Top Medical Billing Mistakes Costing Your Practice Revenue in 2026
Let me ask you something straight: do you actually know where your money is going?
Every single week, healthcare practices across the United States submit thousands of insurance claims — and a big chunk of them come back denied, underpaid, or just stuck somewhere in a queue that nobody is watching. It does not show up in patient satisfaction scores. Nobody talks about it at the front desk. But it quietly drains your revenue, month after month, year after year.
According to the American Medical Association (AMA), the national average claim denial rate has hit 12% in 2026. That means for every $100,000 your practice bills out, you could be losing $12,000 — sometimes more — before you even notice.
The good news? Almost every single one of these billing mistakes is 100% preventable. You just have to know what to look for.
In this guide, we are going to walk through the biggest medical billing mistakes costing practices real money right now — explained in plain English, no confusing medical billing jargon. Whether you are a solo physician, a practice manager, or running a growing multi-provider clinic, keep reading. This one is for you.
Why Billing Errors Hit Harder in 2026 Than Ever Before
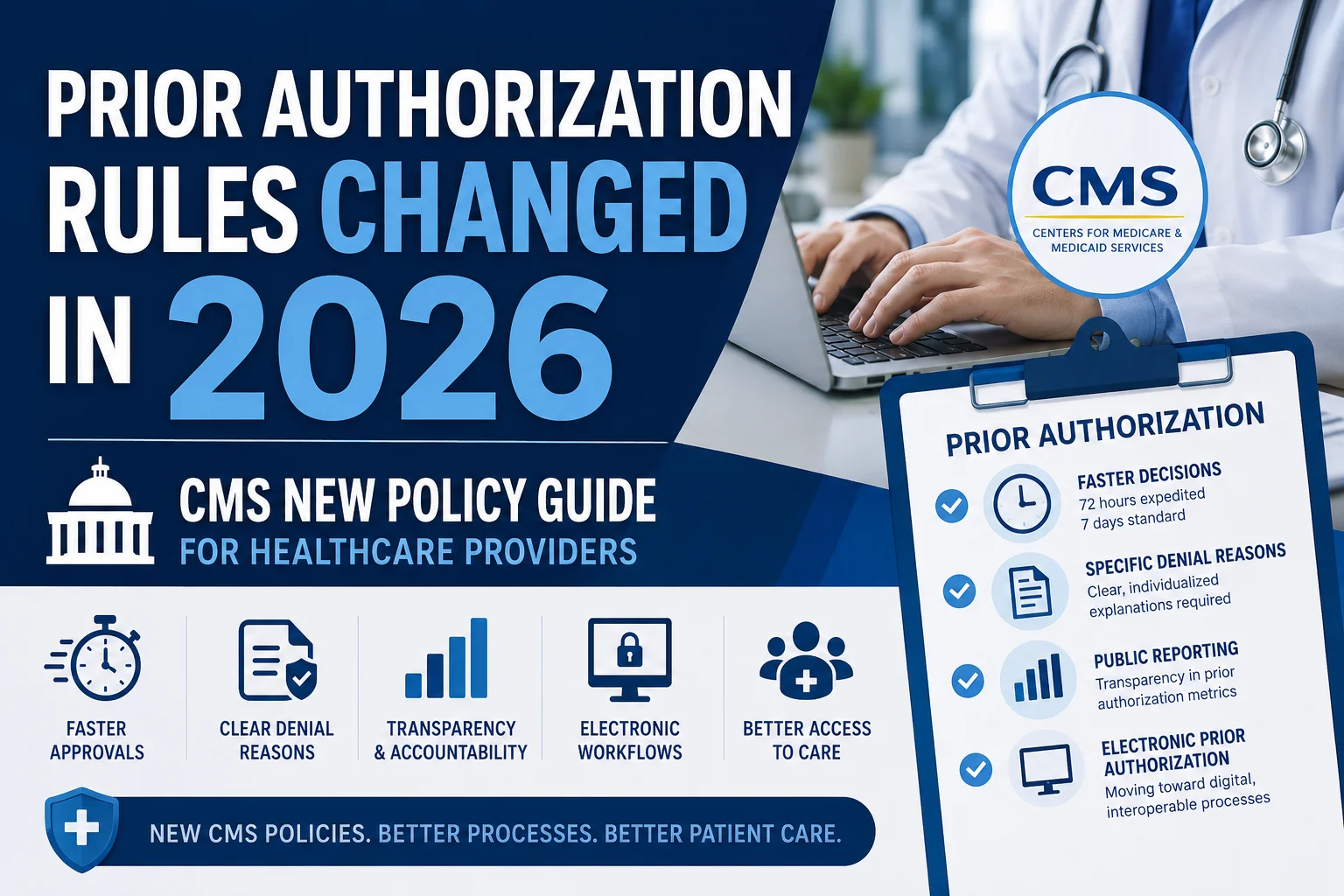
The rules of medical billing are not the same as they were even two or three years ago. Payers have tightened their policies. The CMS Prior Authorization API Rule that went into effect in 2026 added new electronic processing requirements that many practices were not prepared for. Insurance companies are now using automated systems to catch errors faster — and deny claims quicker than ever.
At the same time, staffing shortages in many practices mean billing tasks are being handed off to people who are stretched way too thin. One missed modifier. One wrong code. One day’s delay in filing — and that claim is gone.
“The average healthcare practice loses $50,000 or more annually to preventable billing errors and uncollected revenue.” — Industry data cited by the Medical Group Management Association (MGMA)
The practices that are actually growing their revenue in 2026 are the ones that stopped treating billing as a back-office chore and started treating it as a core part of running a healthy business. Let’s look at exactly where the money is being lost.
Mistake #1: Skipping Insurance Eligibility Verification Before Appointments
This is the one that surprises people the most — because it happens right at the very beginning, before the patient even walks in the door.
Here is what happens all the time: a patient schedules a visit. The front desk assumes their insurance is still active from the last time they came in. The appointment happens. The claim goes out. And then — weeks later — it comes back denied because the patient’s coverage had lapsed, or they switched plans, or your provider is no longer in their network.
Now you are chasing a denial that could have been avoided with a simple two-minute check before the appointment was even confirmed.
What Goes Wrong
- Coverage lapsed and nobody thought to verify it again
- Patient switched to a new employer health plan mid-year
- Provider is no longer in-network with the patient’s updated plan
- Deductible and copay amounts were not verified — patient owes far more than expected and disputes it
The Fix
Verify eligibility for every patient, every single visit — not just new patients. Real-time eligibility checks through your billing system can flag coverage issues before they become denied claims.
At Pro Health Care Advisors, we run real-time insurance eligibility verification as part of every billing workflow — catching coverage problems at scheduling, not three weeks after a claim denial arrives.
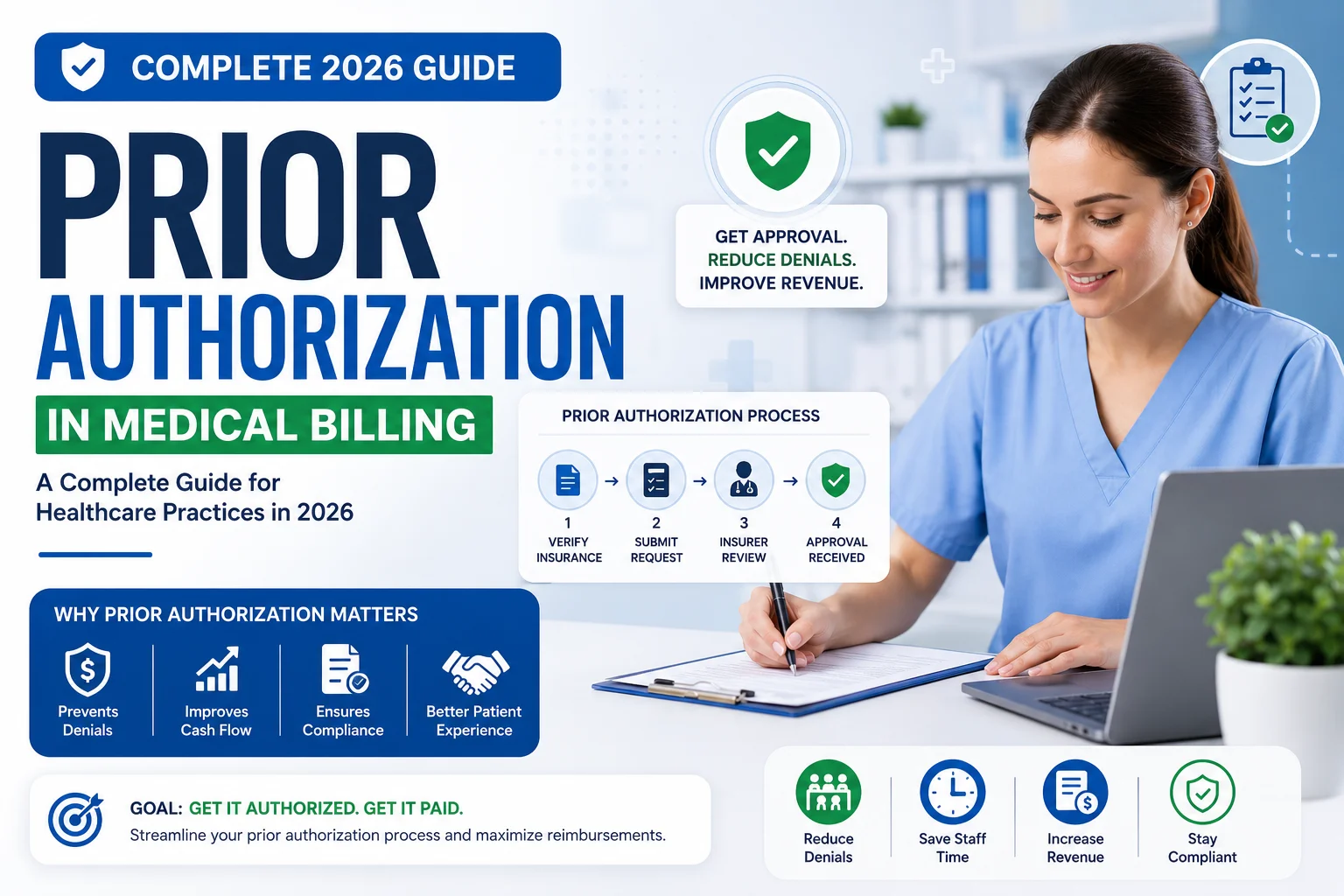
Mistake #2: Missing or Incomplete Prior Authorization
Prior authorization — or prior auth — is the payer’s way of saying “get our approval before you do this.” Surgeries, advanced imaging, specialty referrals, high-cost medications — many of these require a green light from the insurance company before the service happens.
When practices skip this step, or submit the authorization request with incomplete or incorrect information, claims get denied flat out. And unlike a simple coding error you can correct and resubmit, a prior auth denial after the service has already been provided is very hard to reverse. The patient has already been treated. The payer says they never approved it. The practice eats the cost.
With the 2026 CMS Prior Authorization API Rule now requiring electronic processing between payers and providers, there is even less room for manual errors or informal workarounds.
Common Prior Auth Mistakes
- Service was provided before authorization was actually confirmed — not just requested
- Authorization was obtained but the number was not correctly linked to the submitted claim
- Wrong diagnosis code was used on the authorization request
- Authorization expired before the actual date of service
The Fix
Every service requiring prior authorization needs its own dedicated workflow — from initial submission to confirmed approval to proper documentation in the chart. No service moves forward without a confirmed auth number on file, period.
Learn more about our prior authorization management process and how we handle the entire cycle on your behalf.
Mistake #3: Coding Errors — Wrong, Outdated, or Incomplete Codes
Medical coding is the bridge between what happened in the exam room and what actually gets paid. Every diagnosis, every procedure, every service has a specific code assigned to it — ICD-10 for diagnoses, CPT for procedures, HCPCS for supplies and certain services. When those codes are wrong, the claim fails. It really is that simple. And coding errors are consistently among the top reasons claims get denied or come back underpaid.
Types of Coding Errors That Cost Money
- Upcoding — billing for a more expensive service than what was actually provided (this is also a serious compliance and legal risk)
- Downcoding — billing for less than what was done, leaving real money on the table every single time
- Using outdated CPT codes that were deleted or significantly revised in the annual code update
- Missing modifiers that explain a specific clinical circumstance to the payer
- Diagnosis codes that are not specific enough — using a broad, general code when a more precise one is required by the payer
- Linking the wrong diagnosis to the wrong procedure on the claim form
Why This Is Getting More Difficult in 2026
CPT and ICD-10 code sets are updated every single year. On top of that, individual payer policies change separately — sometimes a code that is valid and reimbursable with one payer is flatly denied by another. Without specialty-focused coders who stay current with both the code updates and payer-specific rules, coding errors multiply fast.
The Fix
AAPC-certified coders who specialize in your specific medical specialty. A general coder handling everything from orthopedics to mental health to cardiology to oncology is far more likely to miss the specialty-specific rules that determine whether your claim gets paid.
Our CodeMAXX Services team provides specialty-focused ICD-10, CPT, and HCPCS coding — reducing coding-related denials and making sure every dollar your services deserve actually gets captured.
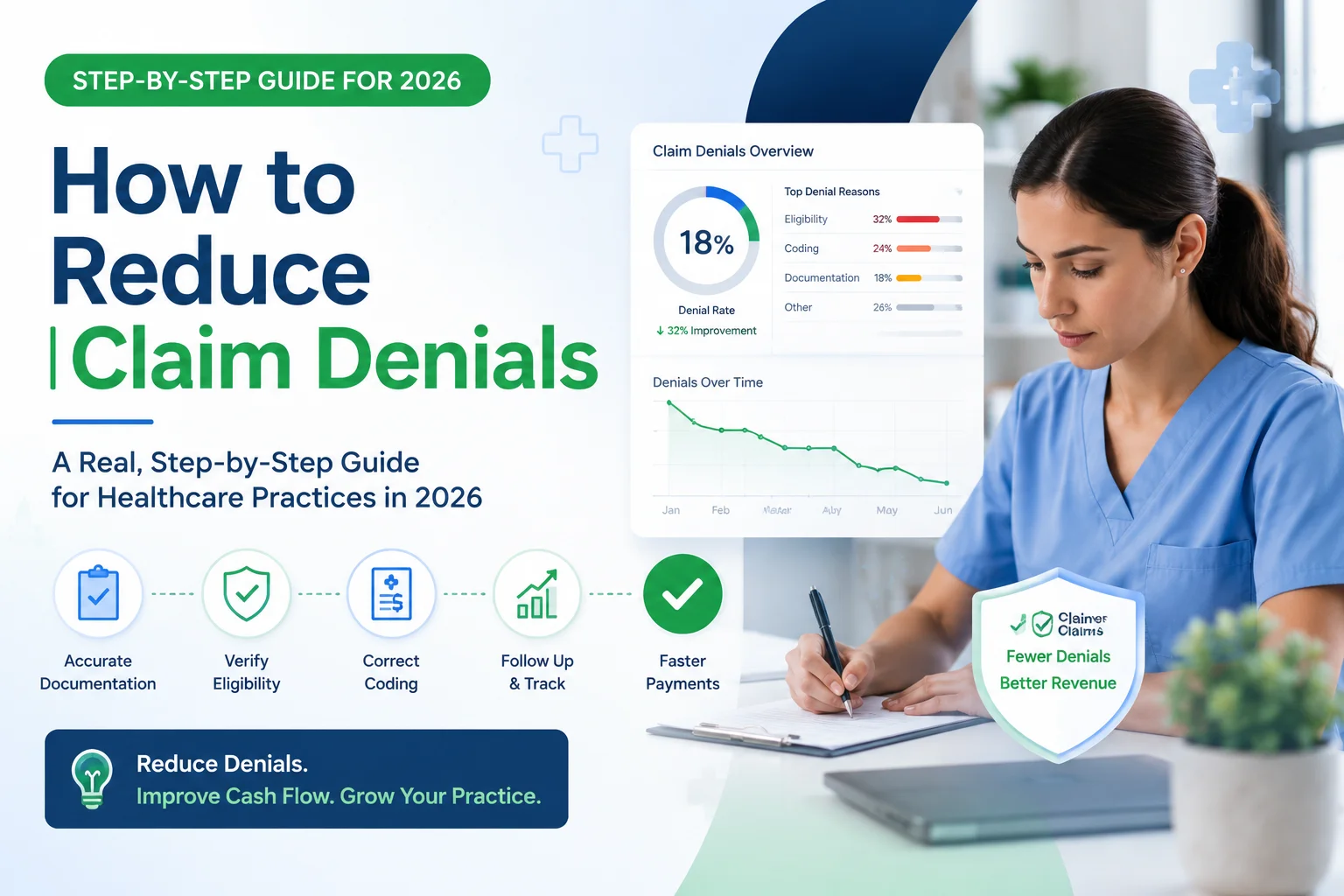
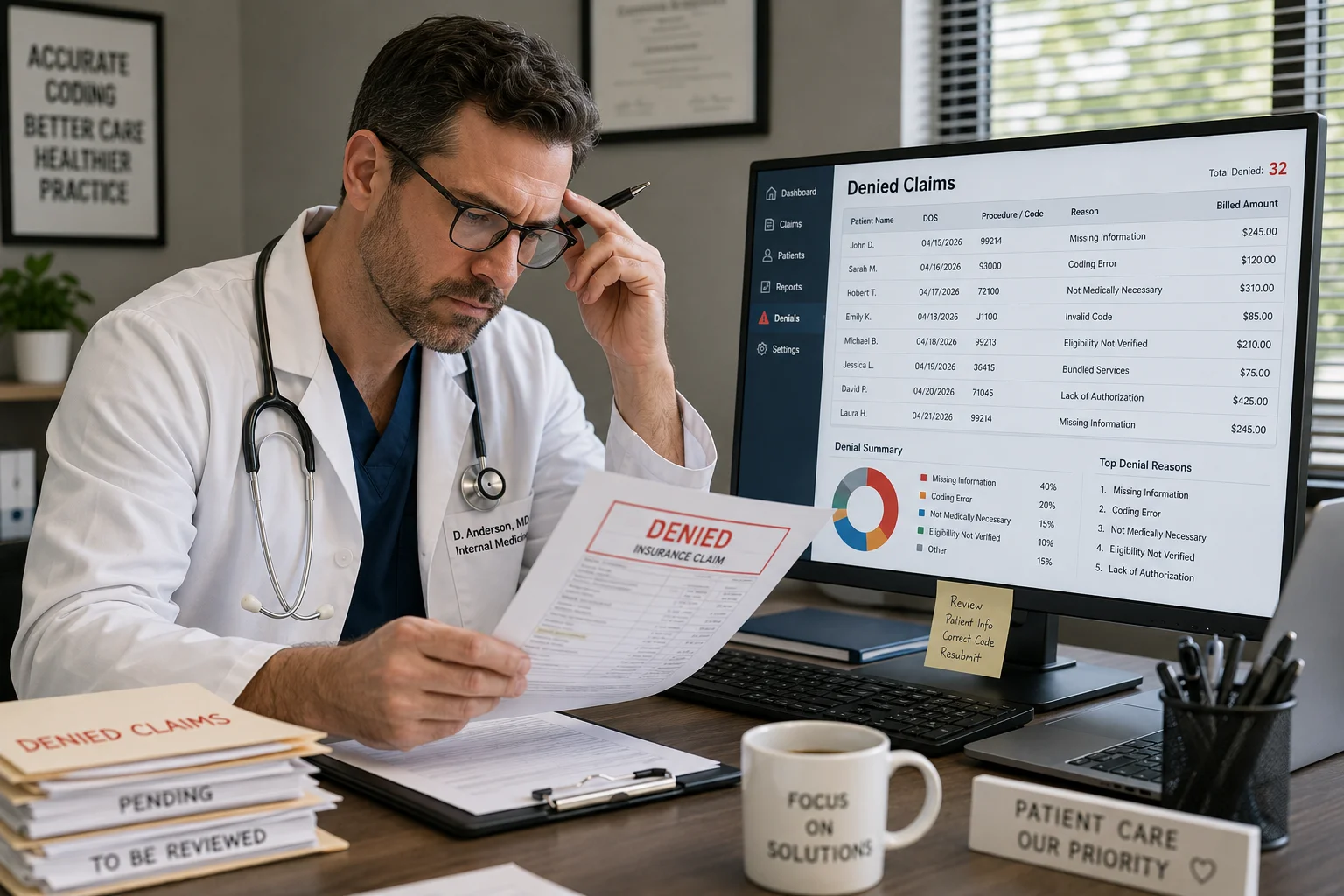
Mistake #4: Slow or Incomplete Denial Management
A denial is not the end of the road. It is actually the beginning — of a second chance to get paid. The problem is that most practices either ignore denials entirely, or take so long to address them that the appeal window closes.
Every insurance company has a hard deadline for submitting appeals. Miss it, and that revenue is simply gone. No appeal accepted. No payment. Nothing — ever.
According to data from the Healthcare Financial Management Association (HFMA), up to 65% of denied claims are never reworked at all — meaning practices are voluntarily walking away from money that could have been recovered with a proper, timely appeal.
Read that again. Sixty-five percent. Practices are not losing that money because they cannot get it back. They are losing it because nobody went back to fight for it.
Why Practices Let Denials Slip
- No dedicated denial management process or person assigned to it
- Staff too busy processing new claims to go back and work old denied ones
- Denial reason codes are not being tracked or analyzed for patterns
- Appeal deadlines are missed because no one is monitoring them
The Fix
Denial management needs to be treated with the same urgency as collections. Every denial gets categorized by reason, worked within a defined timeframe, and tracked through to final resolution — paid or formally closed.
Our Creative Collection Solutions service specializes in accounts receivable recovery — aggressively working denied and aging claims to bring revenue back into your practice that would otherwise stay lost.
Mistake #5: Credentialing Gaps That Block Reimbursement Entirely
Here is a scenario that plays out more often than most people realize.
A new provider joins your practice. Excited to get started, they begin seeing patients right away. Claims go out under their NPI number. Everything looks fine. And then — months later — someone notices the provider was never actually credentialed and enrolled with that payer. Every single claim submitted during that entire period? Not payable. In some cases, any payments that accidentally processed through have to be returned.
Physician credentialing is the formal process of getting a provider enrolled and approved with insurance payers. It takes time — typically 60 to 120 days for commercial payers, and 90-plus days for Medicare and Medicaid in most states. When it is rushed, skipped, or simply forgotten in the chaos of onboarding a new provider, the financial damage can be enormous.
Credentialing Mistakes That Cost Money
- Starting a new provider without confirming active enrollment with key payers first
- CAQH profile that is outdated or has not been re-attested (required every 120 days)
- Missing re-credentialing deadlines with existing payers, causing lapses in coverage
- Incomplete application documentation that causes payer processing to stall for weeks
The Fix
Never let a provider see insurance-covered patients until enrollment is formally confirmed — in writing. Start the credentialing process as early as possible, ideally well before the provider’s first scheduled day.
Our Physician Credentialing service tracks every application, follows up with payers at regular intervals, keeps CAQH profiles current, and makes sure you never lose revenue to a credentialing gap that should not have happened in the first place.
Mistake #6: HIPAA Compliance Failures That Invite Audits
HIPAA compliance is not just a legal checkbox you tick once and forget. A compliance failure can trigger a payer audit — and a payer audit can mean recoupment demands, where payers come back and ask you to return money they already paid, sometimes for claims going back years.
Compliance failures in billing often look subtle on the surface: sending patient data through an unsecured email, not having a signed Business Associate Agreement (BAA) with your billing vendor, or inconsistent clinical documentation that does not properly support the service that was billed.
The HHS Office for Civil Rights (OCR) continues to enforce HIPAA actively in 2026, and payers run their own separate audit programs on top of federal enforcement.
Our HIPAA Compliance service includes BAA management, AES-256 encrypted data handling, restricted PHI access controls, and regular compliance reviews — keeping your practice protected on both the regulatory and payer sides.
Mistake #7: Not Using Electronic Fund Transfer for Faster Payments
This one is less about denials and more about unnecessary delays in getting paid.
Many practices still receive paper checks from insurance companies. Paper checks add days — sometimes full weeks — to your payment cycle. They get lost in the mail. They require manual processing that takes up staff time. And they make payment reconciliation far more complicated than it needs to be.
Electronic Fund Transfer (EFT) connects your practice directly to payer payment systems. When a claim is approved, the payment moves electronically — faster, cleaner, with a complete digital trail that makes reconciliation straightforward.
Learn more about our Electronic Fund Transfer service and how it can accelerate your reimbursement cycle with direct payer connections.
Bonus: RAC Audits Are Increasing — Is Your Practice Ready?
Recovery Audit Contractors — RAC auditors — are third-party companies hired by CMS to identify overpayments in Medicare and Medicaid claims. When a RAC audit flags your practice, you can face significant recoupment demands. You may be forced to return large sums, sometimes for claims that were submitted years ago.
RAC audit activity has increased noticeably in 2026, with particular focus on high-volume specialties including cardiology, oncology, and wound care. If your practice operates in any of these specialties, this is not something to push to the back burner.
For official background on the program, see the CMS Recovery Audit Program overview.
Our MD Audit Shield – RAC service is built specifically to identify compliance risks before auditors do — and to defend your practice confidently if an audit does occur.
What the Numbers Actually Say About Billing Losses in 2026
| Problem | Real Financial Impact |
|---|---|
| 12% national denial rate | $12,000 lost per $100,000 billed |
| 65% of denials never reworked | Permanent, unrecoverable revenue loss |
| Eligibility errors at front desk | Top cause of preventable claim denials |
| Missing prior authorization | Full claim denied, very hard to reverse |
| New provider credentialing gap | All claims during gap period unpayable |
| RAC audit finding | Recoupment demands, sometimes years back |
How Pro Health Care Advisors Fixes Every One of These Problems

We did not build our services around what sounds impressive in a sales pitch. We built them around the specific, real problems described above — because those are the problems that are actually costing practices money right now.
98.5% Clean Claim Rate
Our AAPC-certified billers review every claim before it ever touches a payer — checking codes, modifiers, eligibility status, and prior authorization. That disciplined pre-submission review is why our clean claim rate sits at 98.5%, compared to a national average that hovers around 85–88%.
Less Than 2% Denial Rate
When a claim does come back denied, we work it immediately. Our denial management team categorizes every denial by reason code, files appeals within payer deadline windows, and tracks every case through to final resolution. Nothing falls through the cracks.
Free Revenue Audit — No Strings Attached
Not sure where your money is going? We will tell you — for free. Our revenue audit identifies uncollected revenue, denial patterns, credentialing gaps, and coding issues that are specific to your practice and your specialty.
Request your free revenue audit here — no commitment required.