Hypertension ICD-10 Codes 2026 — Complete I10 to I16 Billing Guide
Nearly half of American adults have hypertension — which makes I10 one of the most frequently reported ICD-10 codes in clinical practice. It is also one of the most frequently coded incorrectly.
The single most common error in hypertension billing is using I10 (essential hypertension) when the patient’s documentation actually supports a more specific combination code — I11, I12, or I13. According to coding guidance from CodeICD’s hypertension coding guidelines, coding I10 when I11 or I12 applies is one of the top mistakes coders make, and it is a leading cause of claim denials in cardiology and internal medicine billing.
This guide walks through every hypertension ICD-10 code from I10 to I16, the “assumed causal relationship” rule that determines which code applies, the combination code logic that trips up even experienced coders, and the documentation requirements that prevent denials.
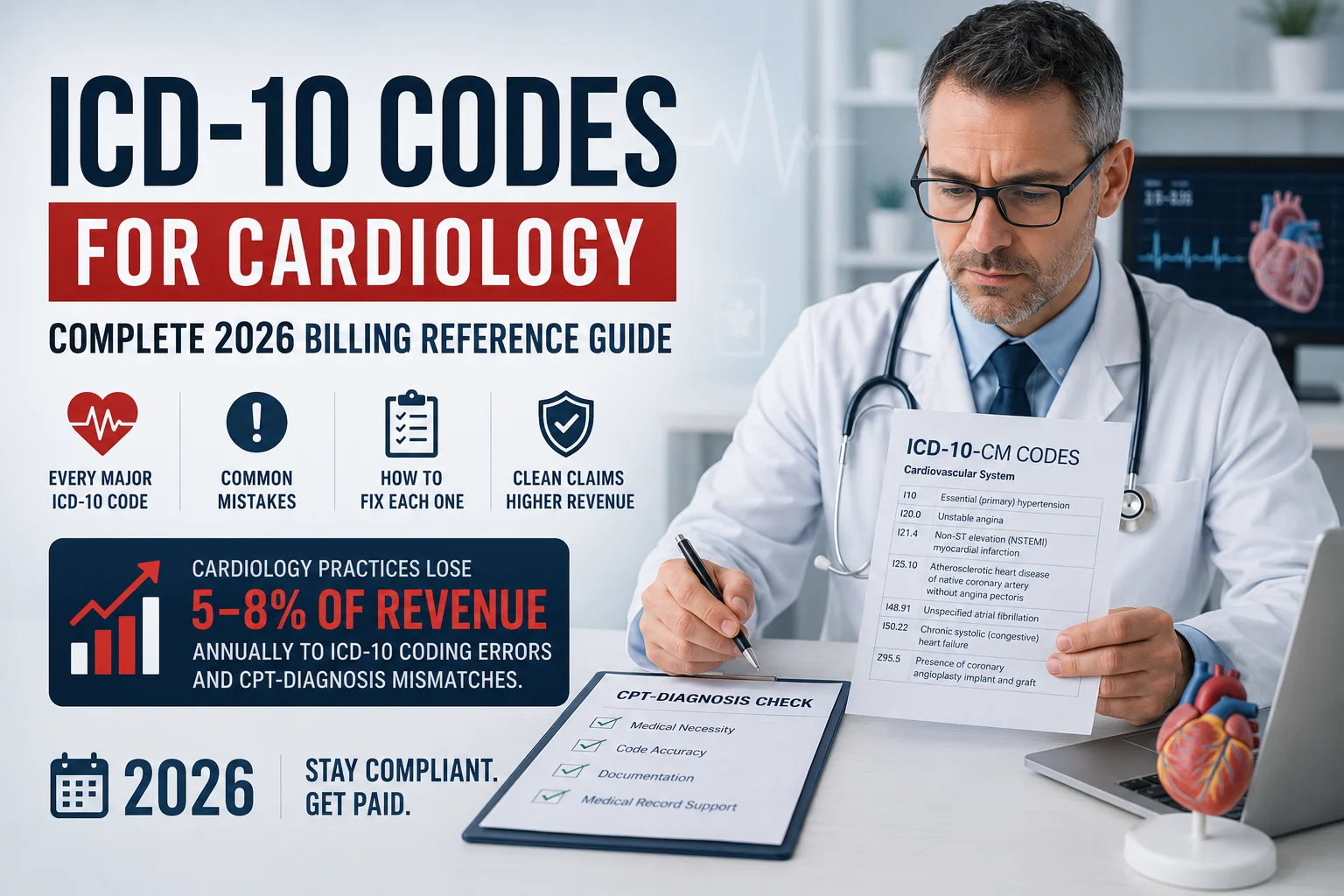
For the complete cardiology ICD-10 reference covering all major cardiac conditions, see our ICD-10 codes for cardiology guide.
The Hypertension Code Family — I10 Through I16
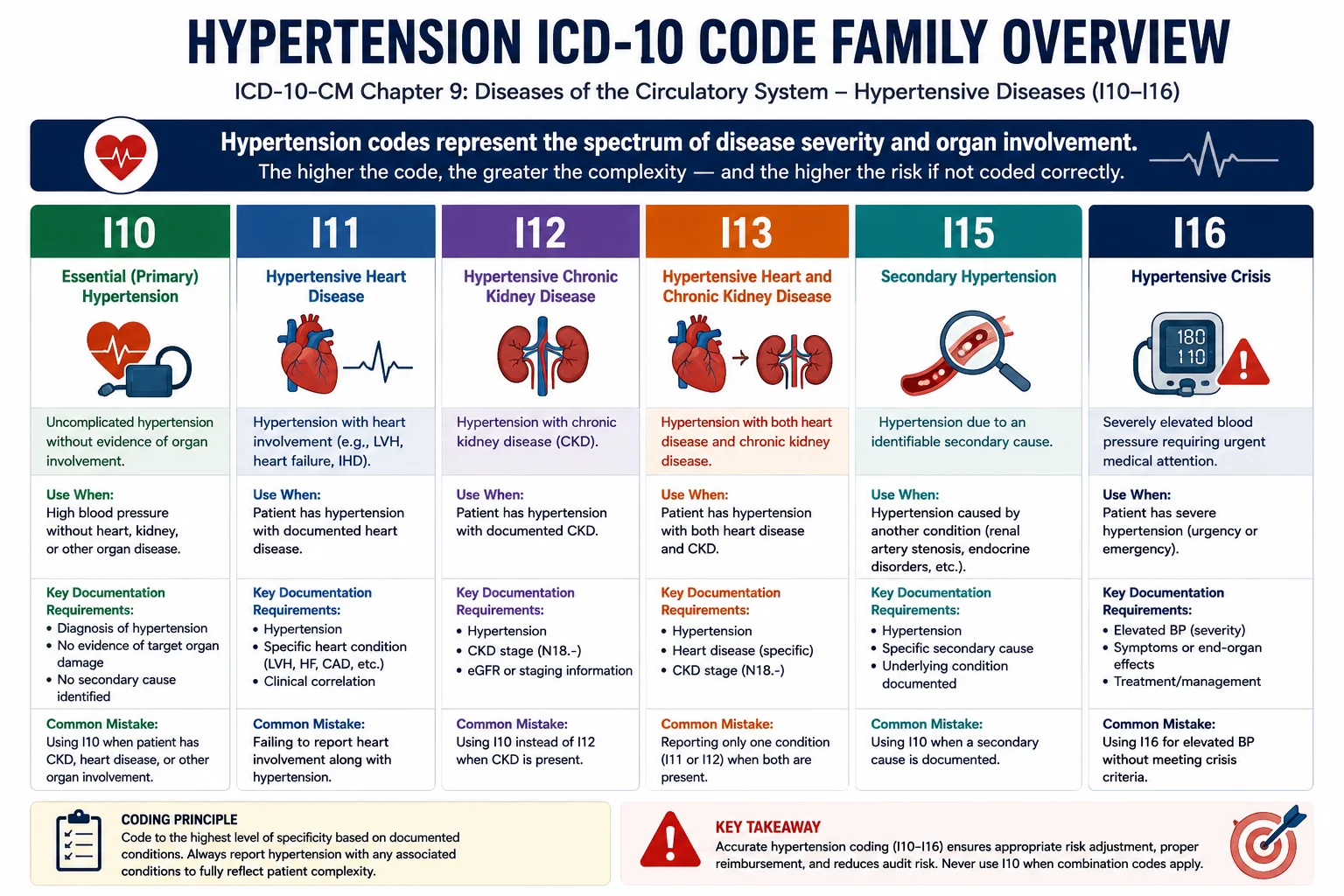
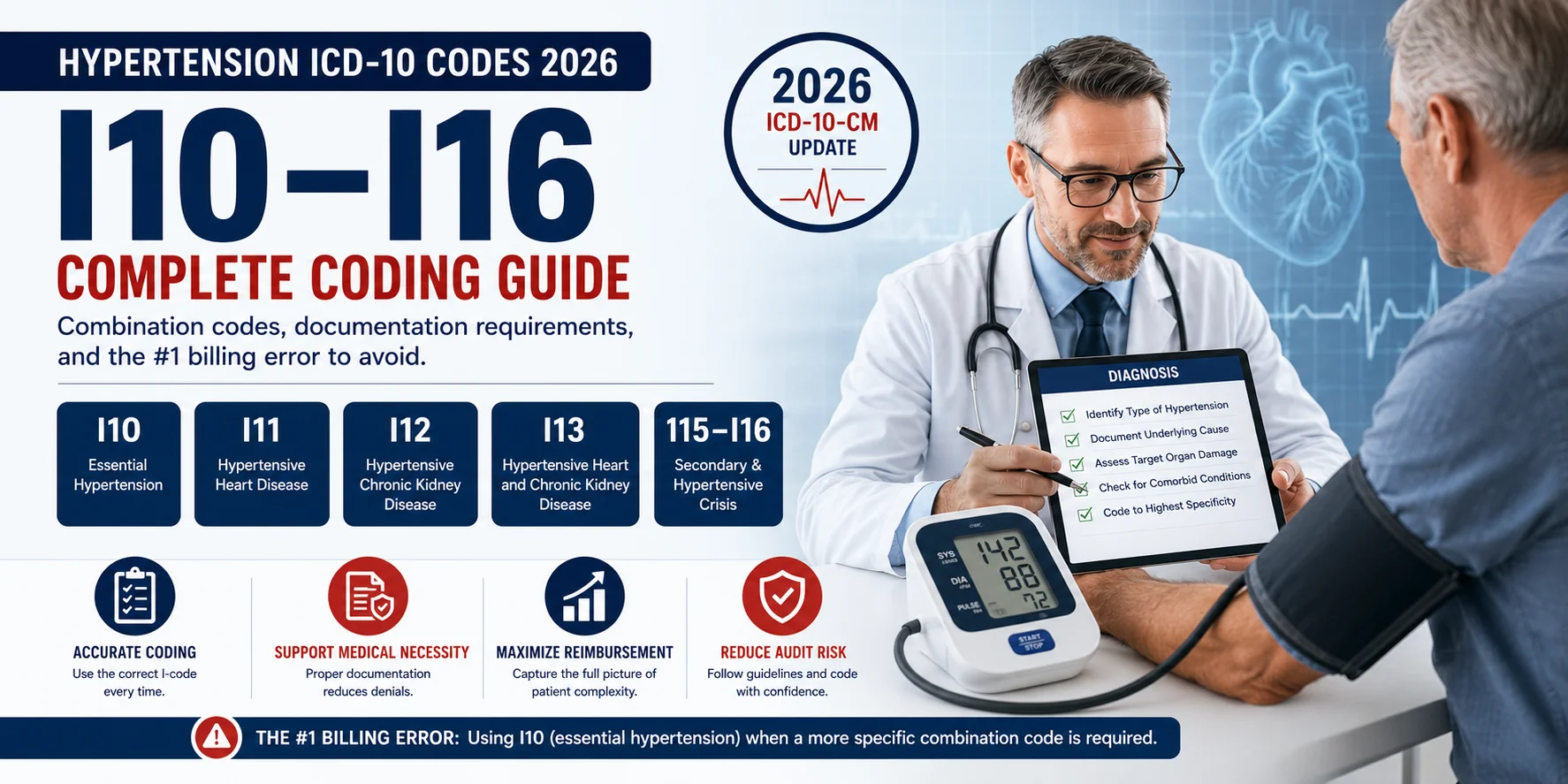
Hypertension codes in ICD-10-CM span categories I10 through I16 in Chapter 9 — Diseases of the Circulatory System. Each category represents a different level of organ involvement:
| Code Range | Category | What It Captures |
|---|---|---|
| I10 | Essential (primary) hypertension | Hypertension alone, no organ complications |
| I11 | Hypertensive heart disease | Hypertension + heart disease |
| I12 | Hypertensive chronic kidney disease | Hypertension + CKD |
| I13 | Hypertensive heart and CKD | Hypertension + heart disease + CKD |
| I15 | Secondary hypertension | Hypertension caused by an identifiable underlying condition |
| I16 | Hypertensive crisis | Hypertensive urgency or emergency |
| I1A.0 | Resistant hypertension | Uncontrolled despite 3+ medications |
According to Patient Notes’ hypertension coding guide, I10 — essential (primary) hypertension — is the most commonly reported hypertension code, used when a patient has high blood pressure without a documented secondary cause.
I10 — Essential (Primary) Hypertension
Use I10 only when the patient has documented hypertension with no related heart disease, no chronic kidney disease, and no identifiable secondary cause.
Critical rule: Do not assign I10 from a blood pressure reading alone. An isolated elevated BP reading without a formal hypertension diagnosis is coded R03.0 (elevated blood-pressure reading, without diagnosis of hypertension) — not I10. The provider must document an actual diagnosis of hypertension, not just a number on a chart.
Controlled vs. uncontrolled: ICD-10-CM does not differentiate between controlled and uncontrolled essential hypertension. Both use I10. However, according to PatientNotes’ clinical guidance, documenting whether hypertension is controlled or uncontrolled still matters — it supports quality measures (HEDIS, MIPS), care planning, and medication management decisions, even though it does not change the base code.
2026 HCC change to note: Under the CMS HCC Model v28, fully phased in for 2026, I10 alone no longer maps to any Hierarchical Condition Category. This is a significant change for risk-adjustment purposes — practices participating in value-based payment models need to ensure that hypertension with organ complications is captured using the correct I11, I12, or I13 code, since I10 alone does not contribute to risk scores under the updated model.
I11 — Hypertensive Heart Disease
I11 applies when hypertension and certain heart conditions coexist. This is where the “assumed causal relationship” rule becomes essential to understand.
Per ICD-10-CM Official Guidelines, when hypertension and specific heart conditions coexist, the coder must assume a causal relationship — even if the physician has not explicitly written “hypertensive heart disease” in the note. If the patient has documented hypertension and a qualifying heart condition, I11 applies by default.
| Code | Description | Additional Code Required |
|---|---|---|
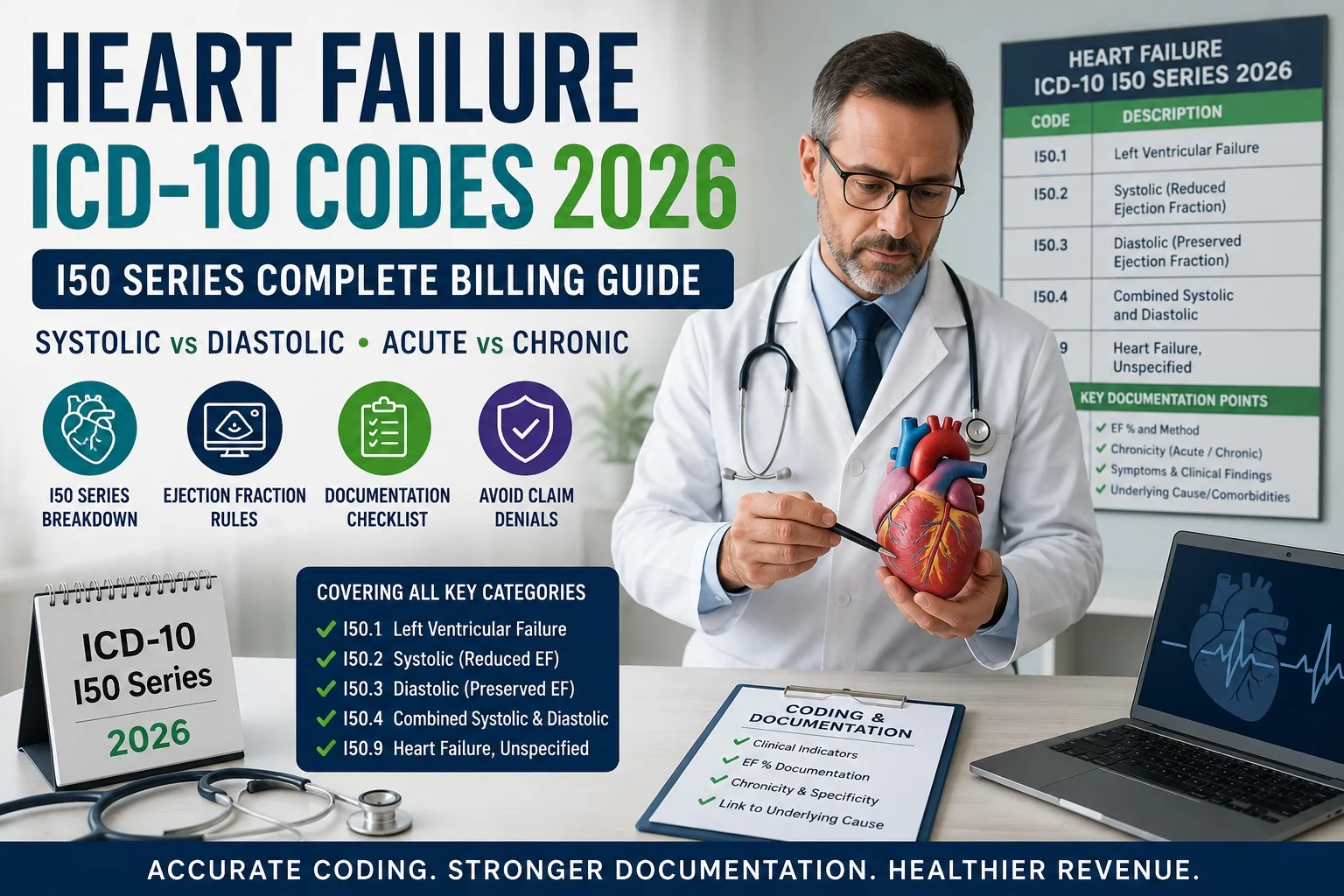
| I11.0 | Hypertensive heart disease with heart failure | Yes — append an I50.x code specifying the heart failure type |
| I11.9 | Hypertensive heart disease without heart failure | No additional heart failure code needed |
The most common sequencing error: When I11.0 applies, an additional code from the I50 series is required to specify the type of heart failure (systolic, diastolic, or combined). Missing this second code results in incomplete coding — and per Outsource Strategies’ coding guidance, this combination is required: report I11.0 for hypertension and heart failure, with an additional code from the I50 series to identify the specific type. For our complete heart failure coding breakdown, see our cardiology ICD-10 reference guide.
Important exception: Coronary artery disease (I25.x) is NOT assumed to be causally related to hypertension. Do not assign I11 based solely on the coexistence of hypertension and CAD — these must be coded separately unless the provider documents a direct causal link.
I12 — Hypertensive Chronic Kidney Disease
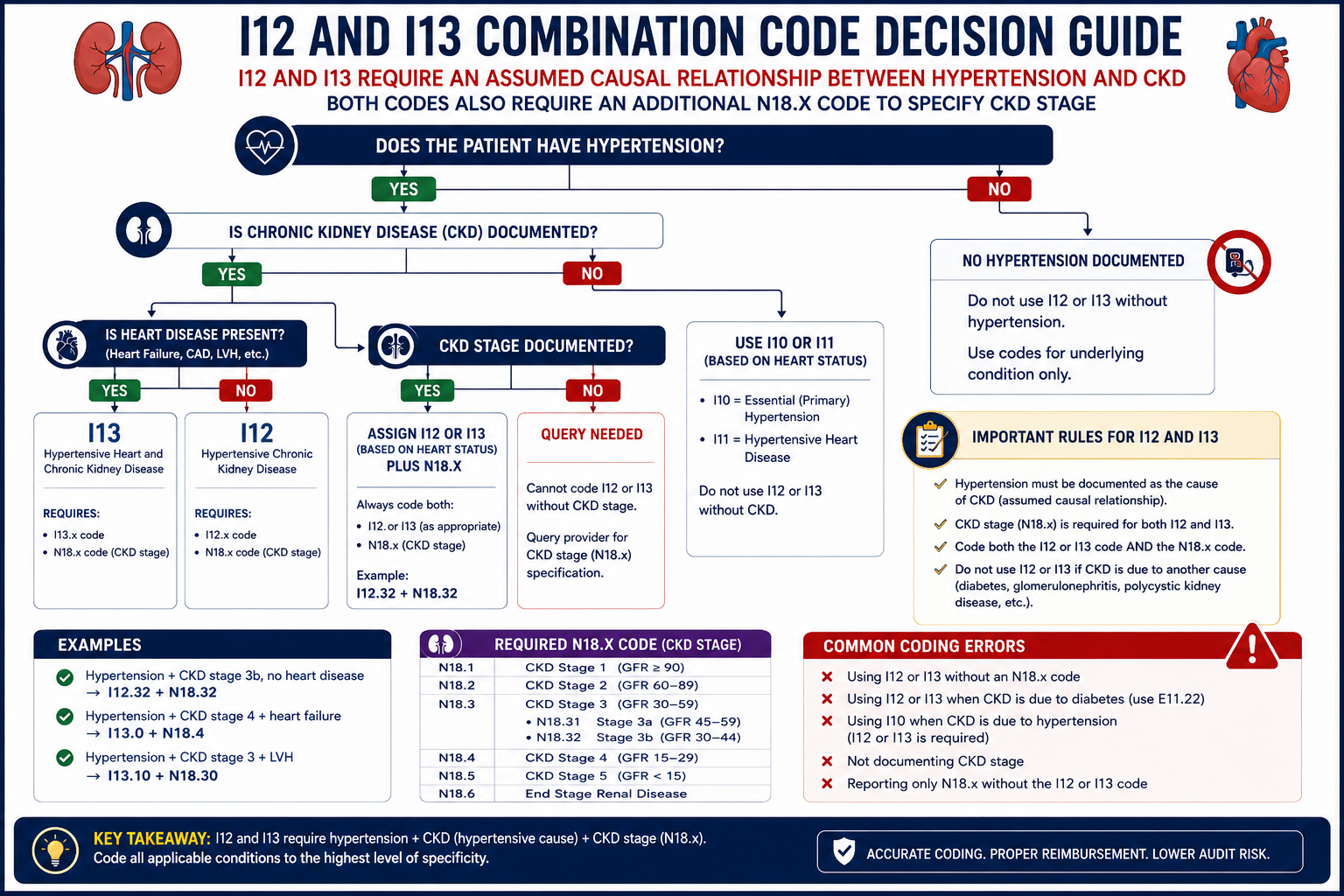
Per ICD-10-CM Official Guidelines Section I.C.9.a.2, the classification presumes a causal relationship between hypertension and chronic kidney disease. Assign I12 codes when both hypertension and a condition classifiable to N18.x (CKD) are present — use I12 regardless of which condition is documented as the primary reason for the encounter, unless the provider explicitly states the CKD is unrelated to the hypertension.
| Code | Description |
|---|---|
| I12.0 | Hypertensive CKD with stage 5 CKD or end-stage renal disease |
| I12.9 | Hypertensive CKD with stage 1–4 CKD, or unspecified CKD |
Mandatory additional code: I12 codes always require an additional N18.x code to specify the CKD stage:
| N18 Code | CKD Stage |
|---|---|
| N18.1 | Stage 1 |
| N18.2 | Stage 2 (mild) |
| N18.3 | Stage 3 (moderate) |
| N18.4 | Stage 4 (severe) |
| N18.5 | Stage 5 |
| N18.6 | End-stage renal disease |
| N18.9 | Unspecified |
A patient with hypertension and stage 3 CKD is coded I12.9 + N18.3 — never I12.9 alone.
Breaking the assumption: If the provider explicitly documents “hypertension unrelated to CKD” or “CKD due to diabetes, not hypertension,” the coder may use I10 and N18.x separately without I12 — but this requires explicit physician documentation stating the conditions are unrelated. The assumption only breaks when the provider says so directly.
I13 — Hypertensive Heart and Chronic Kidney Disease
I13 is the combination code used when a patient has hypertension with both heart disease and chronic kidney disease simultaneously.
According to CodeICD’s coding guidelines, this is one of the most frequently mis-sequenced code families in hypertension billing: when both heart disease and CKD are present with hypertension, the I13 combination code must be used — separate I11 + I12 codes are incorrect.
| Code | Description |
|---|---|
| I13.0 | Hypertensive heart and CKD with heart failure and stage 1–4 CKD, or unspecified CKD |
| I13.10 | Hypertensive heart and CKD without heart failure, with stage 1–4 CKD |
| I13.11 | Hypertensive heart and CKD without heart failure, with stage 5 CKD or ESRD |
| I13.2 | Hypertensive heart and CKD with heart failure and stage 5 CKD or ESRD |
Two additional codes are required with every I13 code:
- An I50.x code specifying the type of heart failure (when heart failure is present)
- An N18.x code specifying the CKD stage
A patient with hypertension, chronic systolic heart failure, and stage 3a CKD is correctly coded: I13.0 + I50.22 (chronic systolic heart failure) + N18.3 (CKD stage 3). Missing either supporting code results in incomplete coding that can trigger payer review.
Sequencing rule: I13.x is sequenced first, followed by the heart failure type code, then the CKD stage code. Sequencing the heart failure code before I13.x is a documented coding pitfall that audit reviewers specifically flag.
I15 — Secondary Hypertension
I15 is used when hypertension has an identifiable underlying cause — distinct from essential (primary) hypertension, where no specific cause is found.
| Code | Description |
|---|---|
| I15.0 | Renovascular hypertension |
| I15.1 | Hypertension secondary to other renal disorders |
| I15.2 | Hypertension secondary to endocrine disorders |
| I15.8 | Other secondary hypertension |
| I15.9 | Secondary hypertension, unspecified |
Use I15 when hypertension is documented as caused by a specific identifiable condition — such as renal artery stenosis, an endocrine disorder, or another defined secondary cause. If the cause is not specified, I10 (essential hypertension) remains the default.
I16 — Hypertensive Crisis
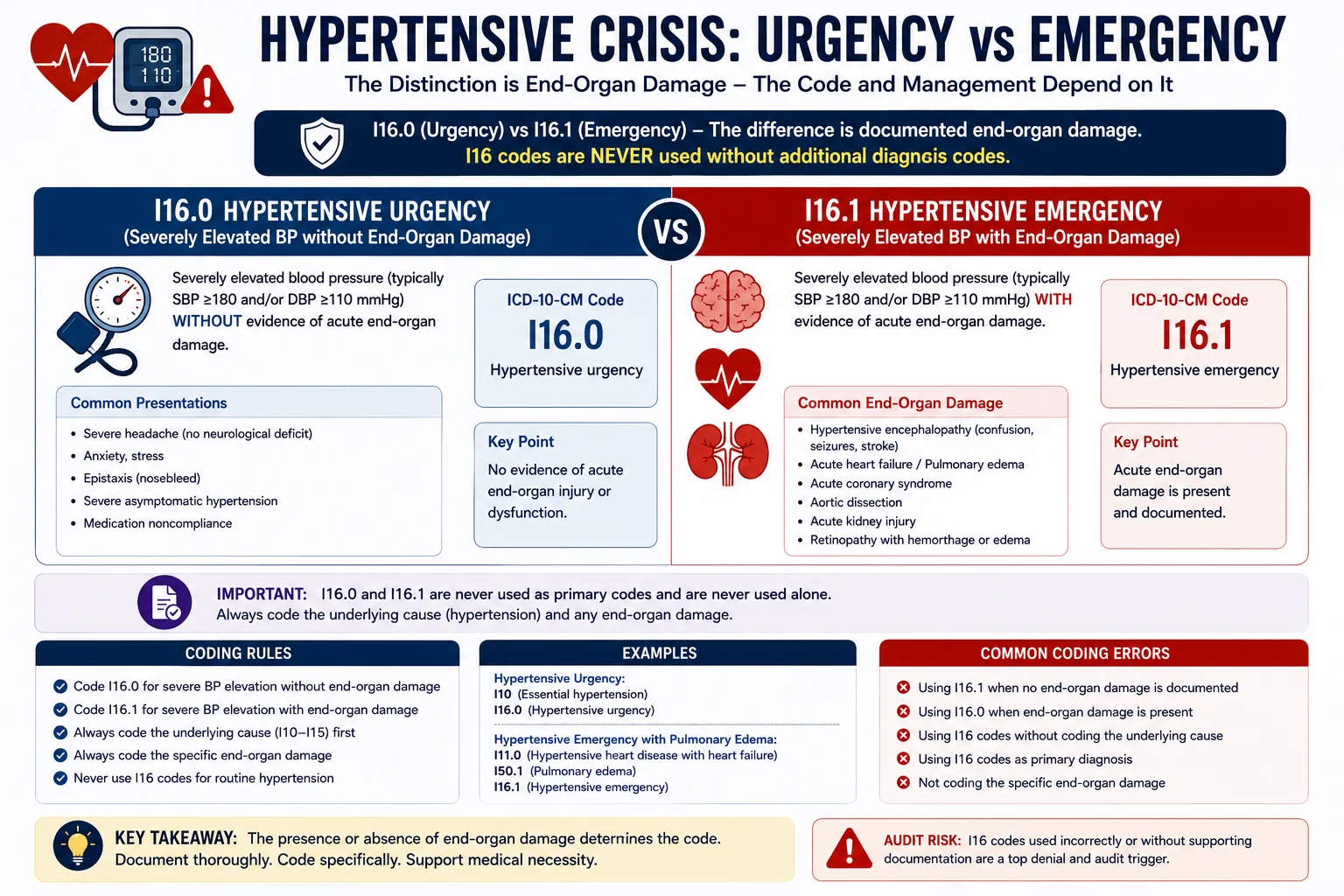
Hypertensive crisis refers to a severe, acute elevation in blood pressure — typically above 180/120 mmHg — requiring urgent medical evaluation. ICD-10-CM divides this into two clinically distinct categories based entirely on whether acute end-organ damage is documented.
| Code | Description | Requirement |
|---|---|---|
| I16.0 | Hypertensive urgency | Severe BP elevation without acute organ damage |
| I16.1 | Hypertensive emergency | Severe BP elevation WITH acute, life-threatening organ damage |
Critical rule — I16 is never standalone. Hypertensive crisis codes are not used by themselves. Always pair I16.x with the underlying hypertension type code (I10 through I15). For example, a patient presenting with hypertensive emergency and acute kidney injury, with no prior hypertension history beyond essential hypertension, would be coded:
I16.1 (hypertensive emergency) + I10 (essential hypertension) + N17.9 (acute kidney injury)
Sequence: the crisis code first, then the underlying hypertension type, then any acute end-organ damage code.
The “With” Convention — Why This Rule Trips Up So Many Coders
The single most important concept in hypertension coding is the ICD-10-CM “with” convention — the assumed causal relationship rule. Here is the complete logic:
Hypertension + heart conditions (I50, I51.4–I51.9) = assumed related → use I11
Hypertension + chronic kidney disease (any stage) = assumed related → use I12
Hypertension + heart conditions + CKD = assumed related → use I13
Hypertension + coronary artery disease (I25.x) = NOT assumed related → code separately
The exception that breaks the assumption: if the provider explicitly states the conditions are unrelated — “CKD due to diabetes, not hypertension” — the coder may code them separately. Without that explicit statement, the assumed relationship governs code selection regardless of what the provider listed as the primary reason for the visit.
Special Coding Situations
Hypertension in pregnancy: Use Chapter 15 codes (O10–O16), not I10–I16, for any hypertension documented during pregnancy. O10.x codes are specific by trimester — for example, O10.011 (pre-existing essential hypertension, first trimester) or O10.213 (pre-existing hypertensive heart disease with heart failure, third trimester). Do not assign I10–I16 codes during pregnancy when an O10.x code applies.
Hypertension and diabetes: Unlike hypertension with heart disease or CKD, there is no assumed causal relationship between hypertension and diabetes. These must be coded separately — the appropriate diabetes code (such as E11.x for Type 2) alongside the hypertension code, unless a specific combination code applies.
Resistant hypertension: There is no separate ICD-10-CM code distinguishing resistant hypertension from other hypertension types. Code the underlying hypertension type (I10, or I11/I12/I13 if organ involvement is present). Document the resistance clearly in the clinical note — while it does not change the code, clear documentation supports medical necessity for additional workup, specialist referrals, and intensive management. An additional code (Z79.899) may be appropriate to capture long-term drug therapy.
Tobacco use: An additional ICD-10 code is required for all hypertension codes if the patient currently uses tobacco or has used it previously. Tobacco use status directly affects risk stratification and should always be captured alongside hypertension coding.
The 5 Most Common Hypertension Billing Errors
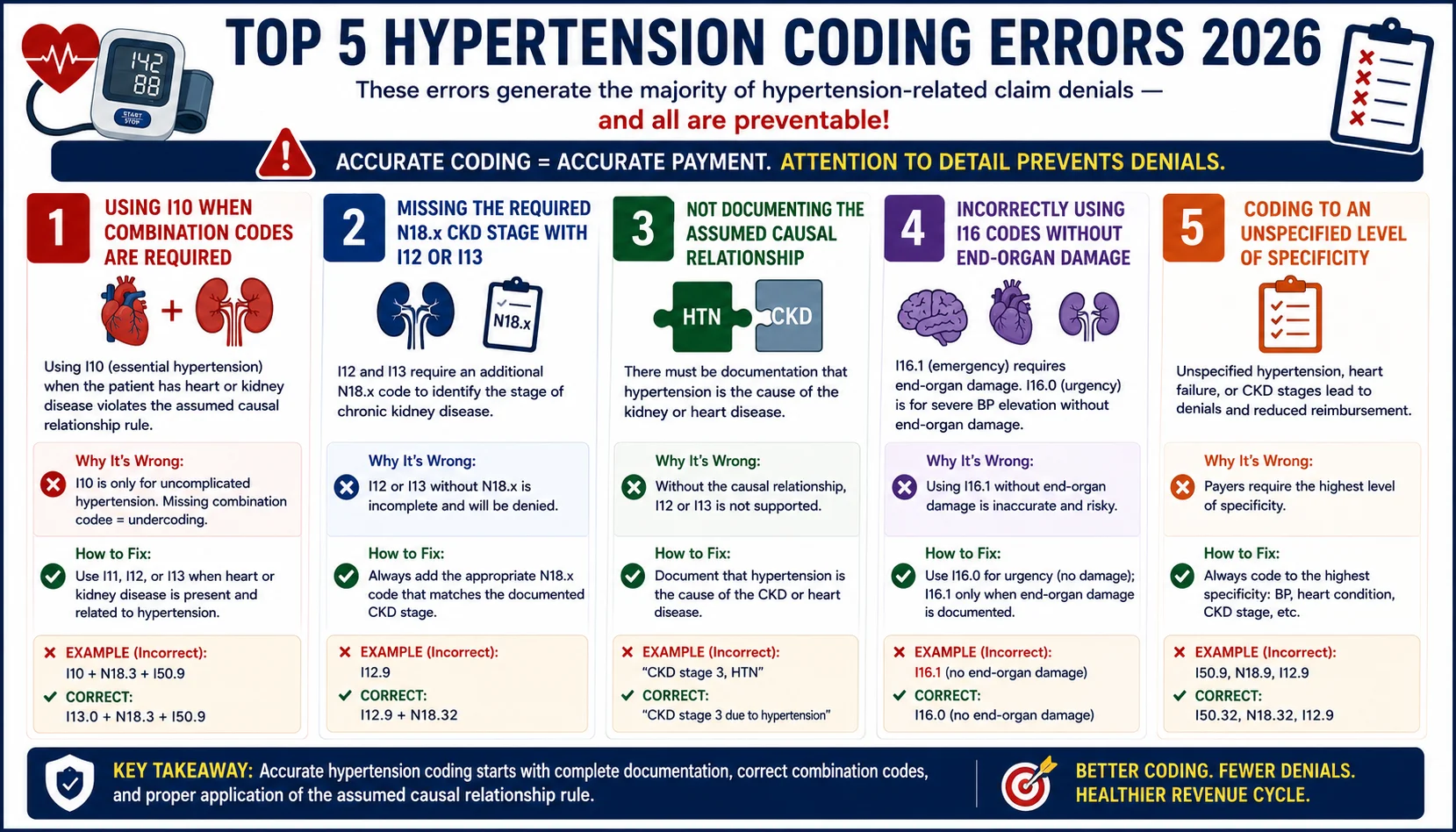
Error 1: Using I10 when I11, I12, or I13 applies. If the patient has hypertension plus documented heart disease or CKD, I10 is incorrect — the combination code is required by the assumed causal relationship rule, regardless of which condition prompted the visit.
Error 2: Using separate I11 + I12 codes instead of the I13 combination code. When both heart disease and CKD coexist with hypertension, I13 must be used. Reporting I11 and I12 together instead of I13 is a documented coding pitfall.
Error 3: Missing the required N18.x or I50.x companion code. I12 and I13 always require an N18.x code specifying CKD stage. I11.0 and I13.0/I13.2 always require an I50.x code specifying heart failure type. Submitting the hypertension code alone, without its required companion code, results in incomplete coding.
Error 4: Coding R03.0 instead of I10. R03.0 is for an isolated elevated blood pressure reading without a formal hypertension diagnosis. Once a provider documents an actual hypertension diagnosis, use I10 or the appropriate combination code — not R03.0.
Error 5: Using I16 (hypertensive crisis) without the underlying hypertension code. I16.x codes are never standalone. Every hypertensive crisis claim must also include the underlying hypertension type code from I10 through I15.
How Pro Health Care Advisors Handles Hypertension Coding
Our cardiology billing services include AAPC-certified coders who apply the assumed causal relationship rule correctly on every hypertension claim — verifying that combination codes (I11, I12, I13) are used when documentation supports them, and that every required companion code (N18.x for CKD stage, I50.x for heart failure type) is included before submission.
Our CodeMAXX services specifically catch the incomplete-coding pattern where I12 or I13 is billed without its required companion code — a common and easily preventable source of claim holds and payer queries.
For our complete cardiology ICD-10 reference covering coronary artery disease, heart failure, atrial fibrillation, and acute MI coding, see our ICD-10 codes for cardiology guide.
Frequently Asked Questions — Hypertension ICD-10 Codes
Q: What is the difference between I10, I11, I12, and I13? I10 is used for uncomplicated essential hypertension with no organ involvement. I11 applies when hypertension causes heart disease. I12 is the combination code for hypertensive chronic kidney disease. I13 is used when both hypertensive heart disease and chronic kidney disease are present simultaneously. Selecting the wrong category — for example, using I10 when I13 applies — is a leading cause of claim denials.
Q: Does controlled vs. uncontrolled hypertension change the ICD-10 code? No. ICD-10-CM uses I10 for both controlled and uncontrolled essential hypertension. The distinction does not change the code, but documenting it supports quality measures (HEDIS, MIPS) and care planning decisions.
Q: Is hypertension assumed to be related to coronary artery disease? No. Unlike heart failure and chronic kidney disease, coronary artery disease (I25.x) is NOT assumed to be causally related to hypertension under ICD-10-CM guidelines. Do not assign hypertensive heart disease (I11) based solely on the coexistence of hypertension and CAD.
Q: What additional code is required with I12 or I13? Both I12 and I13 require an additional N18.x code specifying the chronic kidney disease stage (N18.1 through N18.6, or N18.9 for unspecified). I13.0 and I13.2 also require an I50.x code specifying the type of heart failure.
Q: How is hypertension coded during pregnancy? Hypertension during pregnancy uses Chapter 15 codes (O10–O16), not the standard I10–I16 codes. These pregnancy-specific codes are trimester-specific and supersede the standard hypertension codes for the duration of the pregnancy.
For more on cardiology billing and the broader ICD-10 landscape, see our complete ICD-10 codes for cardiology guide and our medical billing denial codes reference.
The Bottom Line
Hypertension coding looks simple — one common condition, one common code. But the combination code rules for I11, I12, and I13 are where claims most often go wrong, and the financial impact compounds across every patient with cardiovascular or renal comorbidities.
Getting hypertension coding right is not just about avoiding denials. Under the 2026 HCC v28 model, I10 alone no longer contributes to risk adjustment — meaning practices that fail to capture organ involvement with the correct combination codes are also leaving risk-adjustment revenue on the table in value-based care arrangements.
Schedule Your Free Consultation with Pro Health Care Advisors →