Prior Authorization Rules Changed in 2026 — What Every Provider Must Know
If you have noticed something feels heavier about your front desk workflow lately — more paperwork, tighter deadlines, stricter documentation — you are not imagining it.
The rules changed. Not quietly, not gradually. January 1, 2026 flipped a switch that every medical practice in America is now feeling.
Three major things happened at the same time, and most providers are still catching up to all three. This guide breaks down exactly what changed, what it means for your day-to-day operations, and — most importantly — what you need to do right now so your claims do not start piling up in a denial queue.
Let’s walk through this together, step by step.
What Is Prior Authorization, and Why Does It Keep Getting Talked About?
If you already know what prior authorization is, feel free to skip ahead. But for anyone new to running a practice or just joining the front desk team — here is the simple version:
Prior authorization (PA) is the process where your practice asks the patient’s insurance company, “Hey, is it okay if we do this procedure, run this test, or prescribe this medication?” — before you actually do it.
Think of it like asking your parents for permission before buying something expensive. Except in this case, if you forget to ask, or if the insurance company takes too long to answer, your patient doesn’t get care on time — and your practice doesn’t get paid.
For years, this system has been slow, paper-heavy, and frustrating. According to the American Medical Association (AMA), physicians and their staff spend an average of 13 hours per week just on prior authorization paperwork alone. That is nearly two full working days — every single week — that could be spent on patient care.
In 2026, CMS (Centers for Medicare & Medicaid Services) decided: enough is enough.
The Big Three Changes That Hit on January 1, 2026
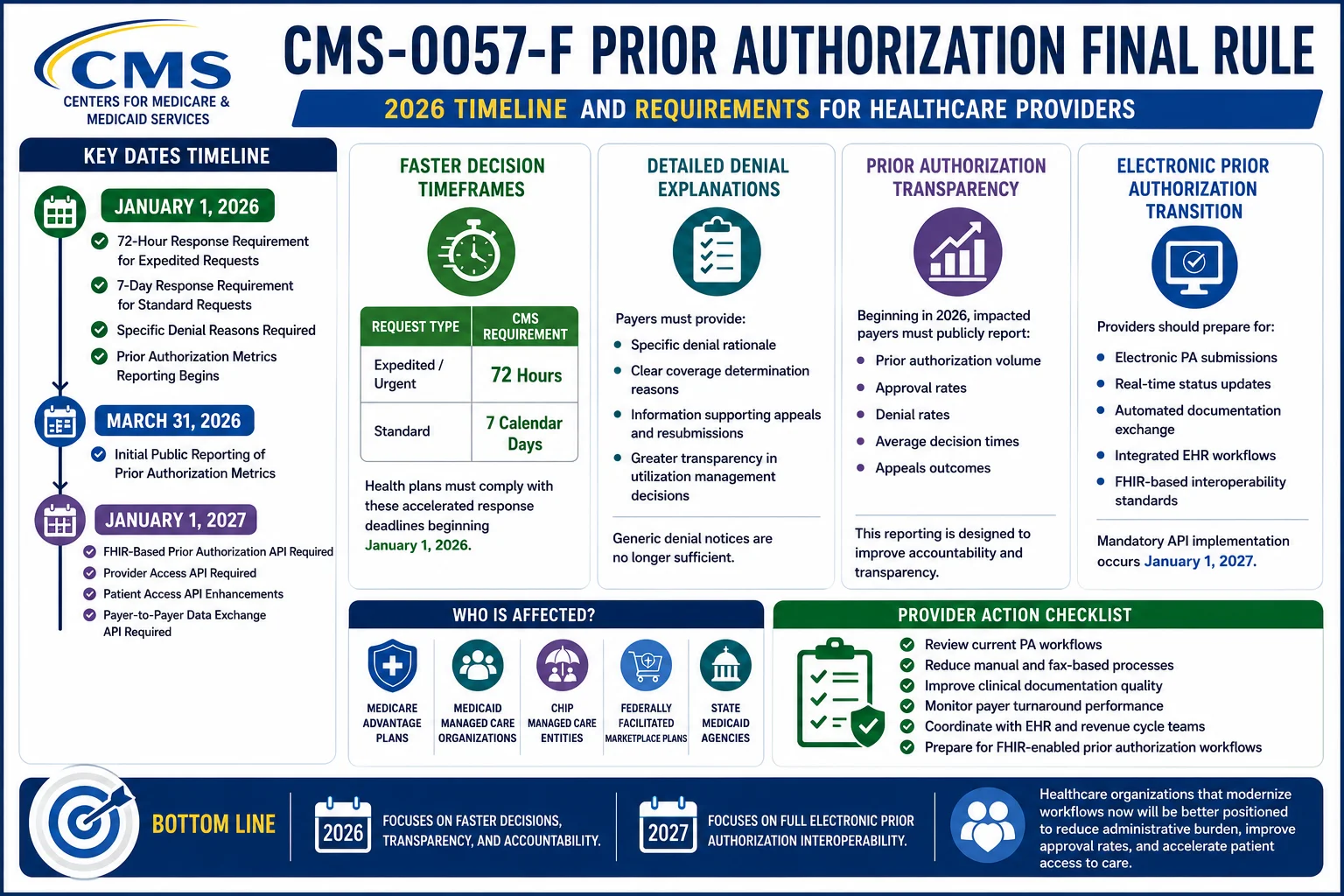
Change #1: The CMS-0057-F Final Rule Went Live
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) was finalized back in January 2024. Payers had two years to get ready. That preparation window is now over.
Here is what the rule now requires from insurance plans — actively, today:
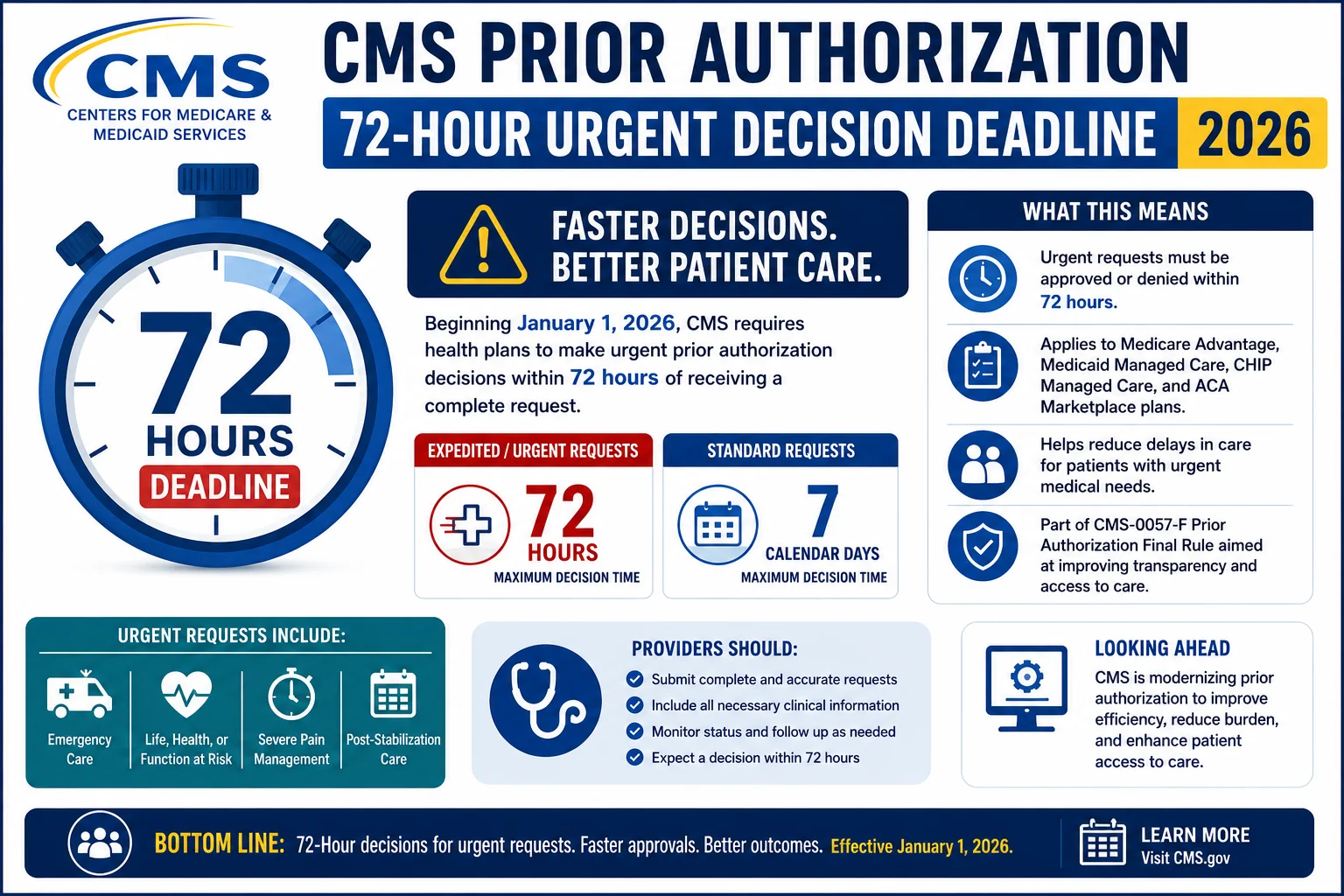
Faster decision timelines:
- Urgent (expedited) requests: Decision must come within 72 hours
- Standard (non-urgent) requests: Decision must come within 7 calendar days
Before this rule, some payers were taking 14, 21, even 30+ days on standard requests. Now that is no longer legally acceptable for Medicare Advantage, Medicaid, CHIP, and Marketplace (Federally-facilitated Exchange) plans.
Mandatory denial reasons:
When a payer denies a prior authorization request, they are now required to tell you why — in specific, actionable terms. No more vague “does not meet criteria” responses that leave you guessing what documentation was missing.
Which payers does this cover?
- Medicare Advantage plans
- Medicaid and CHIP programs
- ACA Marketplace (FFE) plans
Note: Traditional fee-for-service Medicare has its own separate change (see WISeR below).
Why this matters for your practice: Faster decisions mean faster patient scheduling and faster cash flow. But it also means payers will now expect complete, clean documentation upfront — because they have less time to go back and forth with you. Sloppy prior auth submissions will now get denied faster, not slower.
Change #2: WISeR — Prior Authorization Comes to Traditional Medicare for the First Time
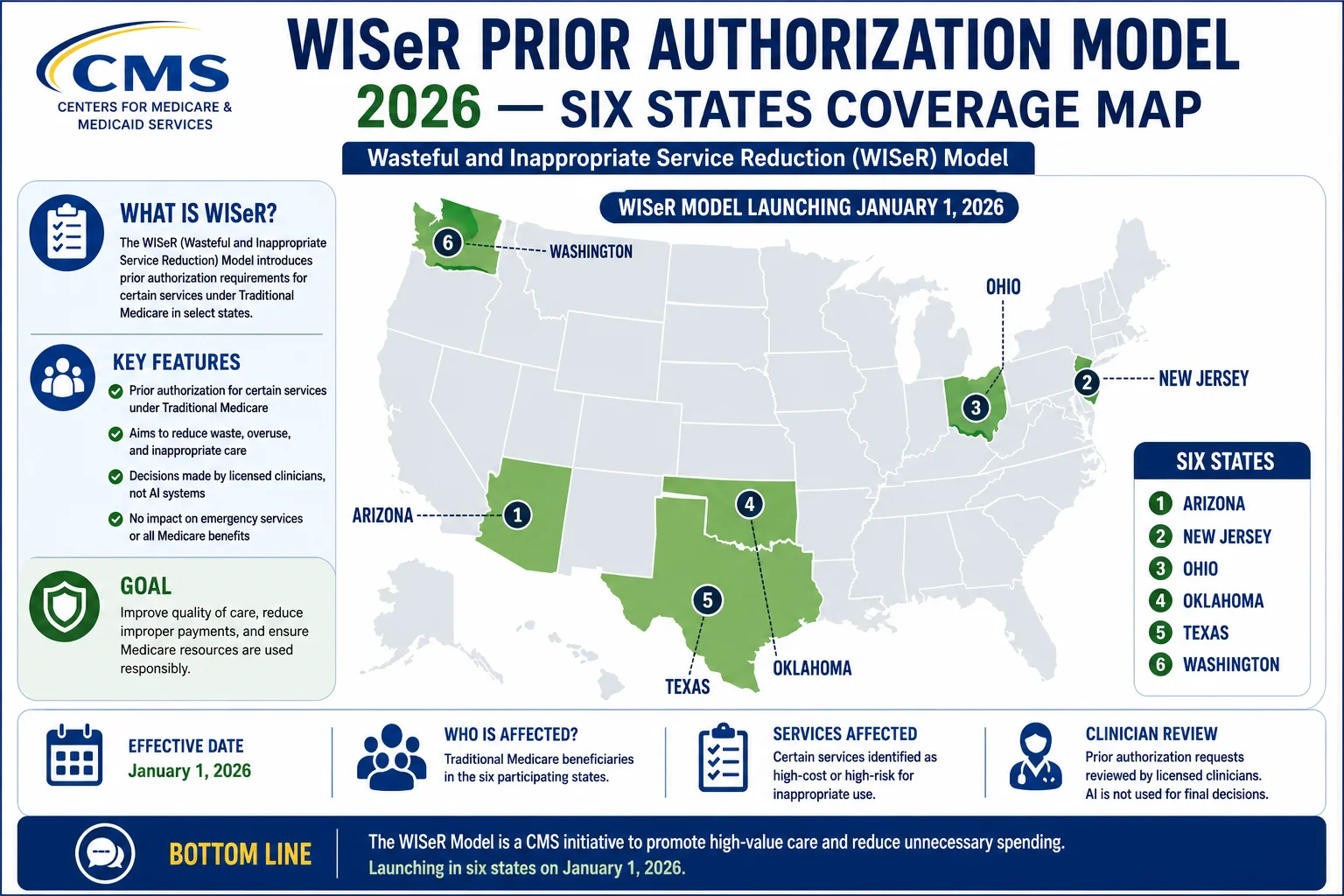
This is the one that surprised many providers the most.
For decades, traditional Medicare (fee-for-service Medicare) did not require prior authorization for most services. That changed on January 1, 2026.
The WISeR Model — which stands for Wasteful and Inappropriate Service Reduction — is a new pilot program launched by the Center for Medicare and Medicaid Innovation (CMMI). It requires prior authorization for certain outpatient services in six states:
- Arizona
- New Jersey
- Ohio
- Oklahoma
- Texas
- Washington
The WISeR model targets 17 specific outpatient services that CMS has identified as frequently overused. These include procedures like nerve stimulators and certain knee surgeries. If your practice is in one of these six states and you perform any of the targeted services — you now have two choices:
- Get advance prior authorization before the procedure
- Risk claim delay or outright denial
If you are in a WISeR state and were not aware of this change, it is worth reviewing your recent claims immediately. Any targeted service performed without the required authorization after January 1, 2026 may already be sitting in a denial queue.
For a full list of targeted services and documentation requirements, visit the CMS WISeR Model page.
Change #3: A New Round of Proposed Rules Is Already Coming
Even as the current rules are being absorbed, CMS released a new set of proposed rules in April 2026 specifically targeting prescription drug prior authorizations. This expansion would bring the same interoperability and timeline requirements to the pharmacy benefit side of healthcare.
What this means practically: the prior authorization reform wave is not stopping in 2026. It is accelerating. Practices that build strong prior auth workflows now will be in a far better position when the next wave of regulations rolls in.
The Electronic Prior Authorization Push: What Is FHIR and Why Should You Care?
You may have heard the term “ePrior Auth” or “FHIR” floating around in recent months. Here is the plain-English version of what that means:
FHIR (Fast Healthcare Interoperability Resources) is a technical standard — basically a common language that allows your Electronic Health Record (EHR) system to automatically talk to an insurance company’s prior authorization system.
Right now, most prior authorizations are handled through phone calls, fax machines, and manual portal logins. FHIR-based electronic prior authorization (ePa) would allow your EHR to check eligibility, see what documents are needed, and submit the authorization request — all without anyone picking up a phone.
CMS has mandated that electronic prior authorization interfaces from impacted payers go live on January 1, 2027. That gives practices and EHR vendors roughly six months to prepare.
What you should be doing right now:
- Ask your EHR vendor if they are on track for FHIR-based ePa integration
- Check whether your top payer contracts are covered under CMS-0057-F
- Make sure your billing team understands the new documentation standards
If you need support navigating these transitions, our team at ProHealthCare Advisors can help you map your current workflow against the new requirements.
The Real-World Impact: What Happens When Practices Miss These Requirements
Let us talk about money, because that is ultimately what keeps a practice running.
Claim denial rates have hit 10–15% industry-wide in 2026. That is not a statistic to gloss over. For a practice seeing 500 patients a month, a 12% denial rate means roughly 60 claims per month going unpaid — at least initially. And a large share of denied claims never get reworked at all. That revenue is simply written off.
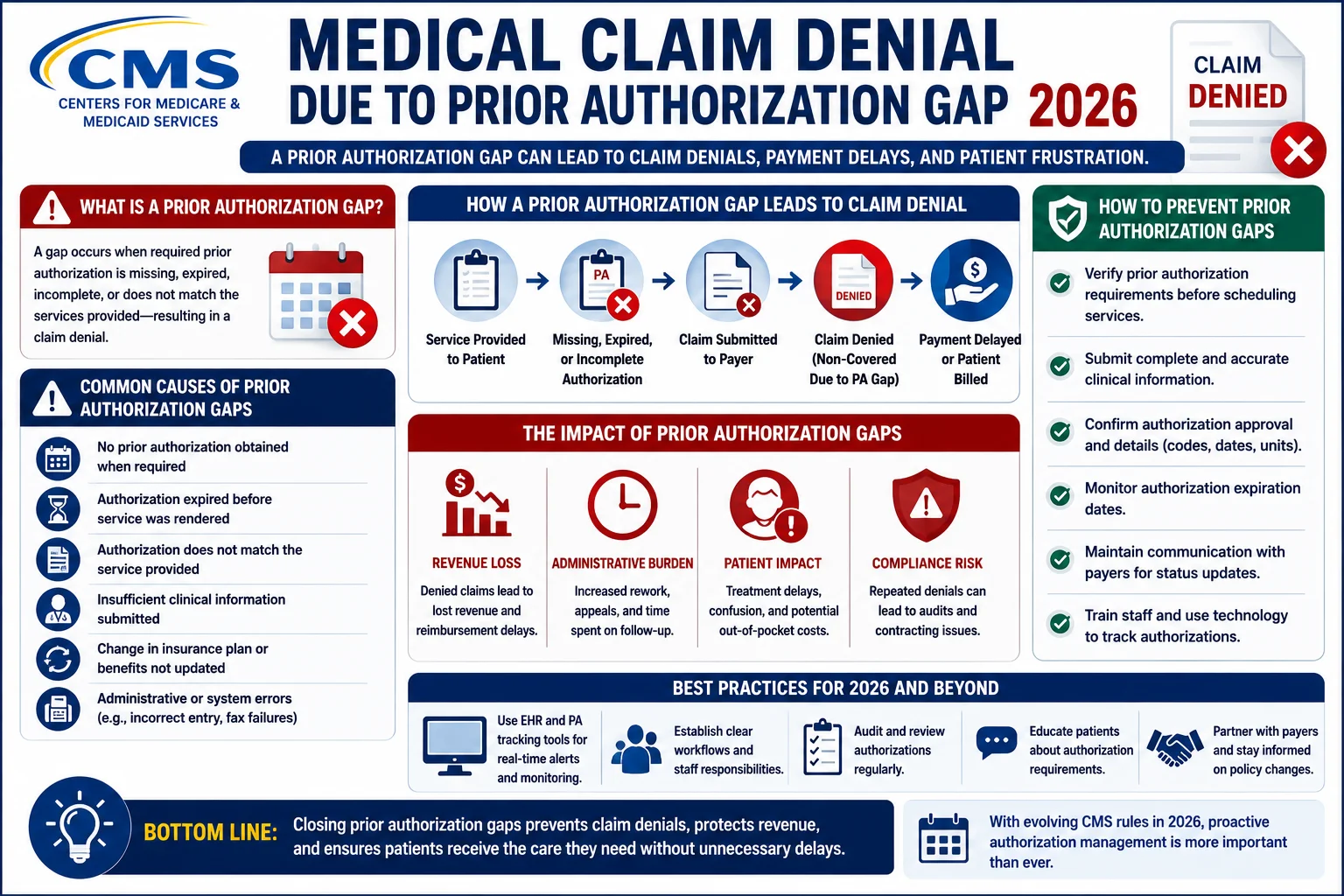
The top reasons prior authorization denials are increasing this year:
1. Missing or expired prior authorizations (especially WISeR-state practices)
If you are in one of the six WISeR states and did not update your authorization workflows at the start of the year, claims for targeted services may have been going out without required PAs since January.
2. Documentation that does not match the new specificity requirements
CMS and payers expect complete clinical documentation upfront — not after a denial. The shorter decision windows payers now have means they are more likely to deny first and ask questions never.
3. Credentialing gaps that make PAs appear invalid
When a provider’s credentials expire or payer enrollment lapses, prior authorizations tied to that provider can be denied retroactively. This is one of the quietest but most damaging revenue leaks in any practice.
At ProHealthCare Advisors, we offer eligibility verification and prior authorization management services that catch these gaps before they become denials. For practices struggling with credentialing specifically, our medical credentialing services ensure your providers stay enrolled and compliant at all times.
State-Level Prior Authorization Reforms: More Is Coming
While CMS has been moving at the federal level, individual states are also piling on with their own reforms in 2026:
- Kentucky introduced legislation requiring insurers to establish PA exemption programs
- Missouri proposed cutting certain PA requirements altogether starting this summer
- North Dakota, Nebraska, and Alaska enacted laws at the start of 2026 requiring faster PA response times from insurers
If your practice operates in multiple states or sees patients across state lines through telehealth, you now have a patchwork of timelines, exemptions, and documentation requirements to navigate. This is exactly where having a billing and authorization partner becomes invaluable rather than optional.
The Industry Pledge: Major Plans Are Already Making Moves
It is not all bad news. Following a landmark HHS/CMS industry pledge signed in 2025, major health plans have begun voluntarily reducing their prior authorization requirements.
As of April 2026, leading health plans collectively announced they had eliminated 11% of prior authorizations across a range of medical services — representing 6.5 million fewer PA requests for patients and providers. One large national plan committed to eliminating authorization requirements for 30% of its covered services, with an additional 30% reduction