for programs where physicians accept some accountability for quality and cost of care in exchange for different — typically better — payment terms.
There are two main tracks under the Quality Payment Program (QPP):
Track 1: MIPS (Merit-Based Incentive Payment System)
MIPS is the default value-based track for most physicians who bill Medicare Part B but are not in an Advanced APM. Under MIPS, your Medicare payments are adjusted based on your performance across four categories:
- Quality — clinical quality measures relevant to your specialty
- Cost — how efficiently you use Medicare resources
- Improvement Activities — things like care coordination, expanded patient access, or health equity work
- Promoting Interoperability — how well your practice uses certified EHR technology
For 2026 payment adjustments, CMS is using 2024 performance year data as the basis. The potential swing is ±9% on your Medicare payments — meaning a practice billing $300,000 in annual Medicare revenue could see a $27,000 difference in either direction based solely on MIPS performance.
Track 2: Advanced APMs (Better Rewards, More Risk)
Advanced APMs — including Medicare Shared Savings Program (MSSP) ACOs, ACO REACH, Making Care Primary, and Primary Care First — offer higher conversion factor rates in exchange for accepting financial risk tied to patient outcomes and total cost of care.
Qualifying APM Participants (QPs) receive the higher conversion factor of $33.57, are excluded from MIPS reporting requirements, and are eligible for shared savings if their patient population’s total cost of care comes in under benchmark.
The tradeoff is real accountability. In two-sided risk arrangements, practices can also face financial penalties if costs exceed targets. This is not the right model for every practice — but for well-organized primary care and multi-specialty groups, the upside potential is significant.
📌 Want to evaluate whether an ACO or Advanced APM makes sense for your practice? Start with a conversation with our billing specialists at ProHealth Care Advisors.
The APCM Codes: The Biggest Opportunity Most Primary Care Practices Are Missing
If you run a primary care practice in 2026 and you are not billing Advanced Primary Care Management (APCM) codes, you may be leaving thousands of dollars per month on the table.
APCM launched on January 1, 2025, and was significantly expanded in the 2026 Physician Fee Schedule. It is designed to replace the patchwork of Chronic Care Management (CCM), Principal Care Management (PCM), and Transitional Care Management (TCM) codes with a single, streamlined monthly payment structure built around relationship-based care rather than minute-counting.
The Three APCM Base Codes
CMS created three HCPCS base codes for APCM, stratified by patient complexity:
| Code | Patient Complexity | Description |
|---|---|---|
| G0556 | Low complexity | 1–2 chronic conditions, no Medicaid |
| G0557 | Moderate complexity | 3+ chronic conditions OR Medicaid eligible |
| G0558 | High complexity | Multiple complex conditions with high needs |
The 2026 Physician Fee Schedule delivered approximately 10% reimbursement increases across all three APCM codes compared to 2025 rates.
Three New Behavioral Health Add-On Codes (2026)
One of the most important expansions in the 2026 rule is the introduction of three brand-new HCPCS add-on codes that can be billed alongside APCM base codes for patients who also need behavioral health integration:
- G0568 — Initial month of Collaborative Care Model (CoCM) services for APCM patients
- G0569 — Subsequent months of CoCM services for APCM patients
- G0570 — Additional behavioral health integration time
This means practices can now layer behavioral health and collaborative care reimbursement on top of their APCM base payment for the same patient in the same month — something that was not possible before 2026.
What APCM Requires: The 13 Service Elements
APCM is not just a billing code. It requires completing a set of 13 defined service elements (when clinically appropriate), including:
- 24/7 patient access to care team for urgent needs
- Ongoing care management and coordination across providers
- Medication reconciliation and management
- Patient health goal assessment and monitoring
- Care plan documentation accessible to the patient
The key distinction from old CCM rules: you do not need to track time per month. The bundled payment covers the management work, as long as you document that the service elements are being addressed.

The G2211 Add-On Code: Still Underused, Still Valuable
Before we move on from primary care, let us address a code that was introduced in 2024 and remains chronically under-billed in 2026: G2211.
G2211 is an add-on code that can be billed alongside office visit E/M codes (99202–99215) when the physician is the patient’s ongoing, longitudinal care manager — meaning this is not a one-time visit but part of an established care relationship.
The reimbursement is modest per encounter (roughly $16–$17 in Medicare) but adds up significantly across a full patient panel. A primary care physician with 1,500 active Medicare patients could add tens of thousands of dollars per year by consistently capturing this add-on when it applies.
The reason it is underused: many physicians are either unaware of it, uncertain about the documentation required, or their EHR templates do not prompt for it at the point of care.
How the Shift Affects Different Specialties
Value-based billing is not a primary care issue alone. Every specialty is affected differently, and it is worth understanding where the pressure and opportunity lie.
Primary Care and Internal Medicine
This is where value-based care hits hardest — and where the reward for adapting is greatest. APCM, G2211, MIPS reporting, and ACO participation all live primarily in this space. Practices with a large Medicare panel that have not yet enrolled in MSSP or another qualifying APM should treat that as an urgent revenue decision, not a long-term planning item.
Behavioral Health
The 2026 rule significantly expands telehealth parity for behavioral health services and adds the new behavioral health APCM add-on codes. Psychiatrists, psychologists, and licensed clinical social workers who coordinate care with primary care practices now have new billing pathways through the Collaborative Care Model integration codes.
Additionally, MIPS applies to behavioral health providers who bill Medicare above the low-volume threshold, meaning performance scores and payment adjustments are very much in play.
Cardiology and Specialty Medicine
Specialists participate in value-based care primarily through MIPS and through episode-based payment models. Cardiologists with high volumes of Medicare patients face meaningful MIPS payment swings. The 2026 efficiency adjustment — which trims work RVU values for imaging and certain procedures — also reduces per-service payments in some procedure-heavy specialty practices. Coding accuracy and complete documentation become even more important when the per-unit reimbursement is being adjusted downward.
Surgery and Procedural Specialties
For surgeons, the most significant 2026 change is the efficiency adjustment on procedures that have seen significant increases in speed or technology assistance over time. Some surgical RVU values were reduced to reflect shorter actual procedure times. At the same time, new CPT codes — including the leg revascularization overhaul covered in our CPT Code Changes 2026 guide — mean that accurately coding new techniques now has proper billing pathways.
The Documentation Shift: From Volume Tracking to Outcome Tracking
This is where the practical day-to-day work changes for most clinical teams.
Under fee-for-service, documentation was largely about justifying the level of service billed — how many problems were addressed, how complex the medical decision-making was, how much time was spent. That work still matters. E/M documentation requirements have not disappeared.
But value-based billing adds a second layer of documentation purpose: tracking quality metrics, care gaps, and patient outcomes that feed into MIPS performance scores and APM reporting requirements.
In concrete terms, your documentation now needs to capture:
Quality measure numerators and denominators — For example, if you are reporting on diabetic HbA1c control, your notes need to clearly document the test result and whether the patient is in control. Many practices lose MIPS points not because they are not doing the care, but because the data is buried in a note rather than structured in a way the EHR can extract.
Care gap closure documentation — Screenings ordered, preventive services offered, and referrals completed need to be documented in a way that flags them as closed in your quality reporting system.
Social determinants of health (SDOH) — The 2026 rule revised HCPCS code G0136, previously used for SDOH screening, to now capture physical activity and nutrition assessments (effective January 1, 2026). This shift reflects CMS’s evolving focus on lifestyle-based prevention alongside social factors.
The bottom line: if your clinical documentation exists only to justify a billing level, you are leaving quality points — and therefore payment — on the table.
What Payers Beyond Medicare Are Doing
CMS sets the tone, but commercial payers are moving fast in the same direction.
In 2026, more commercial payer contracts now include quality metrics, patient outcome thresholds, and cost efficiency targets as conditions of full reimbursement. Many contracts that once paid simply on claims submission now include:
- Annual quality scorecards that affect contracted rates at renewal
- Shared savings arrangements for patient populations managed by the practice
- Pay-for-performance bonuses tied to HEDIS measures or custom quality metrics
- Risk-stratified panels where complex patients generate higher per-member-per-month payments
The practices that track their MIPS performance carefully are building the exact same muscle they need to succeed in commercial value-based contracts. The data infrastructure is the same. The documentation habits are the same. The mindset is the same.
Common Mistakes Practices Are Making Right Now
Even practices that understand value-based billing conceptually are making errors that cost them money.
Not tracking MIPS reporting deadlines. The 2026 payment adjustment is based on 2024 performance data. The 2027 payment adjustment will reflect 2025 data. If your practice submitted 2025 MIPS data late or incompletely, that shows up in your payment rate next year. Missing the submission window means a guaranteed negative adjustment.
Billing CCM codes when APCM is the better fit. Some practices that have been billing Chronic Care Management codes for years have not evaluated whether APCM — with its higher reimbursement and simpler time-tracking rules — would be a better fit for their care management workflows. This is worth a specific analysis by your billing team.
Assuming small practices are exempt from MIPS. Providers below the low-volume threshold (fewer than 200 covered professional services or less than $90,000 in Medicare Part B allowed charges) are exempt. But practices slightly above that threshold are often unaware of their MIPS obligations until denials or audits surface.
Not verifying APCM eligibility at the patient level. APCM requires that the billing provider is responsible for the patient’s primary care needs and is the continuing focal point for their healthcare services. Only one provider can bill APCM for a given patient per calendar month. Billing APCM for patients where care coordination responsibility is shared or unclear creates audit exposure.
Failing to document concurrent care restrictions. APCM cannot be billed in the same month as CCM, PCM, TCM, interprofessional internet consultation, remote evaluation of patient videos or images, virtual check-ins, or e-visits for the same patient. Duplicate billing creates denials and compliance risk.
A Practical Action Plan for 2026
If your practice has not started this transition, here is where to begin:
Step 1: Determine Your QPP Participation Status
Log into the CMS Quality Payment Program portal and confirm whether your practice qualifies as an Advanced APM participant or falls under MIPS. Your participation status determines which conversion factor applies to your 2026 Medicare payments.
Step 2: Pull Your MIPS Performance Score
If you are a MIPS participant, access your current performance score and identify which category is dragging your score down. Quality is typically the highest-weighted category and often where practices have the most room to improve.
Step 3: Evaluate APCM Eligibility
Run a report of your Medicare patients who have two or more chronic conditions. These are your APCM-eligible patients. Calculate the monthly revenue you could generate by billing APCM for this panel and compare it to your current CCM billing.
Step 4: Update Your EHR Templates
Work with your EHR vendor or practice administrator to build structured fields that capture quality measure data at the point of care — rather than requiring retrospective chart review to pull data for MIPS reporting.
Step 5: Consider ACO Enrollment for Next Year
If your practice has not explored Medicare Shared Savings Program participation, 2026 is the year to do the analysis. ACO enrollment timelines mean decisions made now affect 2027 participation. Organizations like the National Association of ACOs (NAACOS) offer resources to help independent practices evaluate the fit.
📌 Our team at ProHealth Care Advisors specializes in helping practices navigate the transition from fee-for-service to value-based billing — from MIPS optimization to APCM implementation. Reach out for a revenue impact assessment.
Official Resources to Bookmark
For practice-level decisions, always reference primary sources:
- CMS 2026 Physician Fee Schedule Final Rule — The authoritative CMS document covering all 2026 payment policies
- CMS Quality Payment Program Portal — Check your MIPS participation status and performance scores
- CMS Advanced Primary Care Management Services page — Official APCM billing requirements and service elements
- AMA Physician Fee Schedule Overview — AMA’s breakdown of fee schedule changes for physicians
- NAACOS — National Association of ACOs — For practices exploring ACO participation
The Bottom Line: Volume Still Matters, But Value Matters More
This shift does not mean you should see fewer patients or bill fewer services. Volume still matters. Efficiency still matters. But the practices that thrive in 2026 and beyond are the ones that understand a simple truth: payers — led by CMS — are increasingly willing to pay more for better outcomes, and less for pure volume without accountability.
The good news is that most primary care practices are already doing the work. They are managing chronic conditions. They are coordinating care. They are keeping patients out of the hospital. The gap is not between what good practices do and what value-based care requires. The gap is between what those practices do and what they actually document and bill for.
Closing that gap is not about gaming the system. It is about getting credit — and payment — for care you are already delivering.
Frequently Asked Questions
Q: What is the difference between MIPS and an Advanced APM in 2026?
A: MIPS is the default value-based track for most Medicare-billing physicians. It applies a payment adjustment (positive or negative) based on annual performance scores. Advanced APMs — like MSSP ACOs — offer a higher conversion factor and exempt you from MIPS in exchange for accepting financial accountability for quality and cost outcomes.
Q: Can I bill APCM codes and still use fee-for-service billing for office visits?
A: Yes. APCM is a monthly care management payment. It does not replace your office visit E/M billing. You can bill your standard 99202–99215 codes for face-to-face visits while also billing APCM for the ongoing care management work that happens between visits.
Q: How do I know if my practice is above the MIPS low-volume threshold?
A: CMS excludes providers below $90,000 in Part B allowed charges OR fewer than 200 covered professional services per year. You can check your status at the QPP portal.
Q: What happens to my Medicare payments if I ignore MIPS?
A: Ignoring MIPS (failing to submit any data) results in the maximum negative payment adjustment — currently -9% on your Medicare Part B payments for that year.
Q: Are commercial payers moving toward value-based models too?
A: Yes. Most major commercial payers now include some form of quality measurement in their physician contracts. The pace varies by payer and region, but the trend is consistent with CMS’s direction.