Telehealth Billing Guide 2026 | The Complete Guide to Billing Virtual Visits to Medicare and Commercial Insurance
Here is a scenario that is playing out in practices across the country right now.
A therapist finishes a 55-minute telehealth session on a Tuesday afternoon. She documents the session, notes the start and stop times, and submits the claim. She uses the same code and modifier combination she has used for two years. The claim comes back denied three weeks later.
What changed?
Telehealth billing in 2026 changed — significantly.
The American Medical Association introduced an entirely new family of CPT codes for virtual visits. The old telephone codes (99441–99443) were permanently deleted. CMS declined to adopt most of the new codes for Medicare. Commercial insurers started following the new codes while Medicare did not. And the result is a dual-track billing system where the exact same telehealth visit gets billed with completely different codes depending on whether the patient has Medicare or a commercial plan.
If nobody told your billing team about that, you are not alone. But every claim you have submitted incorrectly since January 2025 is either denied or at risk of audit recovery.
This guide covers everything that changed in telehealth billing 2026, what codes to use for Medicare versus commercial insurance, which modifiers apply and when, how Place of Service codes affect your reimbursement by as much as $42 per visit, and the ten most common telehealth billing mistakes that are costing practices real money right now.
Why Telehealth Billing 2026 Is More Complicated Than It Has Ever Been
Telehealth billing has never been simple. But 2026 introduced a level of complexity that catches practices off guard even when they think they are keeping up.
Here is the core problem: the AMA and CMS are no longer on the same page.
The AMA — which creates CPT codes — introduced a new telehealth code series (98000 through 98016) designed to make virtual visit billing as logical and consistent as in-person visit billing. These codes cover audio-video visits, audio-only visits, and brief virtual check-ins, all organized by time and medical decision-making complexity, just like in-person E/M codes.
CMS looked at those new codes and determined that most of them were duplicative of existing Medicare billing mechanisms. So CMS declined to recognize codes 98000 through 98015 for Medicare reimbursement.
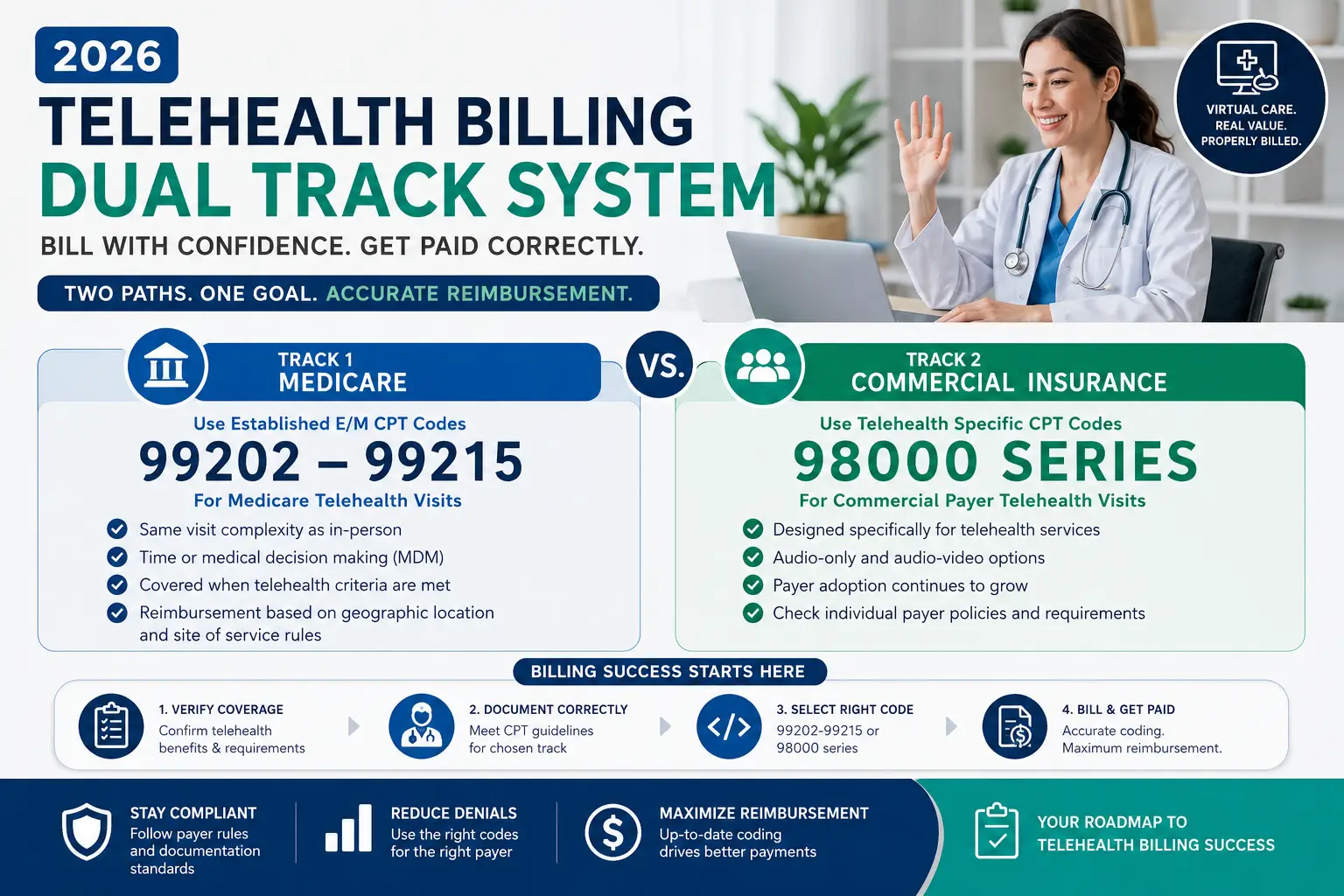
The result: commercial payers and many state Medicaid programs are billing 98000-series codes. Medicare is still billing traditional E/M codes with modifiers. Your practice needs to know which track applies to which patient — and apply the right codes, the right modifiers, and the right Place of Service codes — on every single claim.
One more complexity layer: CPT codes 99441, 99442, and 99443 — the telephone visit codes that have been a fixture in telehealth billing since the pandemic — were permanently deleted effective January 1, 2025. Any claim submitted with those codes in 2026 is automatically denied. No exceptions.
According to the CMS Official Telehealth FAQ updated February 2026, telehealth geographic restrictions have been permanently removed for behavioral health services, and audio-only telehealth for behavioral health remains covered through at least December 31, 2027. These are important protections for mental health providers — but they require specific billing compliance to access.
Let us map both tracks clearly.
Track 1: Medicare Telehealth Billing 2026
For Medicare Fee-for-Service patients, telehealth billing 2026 works on a familiar foundation — standard office E/M codes — but with specific modifiers and POS codes that tell CMS the visit was delivered virtually.
Medicare Telehealth CPT Codes in 2026
Office E/M Codes (Audio-Video Visits):
| CPT Code | Visit Type | Key Rule |
|---|---|---|
| 99202 | New patient, Level 2 | Low MDM or 15-29 min |
| 99203 | New patient, Level 3 | Low MDM or 30-44 min |
| 99204 | New patient, Level 4 | Moderate MDM or 45-59 min |
| 99205 | New patient, Level 5 | High MDM or 60-74 min |
| 99211 | Established, Level 1 | Clinical staff, no physician required |
| 99212 | Established, Level 2 | Straightforward MDM or 10-19 min |
| 99213 | Established, Level 3 | Low MDM or 20-29 min |
| 99214 | Established, Level 4 | Moderate MDM or 30-39 min |
| 99215 | Established, Level 5 | High MDM or 40-54 min |
These are the same codes used for in-person visits. What makes them telehealth claims is the modifier and POS code combination — not the CPT code itself. Medicare identifies telehealth delivery through POS and modifier combinations, not through telehealth-specific CPT codes.
Brief Virtual Check-In:
CPT 98016 — This code replaced HCPCS G2012, which was deleted. It covers 5-to-10-minute technology-based communications with established patients. Two critical rules apply: the service cannot relate to an E/M visit provided within the prior 7 days, and it cannot result in an E/M visit within the next 24 hours. Medicare reimburses 98016 at approximately $16.50 nationally. This is the only code from the 98000-series that Medicare accepts.
Asynchronous E-Visits (Patient Portal Messages):
| CPT Code | Time | Reimbursement (approx.) |
|---|---|---|
| 99421 | 5-10 minutes cumulative | ~$15 |
| 99422 | 11-20 minutes cumulative | ~$29 |
| 99423 | 21+ minutes cumulative | ~$46 |
These codes cover asynchronous digital communications — when a patient sends a message through a patient portal and the provider reviews and responds without a real-time visit. Time is cumulative over a 7-day period.
Deleted codes — Do NOT use in 2026:
- 99441 — Telephone E/M, 5-10 minutes (DELETED)
- 99442 — Telephone E/M, 11-20 minutes (DELETED)
- 99443 — Telephone E/M, 21-30 minutes (DELETED)
- G2012 — Brief virtual check-in (DELETED — replaced by 98016)
Any claim submitted with these codes in 2026 is automatically denied before a human reviewer even sees it.
Medicare Telehealth Modifiers in 2026
Modifiers tell Medicare how the service was delivered. Getting this wrong is one of the top causes of telehealth claim denials.
Modifier 95 — Real-time audio AND video: This is the primary telehealth modifier for Medicare in 2026. Use it when the service was delivered via real-time, interactive audio and video — both modalities present simultaneously.
- Use with standard E/M codes (99202–99215) for audio-video visits
- Do NOT use for audio-only visits
- Do NOT use when billing 98000-series codes to commercial payers (the modality is built into those codes)
Modifier 93 — Audio-only (telephone): Use Modifier 93 when the visit was conducted by telephone or other audio-only technology, without video.
- Required by Medicare for audio-only visits
- Document in the note why video was not used (patient unable or unwilling to use video technology)
- Do NOT use for audio-video visits
- Medicare extended audio-only telehealth coverage through December 31, 2027 — but only when clinically appropriate and documented
Modifier GT — Legacy modifier, mostly retired: Modifier GT was the original telehealth identifier for Medicare. CMS has largely transitioned to Modifier 95, but GT may still appear in limited situations at Critical Access Hospitals billing under Method II. For most practices in 2026, use Modifier 95 — not GT.
Medicare Place of Service Codes — The $42 Difference
This is the detail that costs practices the most money when they get it wrong.
POS 10 — Telehealth in the patient’s home: When the patient is located in their private home during the telehealth visit, use POS 10. This reimburses at the higher non-facility rate — equivalent to what Medicare pays for an in-office visit.
POS 02 — Telehealth outside the patient’s home: When the patient is at any location other than their private home — a clinic, office, skilled nursing facility, school, or workplace — use POS 02. This reimburses at the lower facility rate.
The math that makes this matter: For a 99214 established patient visit in 2026, the difference between POS 10 (non-facility rate) and POS 02 (facility rate) is approximately $42 per visit. Over a full year of telehealth sessions with multiple patients, that difference compounds into thousands of dollars of revenue either captured or missed.
How to document it correctly: At the start of every telehealth session, document the patient’s location in your note. “Patient is participating from their home at [city, state].” That one line determines POS 10 eligibility and protects the payment in any audit review.
The in-person visit requirement for behavioral health: Per the CMS 2026 Physician Fee Schedule, Medicare requires an in-person, non-telehealth visit within 6 months prior to the first mental health telehealth service. This requirement applies after December 31, 2027 — meaning it is currently deferred but approaching. Mental health providers should begin planning workflows to accommodate this requirement before it takes effect.
Track 2: Commercial Insurance Telehealth Billing 2026
Commercial payers — Blue Cross Blue Shield, UnitedHealthcare, Aetna, Cigna, Humana, and others — have largely adopted the new 98000-series CPT codes that Medicare declined. This creates the dual-track system that is the source of most telehealth billing confusion in 2026.
The New 98000-Series Code Structure
The AMA organized the new telehealth codes into two families: audio-video visits and audio-only visits.
Audio-Video Telehealth Visit Codes (98000–98007):
| CPT Code | Patient Type | MDM/Time |
|---|---|---|
| 98000 | New patient | Straightforward / 15-29 min |
| 98001 | New patient | Low / 30-44 min |
| 98002 | New patient | Moderate / 45-59 min |
| 98003 | New patient | High / 60-74 min |
| 98004 | Established patient | Minimal / 10-19 min |
| 98005 | Established patient | Low / 20-29 min |
| 98006 | Established patient | Moderate / 30-39 min |
| 98007 | Established patient | High / 40-54 min |
Key rule for commercial payers: Do NOT add Modifier 95 or Modifier 93 when using 98000–98015 codes. The telehealth modality is built directly into the code descriptor — adding a modifier on top creates a claim error for many payers.
Audio-Only Telehealth Visit Codes (98008–98015): These replaced the deleted telephone codes 99441–99443 and support billing for synchronous phone-only visits.
| CPT Code | Patient Type | MDM/Time |
|---|---|---|
| 98008 | New patient | Straightforward / 15-29 min |
| 98009 | New patient | Low / 30-44 min |
| 98010 | New patient | Moderate / 45-59 min |
| 98011 | New patient | High / 60-74 min |
| 98012 | Established patient | Minimal / 10-19 min |
| 98013 | Established patient | Low / 20-29 min |
| 98014 | Established patient | Moderate / 30-39 min |
| 98015 | Established patient | High / 40-54 min |
Important caveat for audio-only commercial billing: Some commercial payers have restricted audio-only reimbursement to behavioral health services only. Before billing audio-only codes for non-mental health visits, verify coverage with the specific payer. Do not assume that because Medicare covers audio-only telehealth, commercial plans will too.
The Critical Verification Step Before Every Telehealth Claim
This is where most telehealth billing errors originate in 2026 — practices assuming that all payers follow the same rules.
Before submitting any telehealth claim to a commercial payer, verify three things:
- Has this payer adopted the 98000-series codes, or do they still want standard E/M codes with Modifier 95?
- Does this payer require Modifier 95 even for 98000-series codes (some do, contrary to the AMA guideline)?
- Does this payer cover audio-only visits for the specialty and service type being billed?
Assuming a commercial payer follows Medicare rules is one of the fastest ways to generate a wave of telehealth claim denials. Call provider relations or check the payer’s online billing manual before the first claim goes out — and document what you find.
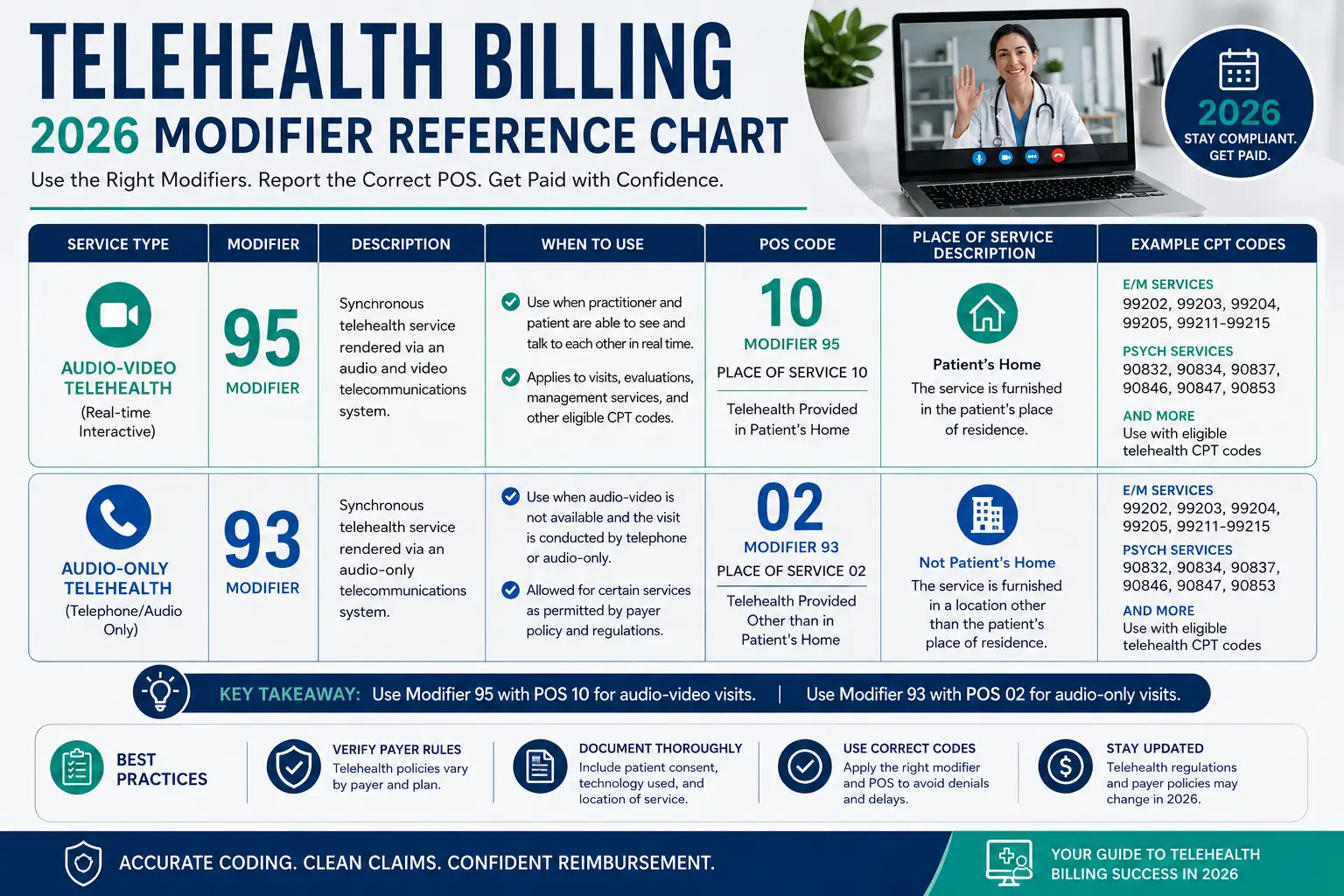
The Complete Telehealth Billing 2026 Modifier Quick Reference
| Scenario | Medicare | Commercial (98000-series) |
|---|---|---|
| Audio + Video visit, patient at home | E/M code + Mod 95 + POS 10 | 98000–98007 + POS 10 (no modifier) |
| Audio + Video, patient NOT at home | E/M code + Mod 95 + POS 02 | 98000–98007 + POS 02 (no modifier) |
| Audio-only (phone), patient at home | E/M code + Mod 93 + POS 10 | 98008–98015 + POS 10 (no modifier) |
| Audio-only (phone), NOT at home | E/M code + Mod 93 + POS 02 | 98008–98015 + POS 02 (no modifier) |
| Brief check-in (5-10 min) | CPT 98016 + POS 10 or 02 | CPT 98016 + POS 10 or 02 |
| Patient portal e-visit | 99421–99423 (no modifier) | Varies by payer |
Save this table. Print it. Put it at every billing workstation. More telehealth billing 2026 denials trace back to wrong modifier + POS combinations than to any other single cause.
Mental Health Telehealth Billing 2026 — Special Rules
Behavioral health telehealth deserves its own section because it has specific protections and requirements that do not apply to other specialties.
Permanent geographic exemption: Per the CMS FAQ, geographic restrictions for behavioral health telehealth services were permanently removed by the Consolidated Appropriations Act of 2021. Both rural and urban patients can receive mental health telehealth services from their homes — there is no location restriction. This is not a temporary waiver — it is permanent law.
Audio-only behavioral health — extended through 2027: For mental health services specifically, Medicare continues to permit audio-only telehealth through at least December 31, 2027. This means a therapist can conduct a phone-only session with an established patient and bill Medicare when video is not available or appropriate.
Documentation requirement for audio-only mental health: The clinical note must document why video was not used. “Patient does not have access to video technology” or “Patient requested audio-only due to privacy concerns at current location” — the reason needs to be in writing, specific to that session, not a standing note.
Time-based mental health codes in telehealth billing 2026: For therapists, counselors, and other non-prescribing mental health providers billing psychotherapy codes (90832, 90834, 90837), the time-based rules do not change for telehealth. The code is still determined by documented face-to-face time. What changes is the modifier and POS code on the claim.
Mental health psychotherapy telehealth claims in 2026:
- Medicare: 90832/90834/90837 + Modifier 95 (audio-video) or Modifier 93 (audio-only) + POS 10 or POS 02
- Commercial: 90832/90834/90837 + Modifier 95 + POS 10 or POS 02 (most commercial payers still want Modifier 95 on psych codes, not the new 98000-series)
This is a case where mental health billing telehealth codes follow neither pure Medicare nor pure commercial rules — therapists should verify each payer’s specific requirements for psychotherapy codes delivered via telehealth.
The Mental Health Parity Act and telehealth: Federal law under the Mental Health Parity and Addiction Equity Act requires that mental health telehealth benefits cannot be more restrictive than medical telehealth benefits under the same plan. If a commercial plan covers video visits for primary care, it must cover video visits for mental health on equivalent terms. If a payer is denying your mental health telehealth claims while paying medical telehealth claims at higher rates, parity compliance may be the issue.
Telehealth Billing 2026 and Remote Patient Monitoring — What Changed
Remote Patient Monitoring (RPM) is one of the fastest-growing revenue opportunities in telehealth billing 2026. The 2026 CMS Physician Fee Schedule introduced significant changes to RPM billing that expand access while restructuring the code requirements.
The key 2026 RPM change: A new billing threshold allows practices to bill CPT 99445 for patients who transmit 2–15 days of data in a 30-day period — previously, patients needed 16+ days of data transmission before any RPM billing was possible. This opens RPM revenue for patients with lower device compliance who previously generated no reimbursement.
Critical 2026 RPM billing rule: CPT 99445 and CPT 99454 cannot be billed for the same patient in the same 30-day period. They are mutually exclusive billing options for different data transmission volumes.
Core RPM codes that remain active in 2026:
| CPT Code | Description | 2026 Approx. Rate |
|---|---|---|
| 99453 | Initial device setup and patient education | ~$19 |
| 99454 | Device supply + 16+ days data transmission | ~$53/month |
| 99445 | Device supply + 2-15 days data transmission (NEW) | ~$28/month |
| 99457 | RPM treatment management, first 20 minutes | ~$51/month |
| 99458 | RPM treatment management, each additional 20 min | ~$41/month |
RPM pairs naturally with telehealth visits — the monitoring data informs the virtual visit, and the visit manages the monitoring program. Practices combining telehealth with RPM are capturing revenue streams that in-person-only practices cannot access.
Telehealth Documentation Requirements 2026 — What Every Note Needs
Documentation for telehealth billing 2026 must cover the same clinical content as an in-person visit — plus several telehealth-specific elements that payers require. Missing any of these creates audit exposure and denial risk.
Every telehealth visit note must include:
1. Patient consent for telehealth: Document that the patient was informed about the telehealth encounter and provided consent. Electronic consent (a signed form in the patient portal) or verbal consent with a documented note (“Patient verbally consented to telehealth services on [date]”) are both acceptable. The consent must be specific to telehealth — a general treatment consent does not satisfy this requirement.
2. Patient location: Document the patient’s location at the time of the visit — city, state, and whether they are at home. “Patient is participating from their private residence in Atlanta, Georgia” is sufficient. This information determines your POS code and is required for Medicare risk adjustment purposes.
3. Provider location: Document where the provider is located. Providers can deliver telehealth from their home per current CMS rules — but the location must be documented. Note that providers are not required to report their home address on Medicare enrollment applications to deliver telehealth from home, per current CMS guidance.
4. Technology platform: Note the technology used for the visit. For HIPAA compliance, the platform must be a HIPAA-compliant telehealth platform with a signed Business Associate Agreement. Document: “Visit conducted via [platform name], a HIPAA-compliant telehealth system.”
5. Modality — audio-video or audio-only: Explicitly state whether the visit was audio-video or audio-only. If audio-only, document why: “Video technology was not available to the patient at this time” or “Patient requested audio-only service due to [reason].” This documentation directly supports Modifier 95 (audio-video) versus Modifier 93 (audio-only) on the claim.
6. Start and end times (for time-based codes): For mental health psychotherapy codes and any time-based E/M visits, document exact start and stop times. This is required to support code selection and is the first thing auditors look for when reviewing telehealth claims.
7. Clinical content: All the same documentation required for an in-person visit — chief complaint, history, examination findings or relevant clinical assessment, medical decision-making or time-based complexity support, assessment, and plan. Telehealth does not reduce documentation requirements. It adds to them.

10 Most Common Telehealth Billing 2026 Mistakes — And How to Fix Every One
Mistake #1: Still Using Deleted Telephone Codes (99441–99443)
These codes were permanently deleted January 1, 2025. If they are still in your superbill or EHR template, every claim using them in 2026 is denied automatically.
Fix: Audit your superbills, charge capture templates, and EHR billing forms right now. Remove 99441, 99442, 99443, and G2012. Add 98016 for brief check-ins.
Mistake #2: Using 98000-Series Codes for Medicare Claims
Medicare does not recognize CPT codes 98000 through 98015. A Medicare claim submitted with these codes is denied automatically.
Fix: Create two separate billing tracks in your practice management system — one for Medicare (standard E/M + modifiers), one for commercial (98000-series where accepted). Never let Medicare claims cross into the commercial track.
Mistake #3: Adding Modifier 95 to 98000-Series Claims
When billing 98000–98015 codes to commercial payers, the telehealth modality is already embedded in the code. Adding Modifier 95 on top creates a claim formatting error for many payers.
Fix: Modifier 95 is for Medicare E/M codes and for commercial payers that still require modifiers with traditional E/M codes. Do not stack it onto 98000-series codes.
Mistake #4: Using POS 02 When POS 10 Applies
If the patient is at home, POS 10 applies — and pays at the higher non-facility rate. Using POS 02 for a home-based patient underpays the claim without generating a denial, meaning the practice never knows they left money on the table.
Fix: Ask every patient at the start of every telehealth visit: “Are you at home right now?” Document the answer. Use POS 10 for home-based patients.
Mistake #5: Not Documenting Patient Location
Without documentation of the patient’s location, you cannot justify your POS code choice in an audit — and Medicare specifically requires location documentation for certain coverage determinations.
Fix: Add a required field to your telehealth note template: “Patient location: [home/other location — city, state].” Make it the first thing entered at the start of every virtual visit.
Mistake #6: Billing Audio-Only Visits Without Documenting Why Video Was Not Used
Medicare allows audio-only billing with Modifier 93, but requires documentation explaining why the visit was audio-only. “Patient didn’t want video” is not sufficient — you need the specific reason and clinical appropriateness.
Fix: Create a standard audio-only documentation phrase for your notes: “Patient was unable to participate via video today due to [reason]. Audio-only visit was clinically appropriate as [reason]. Patient was offered video connection and declined/was unable to connect.”
Mistake #7: Billing the Same Payer Track Across All Patients
Assuming all payers follow the same telehealth billing rules — and billing everyone with the same code and modifier combination — generates denials from whichever payer is on the wrong track.
Fix: Build a payer-specific telehealth billing guide for your top 5–10 payers. Document which code track each payer uses, which modifiers they require, and whether they cover audio-only. Review it quarterly as payer policies continue to evolve.
Mistake #8: Missing the Consent Documentation Requirement
Patient consent for telehealth must be documented for every visit — not just at intake. Many practices document consent once at the beginning of the provider relationship and never again. Payer audits routinely flag this.
Fix: Add a consent acknowledgment to the start of every telehealth visit note: “Telehealth consent confirmed for today’s visit.” Keep the original signed consent form in the patient record.
Mistake #9: Not Verifying Mental Health In-Person Visit Requirement
Medicare requires an in-person visit within 6 months prior to the first mental health telehealth service — this requirement kicks in after December 31, 2027. Practices that start behavioral health telehealth relationships without any in-person history now need to plan for this.
Fix: Begin tracking which behavioral health patients have never had an in-person visit. Develop a plan for how to fulfill this requirement before 2028 — whether through a single in-person intake session or through other clinical arrangements.
Mistake #10: Not Verifying Commercial Payer Telehealth Policies Before Billing
Payer-specific telehealth billing policies in 2026 differ more than most billing teams expect. Assuming a commercial payer follows CMS rules is one of the most common reasons telehealth claim denials occur.
Fix: For every new payer relationship and at the start of every calendar year, verify telehealth billing requirements directly with the payer’s provider relations line or their published billing manual. Document what you learn. Update your payer-specific telehealth billing guide accordingly.
Telehealth Billing 2026 Compliance Checklist
Use this before billing any telehealth claim.
Before Every Telehealth Visit:
- Eligibility verified — telehealth benefits specifically confirmed
- Patient’s location confirmed — home (POS 10) or other (POS 02)
- Prior authorization checked if required by this payer for telehealth
- HIPAA-compliant platform being used (BAA in place)
During the Visit:
- Patient consent for telehealth documented
- Session start time recorded
- Patient location documented (city, state, home vs other)
- Provider location documented
- Technology platform documented
In the Clinical Note:
- Modality documented — audio-video or audio-only
- If audio-only: reason documented specifically
- Session end time recorded (for time-based codes)
- All standard clinical documentation complete
Before Claim Submission:
- Correct code track identified — Medicare (E/M + modifier) or commercial (98000-series)
- Correct modifier applied — 95 (audio-video Medicare/commercial E/M) or 93 (audio-only)
- Correct POS code applied — 10 (home) or 02 (other location)
- Deleted codes (99441–99443, G2012) confirmed absent from claim
- Payer-specific telehealth rules verified for this payer
- Claim scrubbed before submission
How Pro Health Care Advisors Handles Telehealth Billing 2026
Telehealth billing in 2026 is not something you figure out once and you are done. CMS updates rules quarterly. Commercial payers update their coverage policies regularly. The dual-track system requires constant payer-specific verification that cannot be done once and forgotten.
At Pro Health Care Advisors, our medical billing and RCM team handles telehealth billing for small and individual practices across multiple specialties — including primary care, mental health, cardiology, and family practice.
Here is what we do for telehealth billing specifically:
Payer-specific telehealth billing verification: We maintain current telehealth billing requirements for every major payer in our clients’ payer mixes — updated as payers release new policies. No claims go out on the wrong billing track.
Dual-track claim management: We build and maintain separate billing workflows for Medicare and commercial telehealth claims, ensuring the right codes, modifiers, and POS codes are applied to every claim based on the patient’s coverage.
Documentation review: We flag telehealth documentation gaps before claims go out — missing consent, missing patient location, missing modality documentation. These gaps cost practices during audits even when the clinical work was completely appropriate.
Compliance monitoring through MD Audit Shield: Our MD Audit Shield program monitors telehealth billing patterns for the statistical anomalies that attract CMS audit attention — including audio-only claim volumes, modifier usage rates, and code selection patterns compared to specialty peers.
Mental health telehealth credentialing: For mental health providers who became Medicare providers under the 2024 LPC/LMFT expansion, our physician credentialing team handles Medicare enrollment and telehealth credentialing to ensure every provider can bill virtual visits correctly from day one.
HIPAA compliance for telehealth: We ensure our clients’ telehealth billing workflows meet HIPAA compliance standards — BAAs in place, documentation practices current, and staff training covering telehealth-specific privacy requirements.
Contact our team today for a free telehealth billing review. We will identify which of the 10 common mistakes are affecting your practice right now — and show you exactly what it takes to fix them.
Frequently Asked Questions: Telehealth Billing 2026
Q: What CPT codes do I use for telehealth billing in 2026 for Medicare?
A: For Medicare telehealth billing 2026, use standard office E/M codes (99202–99215) with Modifier 95 for audio-video visits or Modifier 93 for audio-only visits, plus POS 10 (patient at home) or POS 02 (patient at other location). For brief virtual check-ins of 5–10 minutes, use CPT 98016, which replaced the deleted G2012. Do not use CPT codes 98000–98015 for Medicare — CMS does not recognize them. Do not use deleted codes 99441–99443 under any circumstances.
Q: What CPT codes do I use for commercial insurance telehealth billing 2026?
A: Most commercial payers have adopted the new 98000-series codes for telehealth billing 2026. Use 98000–98007 for audio-video visits and 98008–98015 for audio-only visits, without adding Modifier 95 or 93 (the modality is built into the code). However, payer adoption varies — always verify with each specific commercial payer before billing 98000-series codes, as some commercial payers still prefer traditional E/M codes with Modifier 95.
Q: What is the difference between POS 10 and POS 02 in telehealth billing 2026?
A: POS 10 applies when the patient is in their private home during the telehealth visit. It reimburses at the higher non-facility rate, equivalent to in-office reimbursement. POS 02 applies when the patient is at any other location — clinic, office, skilled nursing facility, school, workplace. It reimburses at the lower facility rate. The difference can be $30–$50 per visit depending on the code — always document patient location and apply the correct POS code.
Q: Is audio-only telehealth billing still allowed in 2026?
A: Yes, for specific services and payers. Medicare extended audio-only telehealth coverage through December 31, 2027 for behavioral health services and some other limited services. For Medicare audio-only visits, use standard E/M codes with Modifier 93. Some commercial payers also cover audio-only, particularly for behavioral health, but coverage varies. Always document why video was not used and verify each payer’s audio-only coverage before billing.
Q: Are telehealth claims audited more than in-person claims?
A: Yes — telehealth claims are subject to increased audit scrutiny in 2026, particularly from RAC contractors and Medicare Administrative Contractors reviewing for documentation completeness, correct modifier usage, and appropriate POS code selection. The OIG compliance guidance identifies telehealth billing as a continued area of focus. Maintaining complete documentation and following the dual-track billing system correctly is essential for audit protection.
Q: Can I provide telehealth from my home in 2026?
A: Yes. Providers can deliver telehealth services from their homes. Current CMS rules do not require providers to report their home address on Medicare enrollment applications to provide telehealth from home. However, provider location must be documented in the clinical note for every telehealth visit.
Q: What happened to CPT codes 99441, 99442, and 99443?
A: These telephone visit codes were permanently deleted effective January 1, 2025. They have been replaced by the new 98008–98015 audio-only code series for commercial payers. For Medicare, audio-only visits are billed using standard E/M codes with Modifier 93. Any claim submitted with 99441, 99442, or 99443 in 2026 is automatically denied — no exceptions.
Q: How do I bill mental health telehealth differently from medical telehealth in 2026?
A: Mental health psychotherapy codes (90832, 90834, 90837) are typically billed the same way for both Medicare and commercial payers — with Modifier 95 for audio-video or Modifier 93 for audio-only, plus the appropriate POS code. Most commercial payers have not moved mental health psychotherapy codes to the 98000-series system. Geographic restrictions for behavioral health telehealth have been permanently removed. Audio-only mental health telehealth is covered by Medicare through December 31, 2027. An in-person visit requirement for the first mental health telehealth service begins after December 31, 2027.