What Is Medical Billing? The Complete 2026 Guide for Doctors and Practice Managers
You spent years in medical school learning how to help people. Nobody taught you how to get paid for it.
That is not a complaint — it is just reality. Medical education is built around patient care, clinical reasoning, and treatment. The financial side of running a practice? That gets about three hours in most residency programs, if it gets mentioned at all.
So most doctors enter practice with a rough idea that billing involves submitting something to insurance companies and eventually money shows up in the bank account. They hire someone to handle it, trust that it is working, and focus on patients.
And then the denial rate climbs. The accounts receivable ages past 90 days. Revenue that should have come in three months ago is still sitting in limbo. And nobody can clearly explain why.
If you have ever been in that situation — or you just want to understand what is actually happening behind the scenes in your practice — this guide is for you.
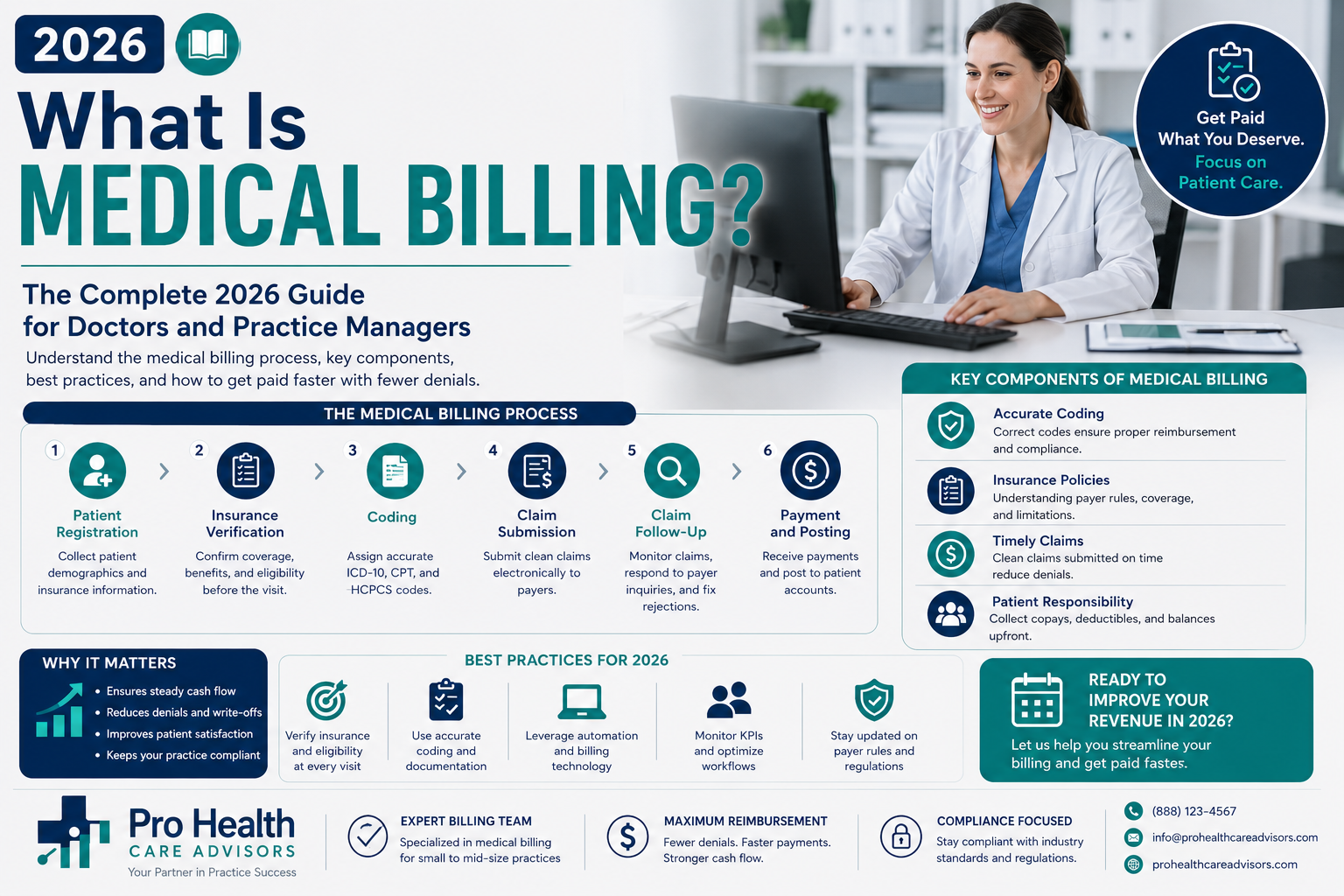
What is medical billing? It is the complete financial engine of your practice. It is a structured, 10-step process that begins the moment a patient schedules an appointment and ends when every dollar owed to your practice has been collected. Understanding it is not optional. Not if you want your practice to stay financially healthy.
Let us go through it from the beginning.
What Is Medical Billing — The Plain-English Definition
Medical billing is the process of submitting claims to insurance companies and collecting payment for healthcare services that a provider has already delivered.
Think of it this way. A doctor sees fifty patients in a week. For each of those visits, the doctor does clinical work — examines, diagnoses, treats, prescribes. But the doctor does not hand each patient a receipt and ask for payment on the way out. Instead, the details of each visit — what was done, why it was done, and who the patient is — go through a structured process that eventually results in payment from the patient’s insurance company, from the patient themselves, or from both.
That entire process is what is medical billing.
Here is a version for someone who has never heard of insurance claims:
Imagine you run a small shop. Every time a customer buys something, instead of paying you directly, they give you their insurance card. You then have to fill out a detailed form — exactly what they bought, why they needed it, and what their insurance plan covers — and send it to their insurance company. The insurance company reviews your form, maybe asks questions, then sends you a check a few weeks later. Sometimes they say your form was wrong and send it back. That is medical billing. Except the stakes are much higher and the forms are much more complicated.
In the United States, medical billing is governed by thousands of rules — from federal programs like Medicare and Medicaid, from private insurance companies like Blue Cross Blue Shield, United Healthcare, Aetna, and Cigna, from state Medicaid programs, and from compliance regulations like HIPAA.
According to the American Medical Association, physicians and their staff spend an estimated 14.5 hours per week just on prior authorizations — one single piece of the billing puzzle. Altogether, poor billing practices cost US providers an estimated $125 billion annually in revenue that is either never claimed or never recovered after denial.
That number exists because what is medical billing — and how to do it correctly — is genuinely complicated. Let us break it down into the ten steps that make up the complete process.
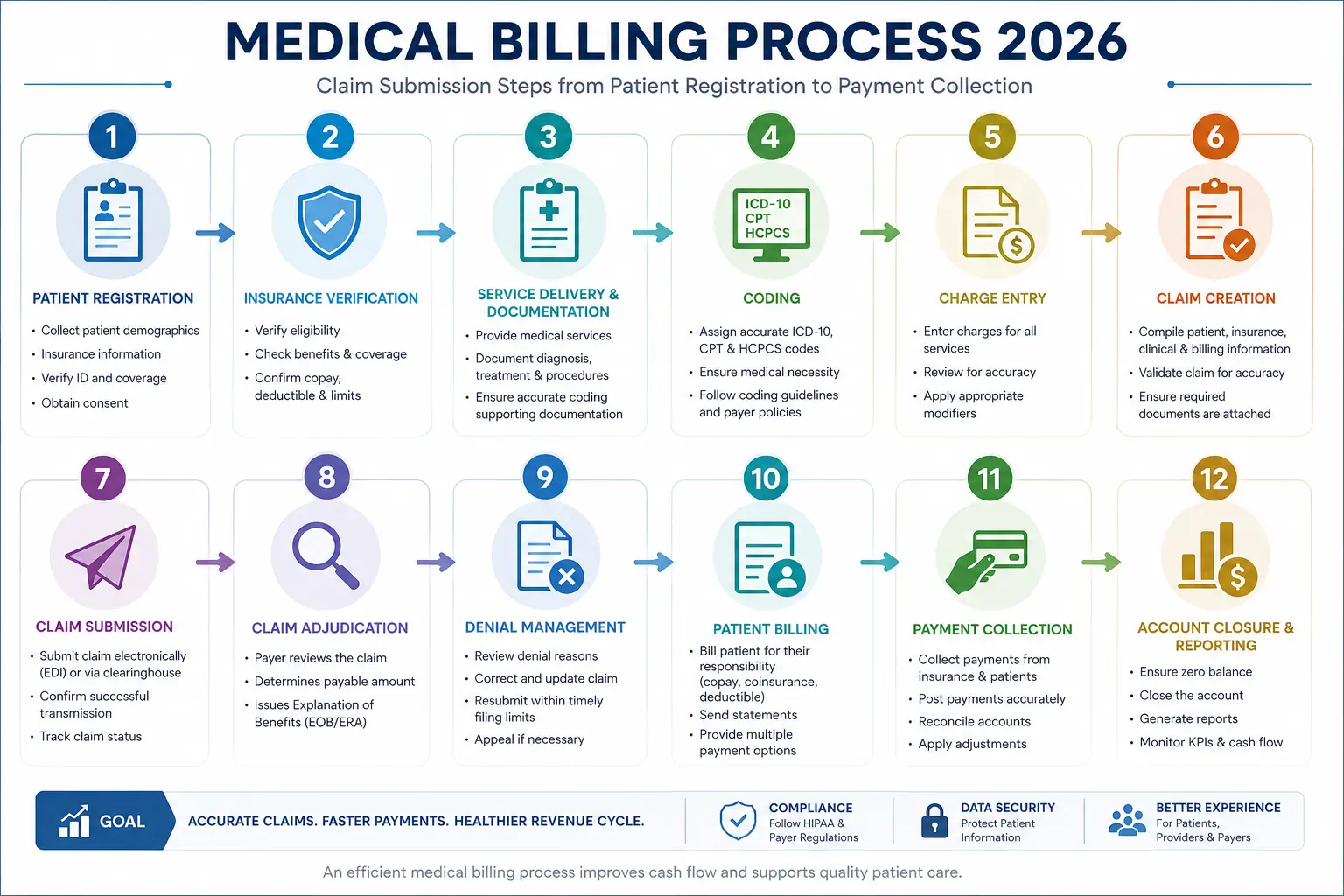
What Is Medical Billing — The 10-Step Process Explained
Every dollar your practice earns goes through ten steps. Each step, done correctly, moves the claim forward. Each step done poorly — or skipped — creates a problem that costs time and money to fix downstream.
Step 1: Patient Registration and Scheduling
Medical billing does not start when a patient walks in the door. It starts when they call to make an appointment.
At registration, your front desk collects — and verifies — the information that every subsequent step depends on:
- Full legal name (exactly matching insurance records)
- Date of birth
- Address and contact information
- Insurance carrier, plan name, group number, and member ID
- Primary care physician information if required by the plan
- Referral information if applicable
- Secondary insurance if the patient has more than one plan
An error here — a transposed number in the policy ID, a name spelled differently from what the insurer has on file, a wrong date of birth — creates a claim rejection at submission, weeks later. The information collected in the first two minutes of the patient relationship determines whether the last step (getting paid) goes smoothly or gets stuck.
What is medical billing’s most preventable failure? Patient registration errors. According to HFMA research, eligibility and patient information issues account for approximately 22% of all preventable claim denials.
Step 2: Insurance Eligibility Verification
Before the patient ever sits in the exam room, their insurance coverage must be verified — not assumed.
Eligibility verification confirms:
- That the patient’s coverage is currently active
- What the patient’s deductible is, and how much has been met
- What the copay and coinsurance amounts are
- Whether the specific service being scheduled requires prior authorization
- Whether the treating provider is in-network with the patient’s plan
- Whether mental health or behavioral health benefits are handled by a separate administrator (a “carve-out”)
In 2026, with high-deductible health plans covering more than 57% of employer-sponsored insured workers, patient financial responsibility has become a significant portion of practice revenue. A patient who arrives for a visit with a $3,000 deductible they have not yet met owes the practice the full amount for that visit — but only if the practice knows this beforehand and collects it.
Eligibility verification is now done electronically, in real time, through clearinghouses and payer portals. Running this check the day before every appointment is the standard that prevents the majority of eligibility-related denials.
Step 3: Prior Authorization
Some services require the insurance company’s formal approval before they are rendered. This is called prior authorization — and getting it wrong is one of the most frustrating billing failures a practice can experience.
The service gets done. The care was clinically appropriate. The patient needed it. But nobody got the authorization number first. And now the claim is denied.
In 2026, the Centers for Medicare and Medicaid Services introduced a new electronic prior authorization (ePA) mandate requiring payers to process urgent requests within 72 hours and standard requests within 7 days. This has sped up authorizations significantly for participating practices — but only if the practice is using ePA-compatible systems.
Services that commonly require prior authorization in 2026:
- Advanced imaging (MRI, CT, PET scans)
- Specialty medications and infusion therapy
- Elective surgical procedures
- Physical, occupational, and speech therapy beyond initial sessions
- Mental health services beyond a plan’s initial approved sessions
- Certain diagnostic tests and genetic testing
The fix is straightforward: check authorization requirements for every scheduled procedure before the appointment, track approval numbers, track expiration dates, and confirm that the service performed matches exactly what was authorized.
Step 4: Medical Coding
After the patient is seen and the provider documents the visit, a medical coder converts that clinical documentation into standardized numeric codes.
This step is the technical heart of what is medical billing — and it is the bridge between clinical care and financial reimbursement.
Two main code systems drive this process:
ICD-10-CM codes — diagnosis codes that tell the insurance company what was wrong with the patient. There are over 72,000 active ICD-10-CM codes. Every condition, symptom, injury, and reason for the visit has a specific code. As of October 2025, CMS added 487 new diagnosis codes and revised 38 existing ones — changes that practices must implement to avoid denials.
CPT codes — procedure codes that tell the insurance company what the provider did. The American Medical Association owns and updates CPT codes annually. The 2026 update includes 288 new codes, 46 revisions, and 84 deletions — one of the most substantial coding updates in recent years.
HCPCS Level II codes — cover supplies, equipment, drugs, and non-physician services not captured by CPT codes.
Coding accuracy is everything in this step. The wrong CPT code for a service billed. A diagnosis code that is too vague to support medical necessity. A missing modifier that the payer requires. Any of these sends the claim toward denial — and creates the compliance risk that OIG audit programs and Recovery Audit Contractors actively monitor.
Step 5: Charge Capture
After coding, the charges are entered into the practice management system. This step ensures that everything the provider did gets documented as a billable charge — and that nothing falls through the cracks.
Practices with poor charge capture systems lose revenue not because claims are denied, but because services were never billed in the first place. A procedure performed, a supply used, an additional service provided — and nobody wrote it down in a way that made it into the claim.
Charge capture audits, where a practice reviews clinical documentation against billing records, regularly surface uncaptured revenue in practices of every size.
Step 6: Claim Building and Scrubbing
With codes and charges in place, the biller builds the claim — an electronic form that packages all of the patient, provider, and service information into a format the payer can process.
Professional claims (for physician services) use the CMS-1500 form. Institutional claims (for hospitals and facilities) use the UB-04 form. Both are submitted electronically in standardized HIPAA formats.
Before any claim goes out, it goes through claim scrubbing — a review process that checks every field for errors, validates code combinations, verifies that required modifiers are present, and confirms that the claim meets each payer’s specific formatting rules.
In 2026, AI-powered claim scrubbers review hundreds of fields in seconds, flagging combinations that have historically been denied by specific payers. According to industry benchmarks, practices using AI-assisted claim scrubbing reduce denial rates by 15–30% compared to practices using manual review alone.
The standard that every practice should aim for: zero claims should go out without scrubbing.
Step 7: Claim Submission
The scrubbed claim travels from the practice management system through an electronic clearinghouse — a service that acts as an intermediary between practices and payers, checking claims for formatting errors before forwarding them to the correct insurance company.
Major clearinghouses in 2026 include Availity, Change Healthcare, and Office Ally. Most practice management systems have clearinghouse integration built in.
Claims submitted electronically to Medicare are typically adjudicated within 14 to 30 days. Commercial payer timelines vary — most aim for 30 days, but complex claims or claims requiring documentation review can take 45 to 60 days.
Timely filing rules apply from this step forward. Medicare requires claims within 12 months of the date of service. Most commercial payers require submission within 90 to 180 days. After the deadline passes, the claim cannot be recovered — that revenue is gone permanently.
Step 8: Payer Adjudication — What Happens on the Insurance Side
Once the payer receives the claim, they run it through their own adjudication process — a series of automated and sometimes manual checks that determine:
- Whether the patient was covered on the date of service
- Whether the provider is credentialed and in-network
- Whether the service was medically necessary based on the diagnosis
- Whether the code combinations are valid under their coverage policies
- Whether prior authorization was obtained if required
- How much to pay based on the contracted rate
The result is an Explanation of Benefits (EOB) or an Electronic Remittance Advice (ERA) — a document that tells you whether the claim was paid, partially paid, or denied, and why.
Reading and understanding denial reason codes on EOBs is a core skill for any billing team. One experienced billing specialist once said something that sticks with our team: the reason code on a denial is frequently not the actual cause of the denial. Payers routinely return generic codes — “not medically necessary,” “insufficient documentation” — that require experience to decode into the actual fix.
Step 9: Payment Posting and Denial Management
When payment arrives — electronically as an ERA or by paper check — it gets posted to the patient’s account. The payment posting process reconciles what was paid against what was billed and identifies:
- Contractual adjustments (the difference between what was charged and the contracted rate)
- Patient responsibility amounts (copay, deductible, coinsurance)
- Underpayments — when the payer paid less than the contracted rate
- Denied line items — specific services on the claim that were not paid
Denial management is what happens next when a claim or line item is denied. This is not a passive process. Claims that sit in denied status without action are lost revenue. The practice that wins on billing treats every denial as a problem to solve:
- What was the denial reason?
- Is this a fixable error (wrong code, missing modifier) or a medical necessity dispute?
- Can it be corrected and resubmitted, or does it need a formal appeal?
- What documentation needs to accompany the appeal?
According to industry data, 57% of denied Medicare Advantage claims are ultimately overturned on appeal. That means more than half of the money payers initially say no to can be recovered — if someone does the work.
Step 10: Patient Billing and Final Collections
After insurance has paid its portion, the patient receives a statement for their remaining responsibility — copay, deductible, coinsurance, or any non-covered services.
In 2026, patient collections have become a higher priority for every practice because high-deductible plans have shifted more financial responsibility to patients. The Medicare Part B deductible alone rose to approximately $283 in 2026 — meaning more patients owe more out of pocket before coverage kicks in.
Best practices for patient billing in 2026:
- Collect known copays at the time of service — not after the claim is processed
- Provide cost estimates before the visit for scheduled procedures
- Offer online payment options — practices that offer digital payment collect faster
- Set clear financial policies and communicate them at intake
- Use a patient-friendly billing statement that explains what insurance paid and what remains
According to CFPB data, around 100 million Americans carry over $220 billion in total medical debt. The practices that minimize their contribution to that problem — through clear upfront communication and easy payment options — also tend to collect more efficiently.
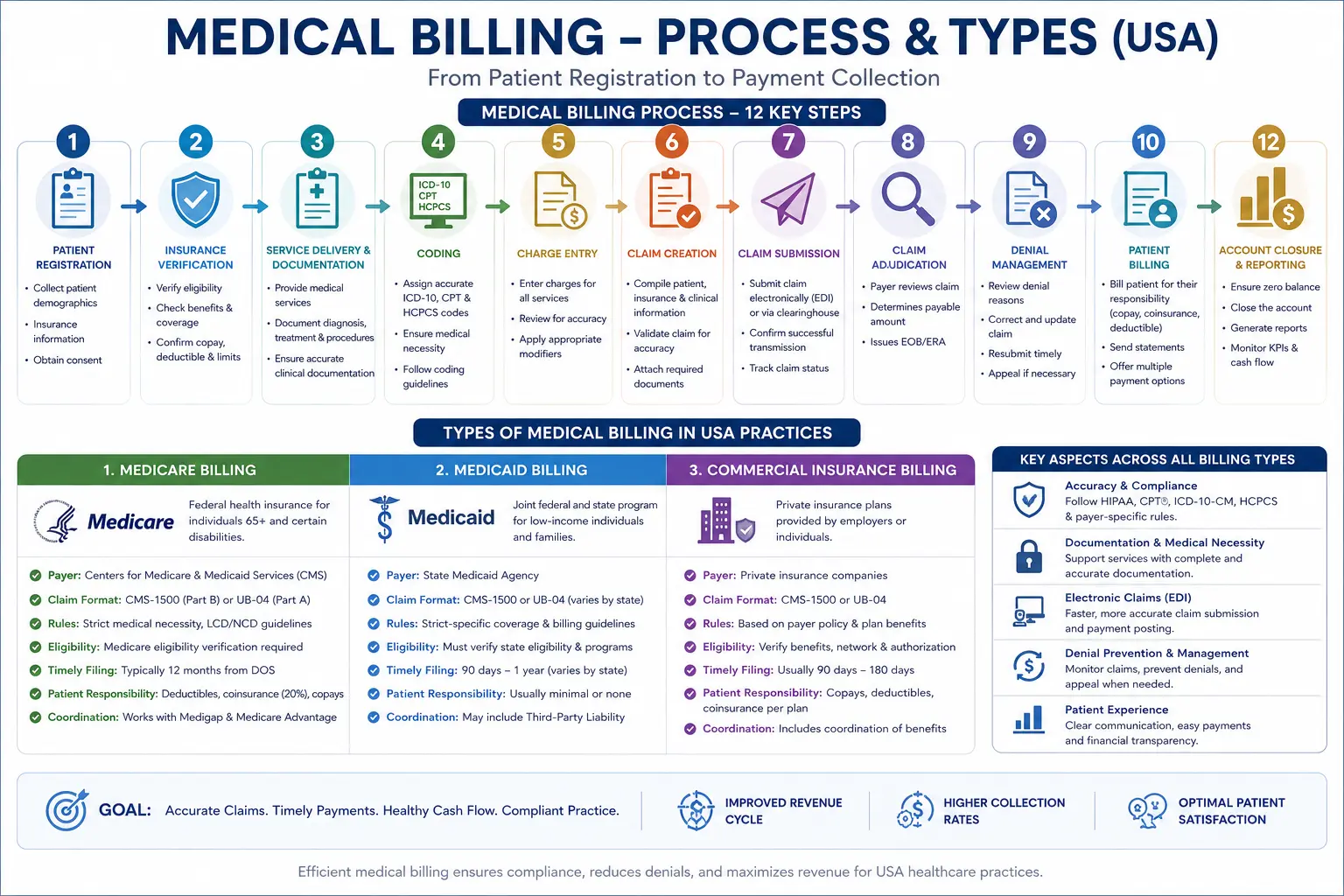
What Is Medical Billing — The Different Types
Not all billing is the same. What is medical billing in a Medicare context is very different from what is medical billing for a commercial insurance plan — and both are different from self-pay or workers’ compensation billing.
Medicare Billing
Medicare is the federal health insurance program primarily for people 65 and older, and for certain people with disabilities. As of 2026, Medicare covers approximately 65 million Americans.
Medicare billing follows CMS rules very precisely. Reimbursement rates are set by the Medicare Physician Fee Schedule — a published list of what Medicare pays for every CPT code. CMS implemented a 2.5% reduction to work RVUs across nearly 7,700 codes in 2026, making revenue optimization more important than ever for procedure-heavy practices.
Key Medicare billing rules every practice must know:
- All Medicare claims must be submitted electronically (with limited exceptions)
- Medicare has a 12-month timely filing deadline
- ABN (Advance Beneficiary Notice) forms must be obtained when a service may not be covered
- Medicare Secondary Payer rules apply when a patient has other coverage
- PECOS enrollment must be current for every provider billing Medicare
Medicare Advantage (Part C) Billing
Medicare Advantage plans are private insurance plans that deliver Medicare benefits. In 2026, Medicare Advantage covers nearly half of all Medicare beneficiaries. Billing Medicare Advantage means billing the private plan — not traditional Medicare — and each plan has its own authorization requirements, network rules, and claim submission protocols.
Medicare Advantage initial denial rates averaged 15.7% in recent reporting — higher than traditional Medicare. Understanding the specific rules of each Medicare Advantage plan in your payer mix is essential for clean claim submission.
Medicaid Billing
Medicaid is the joint federal-state program covering low-income individuals and families. Every state runs its own Medicaid program with its own billing portal, reimbursement rates, and coverage rules. Medicaid billing in Georgia is different from Medicaid billing in Florida or Texas — the code sets are the same, but the administrative requirements differ significantly.
Medicaid managed care organizations (MCOs) — plans like UnitedHealthcare Community Plan, Molina Healthcare, Centene, and Amerigroup — further complicate the landscape, because each MCO has its own claim submission portal and authorization rules even within the same state.
Commercial Insurance Billing
Commercial insurance covers most working-age Americans through employer-sponsored plans. Major commercial payers include Blue Cross Blue Shield (in various state-specific organizations), UnitedHealthcare, Aetna, Cigna, and Humana.
Commercial billing follows contracted rates — amounts your practice has agreed to accept through participation agreements with each payer. Knowing your contracted rates, verifying that payers are paying correctly, and identifying underpayments are all critical components of commercial billing management.
Self-Pay Billing
Self-pay patients have no insurance — or are being seen for services not covered by their plan. Self-pay billing requires clear upfront communication about costs, sliding scale fee structures where applicable, and a direct patient billing process with clear payment options.
Workers’ Compensation Billing
Workers’ compensation covers medical expenses for employees injured on the job. Billing workers’ comp is handled through state-specific carriers, uses different claim forms than standard insurance billing, and has its own documentation requirements and reimbursement schedules.
What Is Medical Billing — In-House vs Outsourced
One of the most important decisions a practice makes is whether to handle billing in-house or to outsource it to a professional billing service.
Both approaches can work. But the data shows a clear performance difference.
According to MGMA 2024 data, practices outsourcing billing achieve an average 94.8% net collection rate versus 89.6% for in-house operations. That 5.2-percentage-point gap represents significant real money at any billing volume.
In-House Billing:
- Full control over the process and performance data
- Direct management of billing staff
- Requires ongoing investment in training, software, and compliance updates
- Staff salaries in 2026 range from $55,000 to $75,000 per biller, plus 20–30% in benefits and payroll taxes
- High turnover rates (40%+) in billing roles create workflow disruptions
- One person out sick can halt the entire revenue cycle
Outsourced Billing:
- Service fee typically 5–8% of collections — often less expensive than in-house staff fully loaded
- Access to specialized expertise in your payer mix and specialty
- Built-in redundancy — no single point of failure
- Continuous training and compliance updates handled by the billing company
- Access to technology (claim scrubbers, eligibility tools, denial analytics) without capital investment
- For practices under 5 providers, outsourcing almost always produces better financial results
For small and individual practices — the ones most likely to be affected by a single billing staff member’s vacation, sick day, or resignation — outsourcing provides stability that in-house billing cannot match at the same cost.
Our medical billing and practice management service handles the complete billing cycle for small and individual practices across the United States — from eligibility verification through payment posting and denial management.
What Is Medical Billing — Key Terms Every Doctor Should Know
If you review your billing reports or sit in on billing meetings, these are the terms you will encounter. Understanding them gives you the ability to ask the right questions and identify problems early.
| Term | What It Means |
|---|---|
| Clean Claim | A claim submitted with no errors — ready to be adjudicated without additional information |
| First-Pass Acceptance Rate | The percentage of claims paid on first submission without correction or appeal |
| Days in A/R | How long it takes, on average, to collect payment after a service is rendered |
| Denial Rate | The percentage of submitted claims that are rejected by the payer |
| Net Collection Rate | The percentage of collectible revenue that is actually collected |
| EOB / ERA | Explanation of Benefits / Electronic Remittance Advice — the payer’s response to a claim |
| Clearinghouse | An intermediary that routes claims from practices to payers electronically |
| Prior Authorization | Payer approval required before certain services are rendered |
| Timely Filing | The deadline by which a claim must be submitted |
| Accounts Receivable (A/R) | Money owed to the practice for services already rendered |
| Superbill | A detailed receipt listing all services, codes, and charges for a patient visit |
| Write-Off | Revenue that cannot be collected — either contractual adjustments or uncollectible debt |
| Credentialing | The process of enrolling a provider with insurance payers |
| PECOS | CMS’s online enrollment system for Medicare providers |
| NPI | National Provider Identifier — the unique number assigned to every healthcare provider |
What Is Medical Billing — Common Problems and Proven Fixes
Understanding what is medical billing is one thing. Knowing where it commonly breaks down in real practices is what allows you to fix the right things.
Problem: High denial rate (above 5%) Most denial rates above 5% trace to a small number of root causes — eligibility errors, coding issues, missing authorizations, or timely filing misses. A structured denial root-cause analysis, done monthly, identifies which category is driving the problem and what process change fixes it.
Problem: Days in A/R over 45 days When accounts receivable ages past 45 days consistently, it usually means claims are sitting without follow-up, or denials are not being worked. Practices with healthy A/R review the aging report weekly — not monthly — and escalate any claim past 45 days to active follow-up.
Problem: Net collection rate below 95% A net collection rate below 95% means the practice is not collecting a significant share of what it is legally entitled to collect. The gap is usually a combination of uncollected patient responsibility, unworked denials, and timely filing lapses. Each gap has a specific fix.
Problem: Credentialing lapses causing denials A provider whose credentialing has lapsed with even one payer generates automatic denials for every claim submitted under that NPI to that payer — and those denials accumulate for weeks before anyone finds the cause. Our physician credentialing service tracks every expiration date and initiates renewals 120 days in advance so this never happens.
Problem: RAC audit exposure Recovery Audit Contractors review claims patterns for anomalies. Practices that bill consistently outside the statistical norms for their specialty and region attract audit attention. Understanding what is medical billing compliance — and monitoring your own patterns — is the foundation of audit protection. Our MD Audit Shield program does this monitoring proactively for small practices.
The Medical Billing Health Checklist — Where Does Your Practice Stand?
Use this checklist to evaluate your current billing performance. Any “No” answer identifies an area costing your practice revenue.
Front-End (Before the Visit):
- Insurance eligibility verified for every patient before every visit
- Prior authorization confirmed before every scheduled procedure requiring it
- Patient demographic information verified against payer records at registration
- Copays collected at time of service — not billed later
Coding and Charge Capture:
- All coders are certified and completed 2026 CPT/ICD-10 update training
- Superbills updated with current year codes every January
- Charge capture audits conducted quarterly to find unbilled services
- Specific ICD-10 codes used — not defaulting to unspecified codes
Claims Submission:
- All claims submitted within 14 days of date of service
- All claims scrubbed before submission
- Timely filing deadlines tracked for every payer in the mix
Denial Management:
- Denial rate reviewed monthly — target below 5%
- Root cause analysis done on denials — not just individual claim fixes
- Every denial appealed within 30 days of denial date
- No claims aging past 90 days without active follow-up
Provider Credentialing:
- All provider credentialing current with all active payers
- Recredentialing calendar maintained with 180/90/60-day advance alerts
- No new provider billing insurance before written confirmation of effective date
Overall Performance:
- First-pass acceptance rate above 92%
- Days in A/R below 35 days
- Net collection rate above 95%
- HIPAA compliance training current for all billing staff
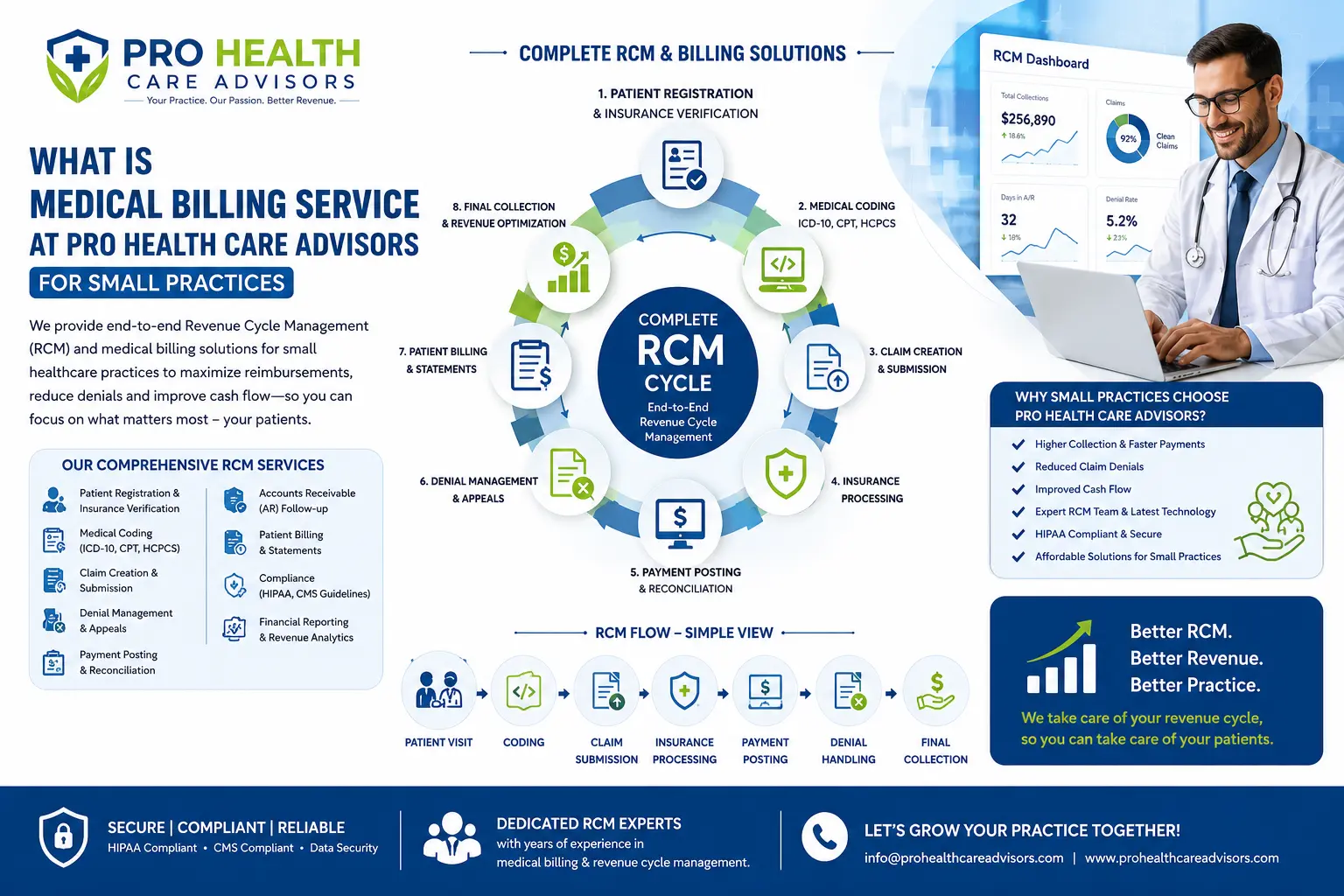
What Is Medical Billing Done Right — How Pro Health Care Advisors Helps
Understanding what is medical billing is the first step. Having a system that executes every one of those ten steps correctly — every day, for every claim — is the difference between a practice that thrives and one that constantly chases its own revenue.
At Pro Health Care Advisors, we serve small and individual medical practices across the United States. We know that when you are a three-physician family practice or a solo psychiatrist in private practice, you do not have a billing department with five specialists, a compliance officer, and a denial management team. You have one or two people doing their best with a process that is genuinely complex.
Here is what we bring to that situation:
Complete billing cycle management: Our medical billing service handles all ten steps — from eligibility verification before the visit through payment posting and patient billing after it. One point of contact. One accountable team. No steps falling through the cracks.
Accurate coding through CodeMAXX: Our CodeMAXX medical coding service validates every CPT and ICD-10 code combination before submission — catching errors at the source, not after they generate denials.
Physician credentialing that never lapses: Our credentialing service tracks every provider’s enrollment with every payer, initiates recredentialing 120 days before deadlines, and ensures no claim goes out under a lapsed enrollment.
HIPAA compliance as standard: Everything we do operates within HIPAA compliance standards — encrypted data, business associate agreements, access controls, and ongoing staff training.
RAC audit protection: Through our MD Audit Shield program, we monitor your billing patterns for the statistical anomalies that attract CMS audit attention — and help you correct them before an auditor finds them first.
EFT setup: We help practices set up Electronic Fund Transfer with all payers so payments arrive electronically, post automatically, and never sit in a paper check pile waiting to be processed.
Contact our team today for a free billing review. We will show you exactly what is medical billing doing — and not doing — in your practice right now, and what it would take to fix it.
Frequently Asked Questions — What Is Medical Billing
Q: What is medical billing in simple terms?
A: Medical billing is the process of getting paid for healthcare services. After a doctor sees a patient, a biller takes the documentation of that visit, codes the services using standardized codes, submits a claim to the patient’s insurance company, and follows up until the practice receives payment. It is the financial bridge between the care a provider delivers and the money the practice collects for delivering it.
Q: What is medical billing vs medical coding?
A: Medical coding is the step that translates clinical documentation into standardized codes — ICD-10 codes for diagnoses and CPT codes for procedures. Medical billing takes those codes and uses them to submit and collect payment. Coding comes first. Billing uses the codes to get paid. Both are essential parts of the revenue cycle, but they are distinct roles with different skills. For a full breakdown, see our medical billing vs medical coding guide.
Q: How long does the medical billing process take?
A: Clean electronic claims submitted to Medicare are typically adjudicated within 14 to 30 days. Commercial payers take 15 to 45 days on average. Claims that require prior authorization documentation, medical necessity review, or appeals can take 60 to 120 days. The timeline also depends on how quickly the practice identifies and works denials. Practices with active denial management collect faster than those that let denials age.
Q: What is the difference between medical billing and revenue cycle management?
A: Medical billing refers specifically to the claim submission and collection process. Revenue cycle management (RCM) is broader — it includes everything from patient scheduling and registration through final payment resolution, plus analytics, contract management, and compliance oversight. Medical billing is the core of RCM, but RCM includes strategic oversight of the entire financial lifecycle of a patient encounter.
Q: What is a clean claim in medical billing?
A: A clean claim is one that is submitted with no errors — correct patient information, valid codes, appropriate modifiers, complete documentation, and compliance with all payer-specific requirements — and that can be adjudicated without the payer needing additional information. The target for any practice should be a first-pass clean claim rate of 95% or higher. Every claim that is not clean on first submission costs money to fix.
Q: What causes most medical billing denials?
A: According to industry research, the most common causes of medical billing denials are eligibility errors (wrong or inactive coverage on the date of service), prior authorization failures (service performed without required approval), coding errors (wrong CPT or ICD-10 code, missing modifier), and missing or incomplete documentation. The vast majority of these are preventable with proper front-end verification and coding quality controls. For a complete breakdown, see our guide on top medical claim denial reasons.
Q: What is medical billing compliance and why does it matter?
A: Medical billing compliance means following all applicable rules — from CMS, from payers, from HIPAA, and from federal anti-fraud statutes — in how you submit, document, and collect for healthcare services. Non-compliance can result in claim denials, overpayment demands, exclusion from Medicare, and in serious cases, civil or criminal penalties. The OIG Compliance Guidance outlines what a compliant billing program looks like. Compliance is not optional — it is the framework within which all billing happens.
Q: Should a small practice outsource medical billing or keep it in-house?
A: For most practices with fewer than 5 providers, outsourcing produces better financial results at lower total cost than in-house billing. In-house billing requires salaries of $55,000–$75,000 per biller plus benefits, ongoing software costs, and management overhead — and is vulnerable to turnover and single points of failure. Outsourced billing costs 5–8% of collections, includes built-in expertise and redundancy, and statistically produces higher net collection rates. The MGMA reports outsourced billing practices achieve an average 94.8% net collection rate versus 89.6% for in-house operations. Contact us for a free billing review to see which approach makes sense for your specific practice.